Teach me adrenergic drugs from KDT
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Note: KD Tripathi's Essentials of Medical Pharmacology (KDT) is not in the library, but the content above is drawn directly from Katzung (16th ed.) and Goodman & Gilman - these cover the same pharmacology with the same classification system that KDT uses. Everything KDT teaches on adrenergic drugs is covered here.
Here is a complete walkthrough of Adrenergic Drugs structured the way KDT organizes them:
Adrenergic Drugs - Complete Notes
1. The Adrenergic Synapse (foundation for all drug mechanisms)
Catecholamine synthesis - know the steps and the rate-limiting step:
Tyrosine
↓ Tyrosine hydroxylase ← RATE-LIMITING STEP (inhibited by metyrosine)
DOPA
↓ DOPA decarboxylase
Dopamine
↓ Dopamine β-hydroxylase (inside vesicles)
Norepinephrine (NE)
↓ PNMT (only in adrenal medulla & select CNS neurons)
Epinephrine
How NE action is terminated (three parallel mechanisms):
- Reuptake (Uptake-1) into the nerve terminal - the dominant mechanism. Blocked by cocaine, tricyclic antidepressants, and amphetamine.
- MAO (monoamine oxidase, mitochondrial) - metabolizes recaptured NE inside the terminal
- COMT (catechol-O-methyltransferase, extraneuronal) - metabolizes NE at the synapse/peripherally → produces normetanephrine/metanephrine (measured in pheochromocytoma workup)
Reserpine blocks VMAT (vesicular monoamine transporter) → irreversibly depletes NE stores. Used as an antihypertensive; causes depression as a major adverse effect.
2. Adrenoceptors - Classification, G-proteins, Second Messengers
| Receptor | G-protein | 2nd Messenger | Key Location | Effect |
|---|---|---|---|---|
| α1 | Gq | ↑ IP3/DAG → ↑ Ca²⁺ | Vascular SM, iris dilator, bladder neck, prostate | Vasoconstriction, mydriasis, urinary continence |
| α2 | Gi | ↓ cAMP | Presynaptic terminals, CNS, platelets | Inhibit NE release (autoreceptor), ↓ central sympathetic outflow, platelet aggregation |
| β1 | Gs | ↑ cAMP | Heart (SA, AV, myocardium) | ↑ HR, ↑ contractility, ↑ AV conduction |
| β2 | Gs | ↑ cAMP | Bronchi, skeletal muscle vessels, uterus, liver | Bronchodilation, vasodilation, glycogenolysis, tocolysis |
| β3 | Gs | ↑ cAMP | Adipose, bladder detrusor | Lipolysis, bladder relaxation |
| D1 | Gs | ↑ cAMP | Renal/mesenteric vessels | Vasodilation → ↑ urine output |
Memory aid: α1 = postsynaptic (effector organ), α2 = presynaptic (feedback brake)
3. Classification of Adrenergic Agonists
By mechanism:
- Direct-acting: Bind receptors directly - epinephrine, NE, isoproterenol, salbutamol, dobutamine, phenylephrine, clonidine
- Indirect-acting: Release stored NE - amphetamine, tyramine
- Mixed-acting: Both direct + indirect - ephedrine, dopamine (partially)
By receptor selectivity (Katzung Table 9-2):
| Drug | Receptor Profile |
|---|---|
| Phenylephrine | α1 > α2 >>>>> β |
| Clonidine | α2 > α1 >>>>> β |
| Norepinephrine | α1 = α2; β1 >> β2 |
| Epinephrine | α1 = α2; β1 = β2 |
| Isoproterenol | β1 = β2 >>>>> α |
| Dobutamine | β1 >> β2 > α |
| Salbutamol, terbutaline | β2 >> β1 >>>>> α |
| Dopamine | D1, D2; β then α (dose-dependent) |
4. Individual Drugs
Epinephrine (Adrenaline)
- Receptors: All (α1, α2, β1, β2) - prototype non-selective agonist
- CVS (dose-dependent):
- Low dose: β dominates → ↑ HR, ↑ contractility, ↑ systolic BP but ↓ diastolic BP (β2 skeletal muscle vasodilation), widened pulse pressure
- High dose: α dominates → both systolic + diastolic BP rise; reflex bradycardia possible
- Respiratory: β2 → bronchodilation; also stabilizes mast cells
- Metabolic: β2 → glycogenolysis, lipolysis, ↑ blood glucose; drives K⁺ into cells (hypokalemia)
- Uses: Anaphylaxis (IM, first-line), cardiac arrest (IV), local anesthetic adjuvant, open-angle glaucoma
Norepinephrine (Noradrenaline)
- Receptors: α1 = α2; β1 >> β2 (no clinically significant β2)
- CVS: Both systolic + diastolic BP rise → reflex bradycardia despite direct β1 stimulation (baroreceptor reflex overrides)
- Uses: Vasopressor of choice in septic shock and neurogenic shock
- Adverse: Tissue necrosis on extravasation - treat with phentolamine infiltration
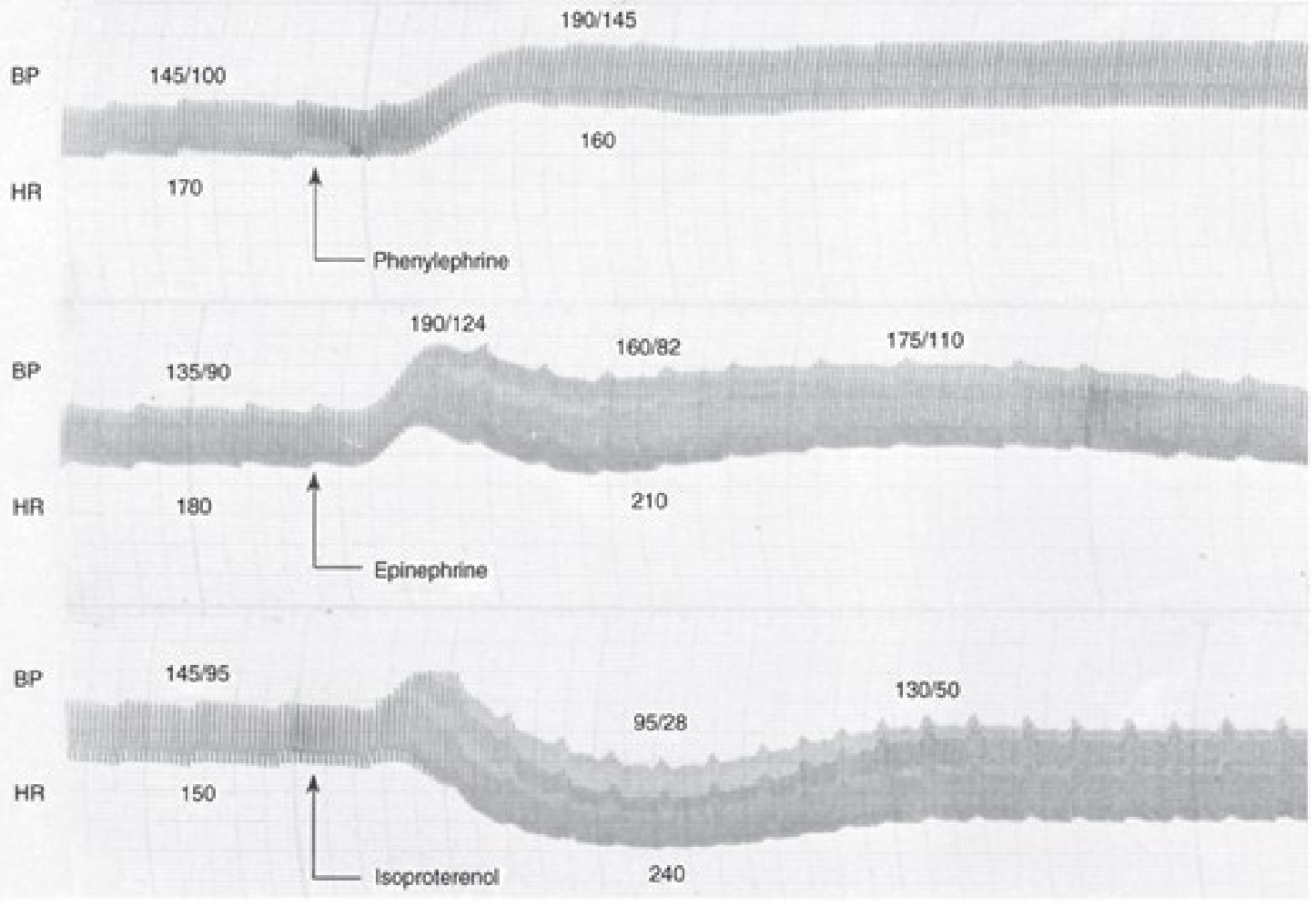
Isoproterenol (Isoprenaline)
- Receptors: β1 = β2, no α
- CVS: ↑ HR, ↑ contractility; systolic BP ↑, diastolic BP ↓ (β2 vasodilation), mean BP falls
- Uses: Complete heart block (bridge to pacemaker), pharmacologic cardiac stress testing
- The CVS tracing below shows the classic differences between all three catecholamines:
Dopamine
Dose-dependent receptor activation:
| Dose | Receptors | Main effect |
|---|---|---|
| 1-3 mcg/kg/min | D1 | Renal/mesenteric vasodilation |
| 3-10 mcg/kg/min | β1 | ↑ Contractility, ↑ HR |
| >10 mcg/kg/min | α1 | Vasoconstriction, ↑ BP |
- Uses: Cardiogenic shock, HF with hypotension
- "Renal-dose dopamine" for renoprotection is NOT evidence-based
Dobutamine
- Receptors: Predominantly β1; racemic mixture - net selective inotrope
- vs dopamine: More inotropic without as much tachycardia; no renal vasodilation
- Uses: Acute decompensated heart failure, dobutamine stress echo
Phenylephrine
- Receptors: Selective α1
- CVS: Vasoconstriction → ↑ BP; reflex bradycardia. No direct cardiac stimulation.
- Uses: Nasal decongestant, vasopressor in spinal anesthesia hypotension, mydriasis (ophthalmology), terminating PSVT (raises BP → reflex vagal → breaks circuit)
Clonidine
- Receptors: Central α2 agonist (locus coeruleus, NTS) → ↓ sympathetic outflow
- Uses: Hypertension, opioid/alcohol withdrawal, ADHD (2nd line), preoperative sedation, diarrhea in diabetic neuropathy
- Adverse: Sedation, dry mouth; rebound hypertension on abrupt withdrawal (important!)
Salbutamol (Albuterol) and β2-selective agonists
- Mechanism in asthma: β2 → ↑ cAMP → airway smooth muscle relaxation + mast cell stabilization
- Adverse: Tremor (β2, skeletal muscle), tachycardia (β1 spillover), hypokalemia
- Hypokalemia use: Can treat acute hyperkalemia (drives K⁺ into cells)
| Drug | Duration | Use |
|---|---|---|
| Salbutamol, terbutaline | SABA (4-6h) | Acute asthma reliever; tocolysis (terbutaline) |
| Salmeterol, formoterol | LABA (12h) | Asthma/COPD maintenance |
| Indacaterol | ULABA (24h) | Once-daily COPD |
Amphetamine
- Mechanism: Indirect; enters nerve terminal via Uptake-1 → reverses VMAT + NET → massive NE/dopamine efflux
- CNS: ↑ dopamine in nucleus accumbens → euphoria, addiction
- Uses: ADHD, narcolepsy
- Tachyphylaxis: Repeated dosing depletes NE stores → reduced effect
Ephedrine
- Mechanism: Mixed direct + indirect; non-catecholamine → not metabolized by COMT, orally active, enters CNS
- Uses: Spinal anesthesia hypotension, nasal decongestant
- Tachyphylaxis (like amphetamine)
5. Adrenergic Antagonists
Alpha-Blockers
| Drug | Selectivity | Key Feature | Uses |
|---|---|---|---|
| Phentolamine | α1 + α2, competitive | Short-acting, reversible | Pheochromocytoma crisis, NE extravasation antidote |
| Phenoxybenzamine | α1 + α2, irreversible | Alkylating agent, long-acting | Pre-op prep for pheochromocytoma |
| Prazosin | α1 selective | First-dose hypotension | Hypertension, BPH |
| Tamsulosin, silodosin | α1A selective (prostate) | Minimal BP effect | BPH (drug of choice) |
| Doxazosin, terazosin | α1 selective, long-acting | Once-daily | Hypertension + BPH |
"Epinephrine reversal" - After α-blockade, Epi's α-pressor effect is blocked but β2 vasodilation is unmasked → net BP falls. NE has no β2 → its pressor effect is only reduced (not reversed) after α-blockade.
Beta-Blockers
Generations:
- Non-selective (β1 + β2): Propranolol, timolol, nadolol, sotalol, pindolol (has ISA)
- Cardioselective (β1 > β2): Metoprolol, atenolol, bisoprolol, esmolol (IV, ultrashort-acting), acebutolol (has ISA)
- With vasodilating property: Carvedilol (+ α1 block), labetalol (+ α1 block), nebivolol (β3/NO vasodilation)
Lipophilic vs hydrophilic:
- Lipophilic (propranolol, metoprolol): hepatic metabolism, CNS penetration → nightmares, depression
- Hydrophilic (atenolol, nadolol): renal excretion, less CNS effects
ISA (Intrinsic Sympathomimetic Activity): Pindolol, acebutolol - partial agonists; less resting bradycardia; NOT preferred post-MI.
Uses of beta-blockers:
- Hypertension (reduce renin, reduce CO)
- Angina, post-MI (reduce oxygen demand, proven mortality benefit)
- Arrhythmias (AF rate control, PSVT prophylaxis)
- Stable heart failure (carvedilol, metoprolol succinate, bisoprolol - reduce mortality; NOT acute decompensation)
- Hyperthyroidism (propranolol - controls symptoms + blocks T4→T3 conversion)
- Glaucoma (timolol eye drops - ↓ aqueous humor production)
- Migraine prophylaxis (propranolol)
- Esophageal varices / portal hypertension (propranolol, nadolol)
- Anxiety/essential tremor (propranolol)
Critical contraindications:
- Asthma/COPD (β2 blockade → bronchospasm)
- Acute decompensated heart failure
- Heart block (2nd/3rd degree), severe bradycardia
- Prinzmetal angina (non-selective → unopposed α → coronary spasm)
- Pheochromocytoma without prior alpha-blockade
6. High-Yield Points for Exams
- Rate-limiting step = Tyrosine hydroxylase. Inhibited by metyrosine (used pre-op in pheochromocytoma).
- Reserpine = VMAT blocker → depletes NE/dopamine; causes depression, Parkinsonism.
- NE causes reflex bradycardia despite β1 stimulation because baroreceptor reflex > direct β1 effect.
- Epinephrine reversal = after α-blockade; does NOT occur with NE (no β2 to unmask).
- Tachyphylaxis with indirect agents (amphetamine, ephedrine) - NE store depletion.
- Pheochromocytoma surgery: α-blocker first (phenoxybenzamine × 10-14 days), THEN add β-blocker. Never β first.
- Dobutamine > dopamine for pure inotropy in cardiogenic shock.
- Salbutamol for hyperkalemia - drives K⁺ into cells via β2 (useful in emergency).
- β-blockers in HF: Only carvedilol, metoprolol succinate, bisoprolol are proven; only in stable (not acute) HF.
- Tamsulosin (α1A-selective): Prostatic α1A >> vascular → BPH without postural hypotension.
- Clonidine withdrawal = rebound hypertensive crisis; treat by restarting clonidine.
- Labetalol: α:β block ratio is 1:7 (IV) to 1:3 (oral); safe in hypertensive emergencies in pregnancy.
Sources: Katzung's Basic and Clinical Pharmacology 16e; Goodman & Gilman's Pharmacological Basis of Therapeutics - covering the same content as KDT Chapter on Adrenergic Drugs.
This is a shared conversation. Sign in to Orris to start your own chat.