Supraclavicular devices and their classi- and their classifications.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks and clear diagrams. Here is a full, well-structured answer:
Supraclavicular Devices and Their Classifications
The term "supraclavicular devices" in clinical medicine refers primarily to needles, catheters, and ultrasound probes used to access structures in the supraclavicular fossa - most commonly for brachial plexus nerve blocks or central venous access. Below is a structured overview.
1. Context: What Are "Supraclavicular Devices"?
There are two major clinical contexts:
| Context | Purpose |
|---|---|
| Regional Anesthesia | Needle/catheter placed in supraclavicular fossa to block the brachial plexus ("supraclavicular block") |
| Vascular Access | Needle/catheter inserted supraclavicularly to cannulate the subclavian or internal jugular vein |
2. Supraclavicular Brachial Plexus Block - Classification of Approaches
The supraclavicular block targets the brachial plexus at the level of the trunks and divisions, where the plexus is most compact. This gives it the nickname "spinal of the arm" - rapid onset, dense, reliable anesthesia from elbow distally.
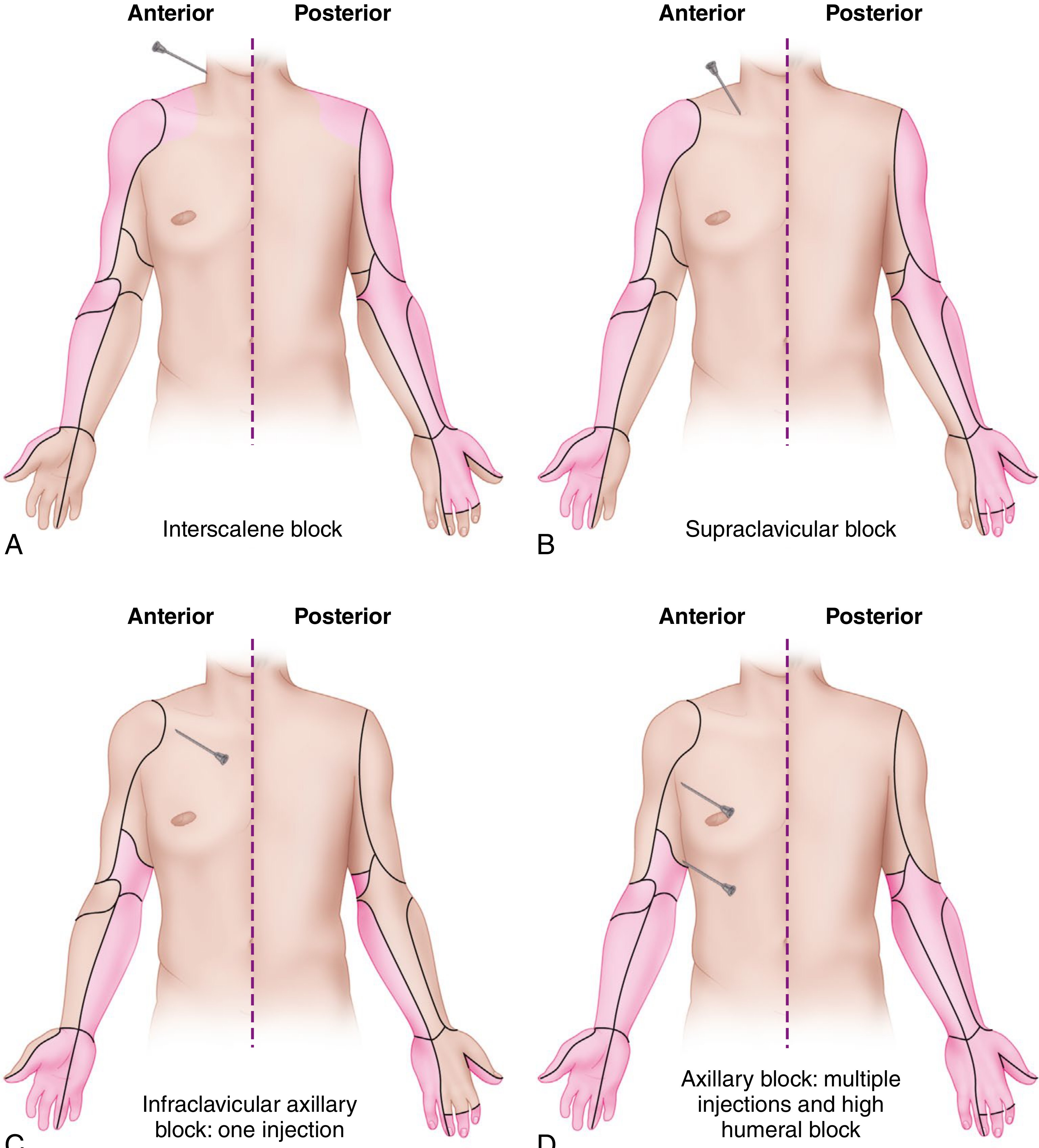
Figure: Distribution of brachial plexus blocks. B (top right) shows supraclavicular block - note the dense coverage from elbow to hand. - Campbell's Operative Orthopaedics 15e
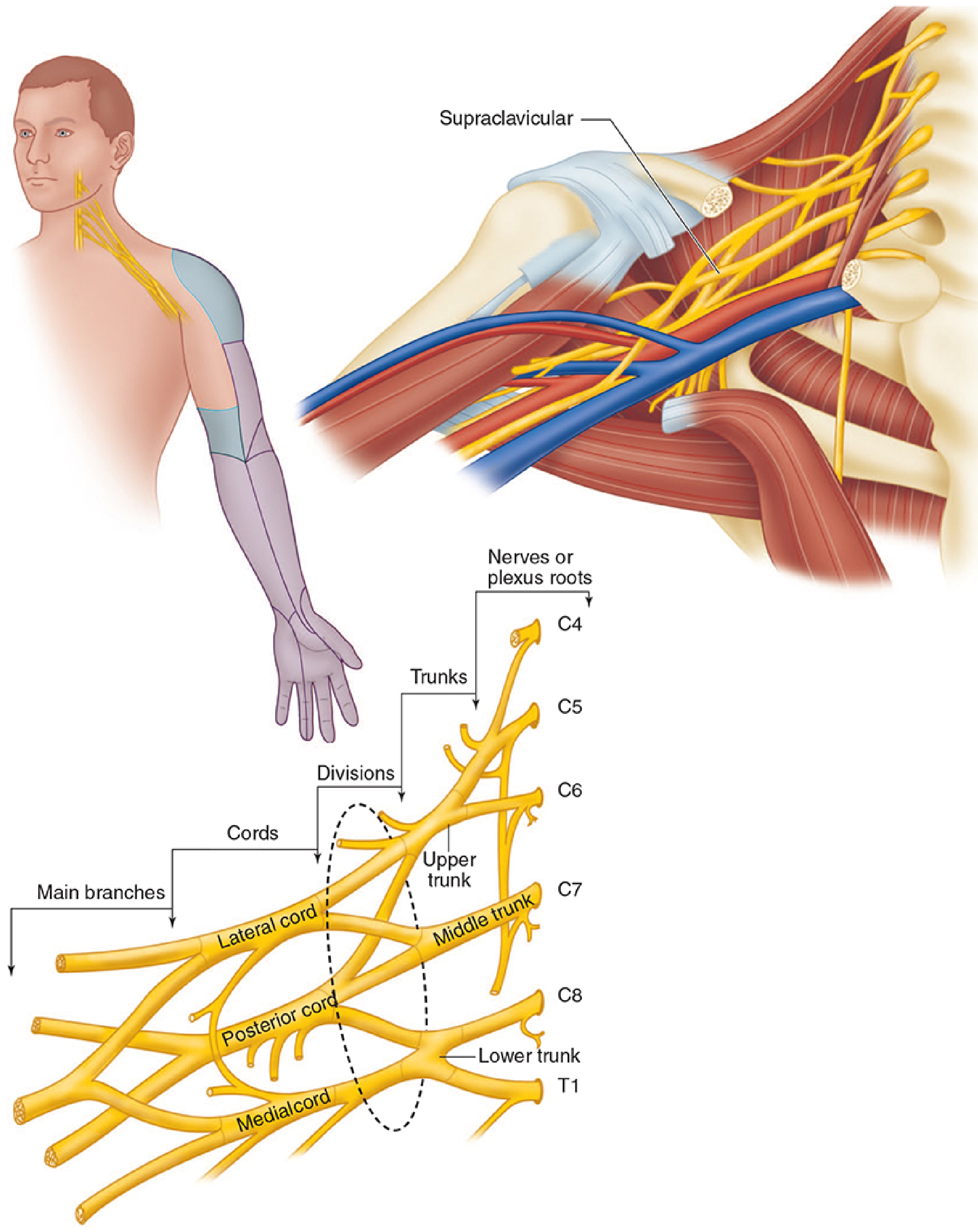
Figure: Brachial plexus anatomy showing the supraclavicular probe position at trunk/division level - Morgan & Mikhail's Clinical Anesthesiology 7e
Classification by Guidance Technique
Three main guidance modalities are used:
A. Paresthesia Technique (Historical)
- Pure landmark-based
- Needle advancement until patient reports paresthesia (tingling/shooting sensation in the arm)
- Largely abandoned due to risk of pneumothorax (0.5-6%) and nerve injury
- Not considered standard of care today
B. Peripheral Nerve Stimulator (PNS) Technique
- Needle attached to nerve stimulator
- Needle advanced until appropriate motor twitch is elicited at low current (0.4 mA, 0.1-0.3 ms)
- Acceptable twitches: pectoralis/deltoid/biceps (upper trunk), triceps (upper/middle trunk), hand/wrist flexion-extension (lower trunk)
- Distal hand/wrist responses best confirm fascial plane placement
- Can be used as an adjunct alongside ultrasound
C. Ultrasound-Guided Technique (Current Standard)
-
High-frequency linear transducer placed in the supraclavicular fossa, coronal oblique plane, just above and parallel to the clavicle
-
The brachial plexus appears as a "cluster of grapes" - multiple hypoechoic nodules lateral, posterior, and superior to the subclavian artery
-
First rib identified as a hyperechoic curvilinear line just deep to the artery (acts as a medial barrier)
-
Needle advanced in-plane, lateral to medial, toward the angle formed by the first rib and subclavian artery
-
Color Doppler used to identify surrounding vessels (suprascapular artery, dorsal scapular artery)
-
Significantly reduces (but does not eliminate) pneumothorax risk
-
Miller's Anesthesia 10e, Morgan & Mikhail's Clinical Anesthesiology 7e, Barash's Clinical Anesthesia 9e
Classification by Needle/Catheter Type
| Device | Use |
|---|---|
| Single-shot needle (22G, 2.5-5 cm) | One-time injection; short procedures |
| Perineural catheter | Continuous infusion for prolonged analgesia; note - supraclavicular catheters provide inferior analgesia vs. infraclavicular catheters and are more prone to displacement |
Classification Within the Brachial Plexus Block Family
The supraclavicular block is one of four major approaches to the brachial plexus:
| Approach | Plexus Level Targeted | Best For |
|---|---|---|
| Interscalene | Roots/trunks (C5-C7 predominant) | Shoulder surgery |
| Supraclavicular | Trunks/divisions | Elbow, forearm, wrist, hand (distal to shoulder) |
| Infraclavicular | Cords | Elbow, forearm, wrist, hand; stable catheter site |
| Axillary | Terminal branches | Forearm, wrist, hand |
- Campbell's Operative Orthopaedics 15e, Miller's Anesthesia 10e
3. Supraclavicular Central Venous Access Device
In emergency medicine, "supraclavicular approach" also refers to subclavian/internal jugular vein cannulation via a supraclavicular route:
-
Known as the "pocket shot"
-
Landmark: 1 cm lateral to the clavicular head of the SCM, 1 cm posterior to the clavicle; needle angle 10 degrees above horizontal, bevel oriented medially toward the contralateral nipple
-
Depth: typically 2-3 cm
-
Advantages over infraclavicular subclavian: fewer catheter malpositions, fewer failures, feasible in upright patients with severe orthopnea, less interference with CPR
-
Ultrasound guidance: probe placed to visualize the IJ/subclavian vein junction; the combined lumen appears as a "venous lake"
-
Tintinalli's Emergency Medicine, Comprehensive Study
4. Key Complications (Supraclavicular Block)
| Complication | Incidence |
|---|---|
| Pneumothorax | 0.5-6% (reduced but not eliminated by US guidance) |
| Phrenic nerve palsy | 40-60% |
| Horner syndrome | Present (cervical sympathetic block) |
| Recurrent laryngeal nerve palsy | Possible |
| Subclavian artery puncture | Possible |
| Ulnar nerve sparing | Lower trunk may be missed if not carefully traced caudally |
Contraindication: Patients unable to tolerate any respiratory compromise (bilateral blocks, contralateral phrenic palsy, severe COPD).
Summary
"Supraclavicular devices" classify primarily into:
- Guidance modality - paresthesia (historical) / nerve stimulator / ultrasound (current standard)
- Device type - single-shot needle vs. perineural catheter
- Application - brachial plexus block (anesthesia) vs. central venous access (emergency/critical care)
The supraclavicular brachial plexus block sits between the interscalene and infraclavicular blocks in the anatomical classification of upper limb regional anesthesia, targeting the brachial plexus where it is most compact - at the trunk/division level just above the first rib.
This is a shared conversation. Sign in to Orris to start your own chat.