What is phlebotomy why it is called And information about polycythemia vera
Reading File
Finding Sources
Finding Sources
Searching PubMed
polycythemia vera treatment phlebotomy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information. Let me compile the full answer.
Phlebotomy - What It Is and Why It's Called That
Etymology (Why It's Called "Phlebotomy")
The word phlebotomy comes from two Greek roots:
- phlebo- (φλέβα, phleba) = vein
- -tomy (τομή, tome) = cutting / incision
So literally, phlebotomy means "cutting of a vein." This reflects its ancient origin - the procedure has been performed for thousands of years (bloodletting was once a primary medical treatment). Today, the term covers both therapeutic phlebotomy (removing blood to treat disease) and diagnostic phlebotomy (drawing blood for laboratory testing).
What Is Phlebotomy?
Phlebotomy is the procedure of puncturing or incising a vein to draw blood, either for:
- Diagnostic purposes - collecting blood samples for laboratory tests (CBC, chemistry panels, cultures, etc.)
- Therapeutic purposes - removing a measured volume of blood to treat conditions of blood overload (like polycythemia vera, hemochromatosis, or porphyria cutanea tarda)
Basic Technique
- A tourniquet is placed around the arm to occlude the vein and make it prominent
- A needle is inserted into the vein
- Blood is collected into vacuum tubes or a collection bag
- For therapeutic phlebotomy, typically 450-500 mL of blood is removed per session
- Smaller-gauge needles and excessive suction pressure should be avoided as they cause hemolysis
(Roberts and Hedges' Clinical Procedures in Emergency; Tietz Textbook of Laboratory Medicine, 7th Ed.)
Polycythemia Vera (PV)
Definition
Polycythemia vera is a clonal myeloproliferative neoplasm characterized by an absolute increase in red cell mass, along with excess production of white blood cells and platelets (panmyelosis). It is classified as a primary marrow disorder - distinct from secondary polycythemia (which arises from hypoxia or elevated erythropoietin).
(Henry's Clinical Diagnosis and Management by Laboratory Methods)
Molecular Pathogenesis - The JAK2 Mutation
The central driver of PV is an activating mutation in JAK2 (Janus kinase 2), a tyrosine kinase that normally acts downstream of the erythropoietin receptor and other cytokine receptors.
- JAK2 V617F (exon 14 mutation) is found in ≥96% of PV patients
- A smaller subset carry JAK2 exon 12 mutations
- These mutations sharply lower the dependence of hematopoietic cells on growth factors, causing uncontrolled proliferation of erythroid, myeloid, and megakaryocytic lines
- The allele frequency is often high (>50%) in PV due to uniparental disomy at chromosome 9p
The diagram below shows the JAK2 protein structure and where these mutations occur:
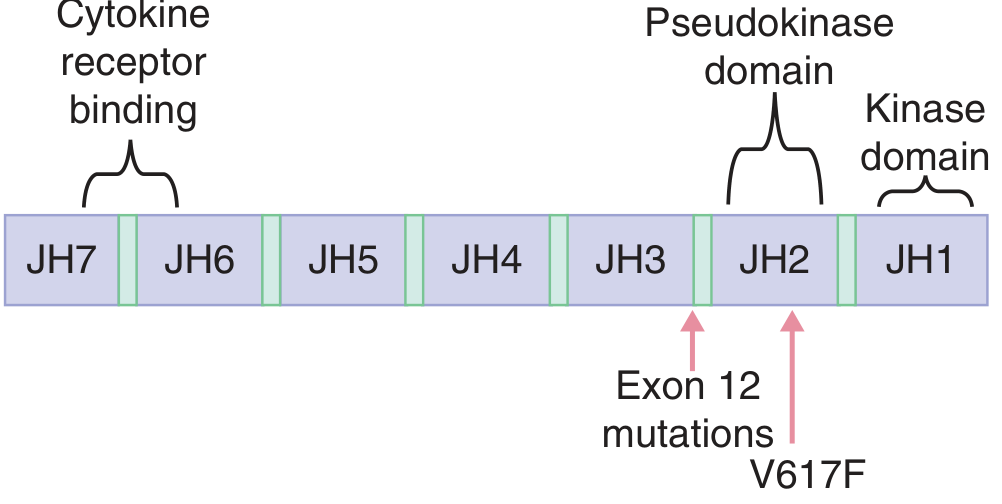
(Goldman-Cecil Medicine, 26th Ed.)
Pathophysiology
- The neoplastic clone proliferates independently of erythropoietin, so serum EPO levels are low (a key distinguishing feature from secondary polycythemia)
- RBC mass increases, raising blood viscosity - which can rise from the normal 3x water to 10x that of water
- Total blood volume increases, sometimes nearly doubling
- The vascular system becomes intensely engorged; capillaries become plugged
(Guyton and Hall Textbook of Medical Physiology)
Morphology (What You See Pathologically)
| Finding | Detail |
|---|---|
| Bone marrow | Hypercellular - increased erythroid, myeloid, megakaryocytic forms |
| Liver | Enlarged with foci of extramedullary hematopoiesis |
| Spleen | Mildly enlarged (~250-300 g) due to vascular congestion |
| Blood vessels | Thromboses and infarctions in heart, spleen, kidneys |
| Marrow fibrosis | Present in 10% at diagnosis; can progress to "spent phase" |
(Robbins & Kumar Basic Pathology)
Clinical Features
PV appears insidiously, typically in late middle age (median age ~61 years).
Symptoms from increased blood viscosity and mass:
- Headache, dizziness
- Plethoric (ruddy) face, often with slight cyanosis
- Hypertension
- Gastrointestinal symptoms
Thrombotic and hemorrhagic complications:
- ~30% develop thrombotic events (usually brain or heart)
- Hepatic vein thrombosis (Budd-Chiari syndrome) - uncommon but severe
- Minor hemorrhages (epistaxis, gum bleeding) are common
- Life-threatening hemorrhage in 5-10%
Other features:
- Aquagenic pruritus - itching triggered by water (from histamine released by neoplastic basophils) - affects ~36% of patients
- Peptic ulcers (also histamine-mediated)
- Gout in 5-10% (from high cell turnover)
- Splenomegaly (palpable spleen in ~36%)
- Erythromelalgia of the hands
Laboratory Findings
| Parameter | Value in PV |
|---|---|
| RBC count | 6-10 million/µL (normal ~4.5-5.5 million) |
| Hematocrit | ≥60% (normal 40-45%) |
| Hemoglobin (median) | ~18.4 g/dL |
| Granulocytes | Up to 50,000/µL |
| Platelets | Often >400,000/µL (thrombocytosis in 53%) |
| Serum EPO | Low (key differentiator from secondary polycythemia) |
| JAK2 V617F | Positive in ≥96% |
| Basophilia | Common |
Natural History and Complications
- Without treatment - death from vascular complications within months
- With phlebotomy - median survival increased to ~10 years
- "Spent phase" (post-PV myelofibrosis) - occurs in 15-20% after ~10 years; marrow is replaced by fibroblasts and collagen; spleen enlarges markedly as hematopoiesis shifts there
- Blast crisis / AML transformation - less common than in CML but does occur
(Robbins & Kumar Basic Pathology)
Treatment
1. Therapeutic Phlebotomy (First-Line)
- Cornerstone of treatment - removing 450-500 mL of blood per session
- Reduces RBC mass and lowers blood viscosity
- Initially scheduled weekly; hemoglobin checked at each session
- If hemoglobin drops below 10 g/dL, frequency is reduced to every other week
- Dramatically extends survival (from months to ~10 years)
2. Cytoreductive Therapy
- Hydroxyurea (hydroxycarbamide) - most commonly used, reduces all cell lines
- Ruxolitinib (JAK2 inhibitor) - approved for the spent phase of PV and for patients resistant/intolerant to hydroxyurea
- Interferon-alpha - used especially in younger patients or in pregnancy
- Anagrelide - to reduce platelet counts
3. Supportive Management
- Low-dose aspirin - reduces thrombotic risk
- Antihistamines or PUVA for pruritus
- Allopurinol for gout
- Treatment of erythromelalgia with aspirin
(Goldman-Cecil Medicine; Robbins & Kumar Basic Pathology)
Summary Table: PV vs. Secondary Polycythemia
| Feature | Polycythemia Vera | Secondary Polycythemia |
|---|---|---|
| Cause | JAK2 mutation (clonal) | Hypoxia / elevated EPO |
| Serum EPO | Low | High |
| WBC/Platelets | Increased (panmyelosis) | Normal |
| Splenomegaly | Present | Usually absent |
| Thrombosis risk | High | Moderate |
| Treatment | Phlebotomy, hydroxyurea | Treat underlying cause |
In short, phlebotomy is both a diagnostic tool (blood drawing) and the primary treatment for PV - the irony being that the very procedure named after cutting veins is what keeps PV patients alive longest.
This is a shared conversation. Sign in to Orris to start your own chat.