Extrapyramidal tracts
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile a complete, well-structured answer.
Extrapyramidal Tracts
Definition and the Pyramidal vs. Extrapyramidal Distinction
Descending motor pathways are divided into two broad groups:
- Pyramidal tracts (corticospinal and corticobulbar): originate in cortex, pass through the medullary pyramids, and descend directly onto lower motor neurons in the spinal cord.
- Extrapyramidal tracts: all other descending pathways - those that originate in the brain stem (not in the cortex directly) and do not pass through the medullary pyramids.
Classically, lesions of the pyramidal system cause spasticity and paralysis, while lesions of the extrapyramidal system cause involuntary movements, changes in muscle tone, and slowness of movement (bradykinesia) - without frank weakness. However, this strict division is now recognized as an oversimplification, because the two systems are interconnected and both contribute to voluntary and postural motor control. - Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 249
The Five Extrapyramidal Tracts
The extrapyramidal tracts are organized into two functional groups based on their spinal cord location and function:
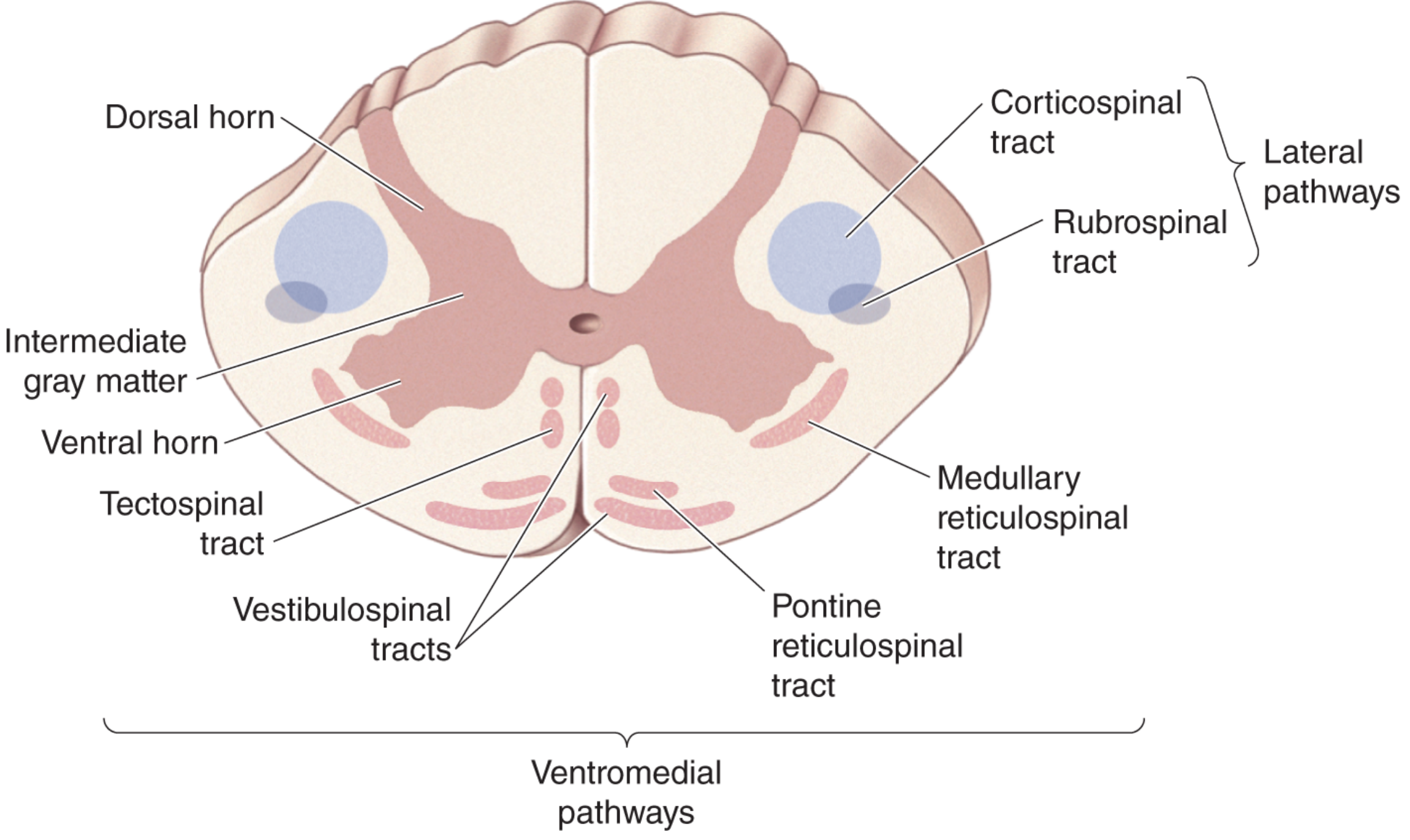
Group 1: Lateral Pathway
1. Rubrospinal Tract
| Feature | Detail |
|---|---|
| Origin | Red nucleus (midbrain tegmentum) |
| Decussation | Crosses immediately (ventral tegmental decussation) |
| Spinal cord position | Lateral column (lateral white matter, just anterior to lateral corticospinal tract) |
| Termination | Motoneurons in the lateral spinal cord / dorsolateral horn |
| Function | Controls distal limb muscles for fine voluntary movements; activates flexors, inhibits extensors |
| Input to red nucleus | Cerebral cortex (motor cortex via corticorubral fibers) + cerebellar deep nuclei (dentate nucleus) |
The rubrospinal tract is the only extrapyramidal tract in the lateral pathway, making it functionally complementary to the lateral corticospinal tract. In humans, its role is relatively minor compared to primates, as the lateral corticospinal tract dominates. - Neuroscience: Exploring the Brain, 5th ed.
Group 2: Ventromedial Pathways
These four tracts control axial (trunk) and proximal limb muscles, maintain posture, and regulate balance.

2. Lateral Vestibulospinal Tract
| Feature | Detail |
|---|---|
| Origin | Lateral vestibular nucleus (Deiters' nucleus) |
| Course | Ipsilateral, projects all the way to lumbar spinal cord |
| Termination | Ventromedial spinal cord, extensor motor neurons |
| Function | Activates extensors, inhibits flexors - maintains upright posture and balance by facilitating antigravity (extensor) muscles of the legs |
A second vestibulospinal component projects bilaterally to the cervical cord, controlling neck/back muscles to stabilize head position (keeping eyes stable during body movement). - Neuroscience: Exploring the Brain, 5th ed., p. 1329
3. Pontine (Medial) Reticulospinal Tract
| Feature | Detail |
|---|---|
| Origin | Pontine reticular formation (medial / oral pontine nucleus) |
| Course | Bilateral; ventromedial spinal cord |
| Function | Excitatory - enhances antigravity stretch reflexes; facilitates extensor muscles; helps maintain standing posture by resisting gravity. Predominant effect on extensors |
4. Medullary (Lateral) Reticulospinal Tract
| Feature | Detail |
|---|---|
| Origin | Medullary reticular formation |
| Course | Bilateral; ventromedial spinal cord |
| Function | Inhibitory - opposes the pontine tract; inhibits extensor stretch reflexes and has a generalized inhibitory effect on both flexor and extensor muscles, with predominant inhibition of extensors |
The pontine and medullary reticulospinal tracts thus work antagonistically. The pontine tract facilitates extensors (anti-gravity); the medullary tract inhibits extensors. Together they fine-tune postural tone. - Costanzo Physiology, 7th ed.
5. Tectospinal Tract
| Feature | Detail |
|---|---|
| Origin | Superior colliculus (tectum of the midbrain) |
| Decussation | Crosses immediately (dorsal tegmental decussation) |
| Projection | Only to cervical spinal cord |
| Function | Controls neck muscles - mediates orienting movements of the head and eyes in response to visual, auditory, and somatosensory stimuli; integrates head-eye coordination |
The superior colliculus receives input from the retina plus visual, auditory, and somatosensory cortex, constructing a spatial map. Activation drives head and eye orientation to bring a stimulus to the fovea. - Neuroscience: Exploring the Brain, 5th ed., p. 1329
Summary Table: All Five Extrapyramidal Tracts
| Tract | Origin | Crosses? | Spinal Position | Main Function |
|---|---|---|---|---|
| Rubrospinal | Red nucleus (midbrain) | Yes (immediately) | Lateral column | Distal limb movements, flexor activation |
| Lateral vestibulospinal | Lateral vestibular nucleus (Deiters') | No (ipsilateral) | Ventromedial | Extensor facilitation, balance/posture |
| Pontine reticulospinal | Pontine reticular formation | Bilateral | Ventromedial | Extensor facilitation (antigravity) |
| Medullary reticulospinal | Medullary reticular formation | Bilateral | Ventromedial | Extensor inhibition, tone modulation |
| Tectospinal | Superior colliculus | Yes (immediately) | Ventromedial (cervical only) | Head/neck orienting, visuo-motor reflexes |
The Extrapyramidal System - Broader Concept
The term "extrapyramidal system" is also used more broadly in clinical neurology to refer to the basal ganglia and their associated circuits, which modify motor function without being part of the corticospinal tract. These structures include:
- Basal ganglia: caudate nucleus, putamen, globus pallidus (internal and external), substantia nigra (pars compacta and pars reticulata), subthalamic nucleus
- Red nucleus and reticular formation of the brainstem
- Cerebellum (sometimes grouped)
The basal ganglia influence movement via a loop: Cortex → Striatum → Globus pallidus/SNr → Thalamus (VL, VA nuclei) → Cortex. The output of the basal ganglia (GPi and SNr) is tonically inhibitory (GABAergic) to the thalamus. Motor activity disinhibits thalamic relay nuclei, enabling smooth, coordinated movement. - Barash's Clinical Anesthesia, 9e; Kaplan & Sadock, p. 250
Clinical Relevance: Extrapyramidal Dysfunction
Damage to extrapyramidal structures produces characteristic clinical syndromes:
| Structure Damaged | Clinical Syndrome |
|---|---|
| Substantia nigra (dopaminergic neurons) | Parkinson disease - bradykinesia, rigidity, resting tremor, postural instability |
| Striatum/basal ganglia | Huntington disease - chorea, athetosis |
| Red nucleus | Contralateral intention tremor and choreoathetosis (Benedikt syndrome if CN III also involved) |
| Subthalamic nucleus | Hemiballismus (wild flinging movements of contralateral limbs) |
| Bilateral (kernicterus, hypoxia) | Double athetosis - choreoathetosis, dystonia from neonatal insult |
Extrapyramidal symptoms (EPS) from antipsychotic drugs (dopamine D2 blockade) include: acute dystonia, akathisia, parkinsonism, and tardive dyskinesia - all mimicking natural extrapyramidal system dysfunction. - Adams and Victor's Principles of Neurology, 12th ed.; Maudsley Prescribing Guidelines, 15th ed.
Sources: Costanzo Physiology 7th ed. | Neuroscience: Exploring the Brain 5th ed. | Adams and Victor's Principles of Neurology 12th ed. | Kaplan & Sadock's Comprehensive Textbook of Psychiatry | Barash's Clinical Anesthesia 9th ed. | Ganong's Review of Medical Physiology 26th ed.
This is a shared conversation. Sign in to Orris to start your own chat.