Grand case presentation coronary circulation nd structure of valve
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have all the information needed for a comprehensive grand case presentation. Let me compile the full response.
Grand Case Presentation: Coronary Circulation & Structure of Cardiac Valves
PART I: CORONARY CIRCULATION
1. Overview and Clinical Significance
About one-third of all deaths in industrialized countries result from coronary artery disease, making this one of the most important topics in cardiovascular medicine. Most older adults have at least some impairment of the coronary circulation.
- Guyton and Hall Textbook of Medical Physiology, p. 268
2. Anatomical Arrangement of the Coronary Blood Supply
The main coronary arteries lie on the surface of the heart (epicardium). Smaller arteries penetrate from the surface into the cardiac muscle mass. Only the inner ~0.1 mm of the endocardial surface can receive nutrition directly from the intracavitary blood; all remaining myocardium depends on coronary flow.
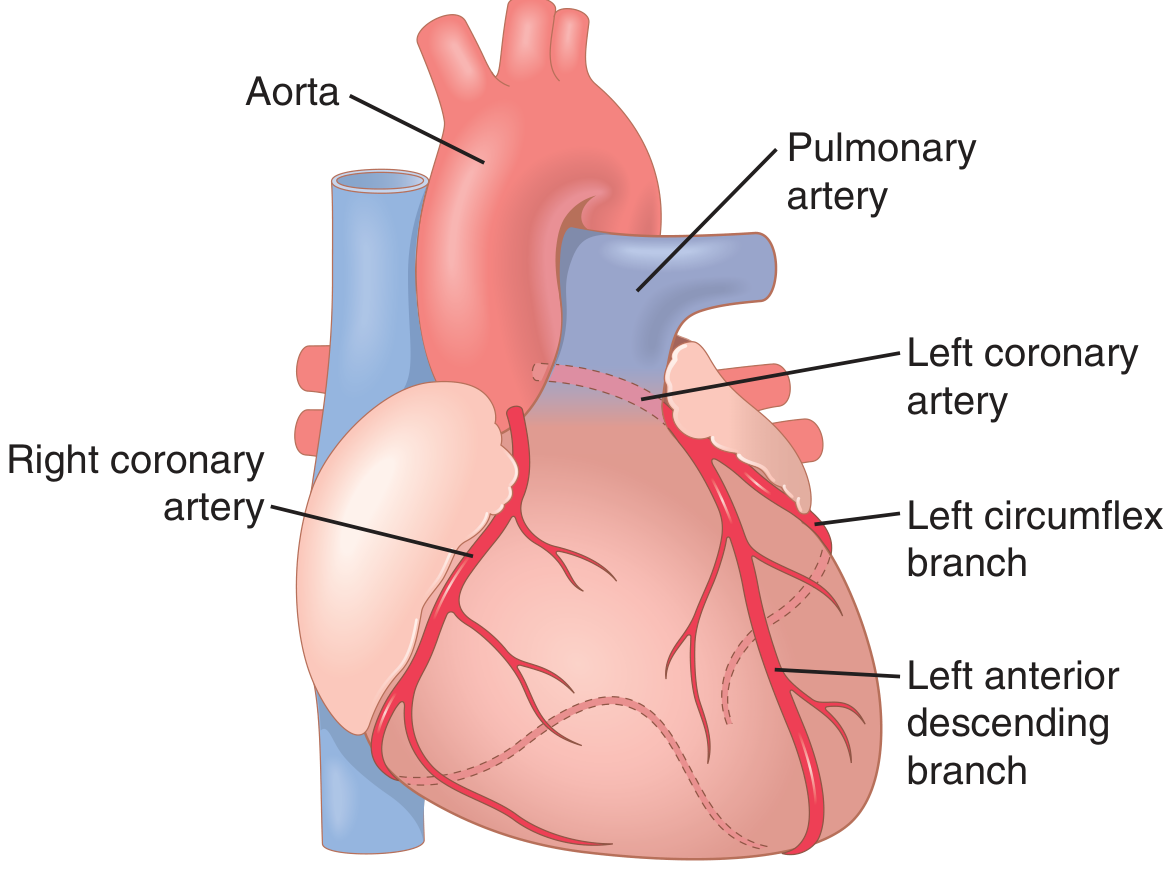
Left Coronary Artery (LCA)
- Supplies the anterior and left lateral portions of the left ventricle
- Divides into:
- Left Anterior Descending (LAD) - supplies anterior LV wall and anterior septum
- Left Circumflex (LCx) - supplies lateral and posterior LV
Right Coronary Artery (RCA)
- Supplies most of the right ventricle
- Supplies the posterior part of the left ventricle in 80-90% of people (right dominant circulation)
3. Coronary Venous Drainage
| Pathway | Origin | Destination |
|---|---|---|
| Coronary sinus | ~75% of LV venous blood | Right atrium |
| Anterior cardiac veins | RV venous blood | Right atrium directly |
| Thebesian veins | Small amounts | All four chambers directly |
4. Normal Coronary Blood Flow
- Resting coronary flow: ~70 mL/min/100 g of heart weight (~225 mL/min total)
- This represents 4-5% of total cardiac output
- During strenuous exercise, coronary flow increases 3-4 fold (cardiac work can increase 6-9 fold)
5. Phasic Flow: The Systole-Diastole Paradox
A unique feature of the coronary circulation is mechanical compression during systole:
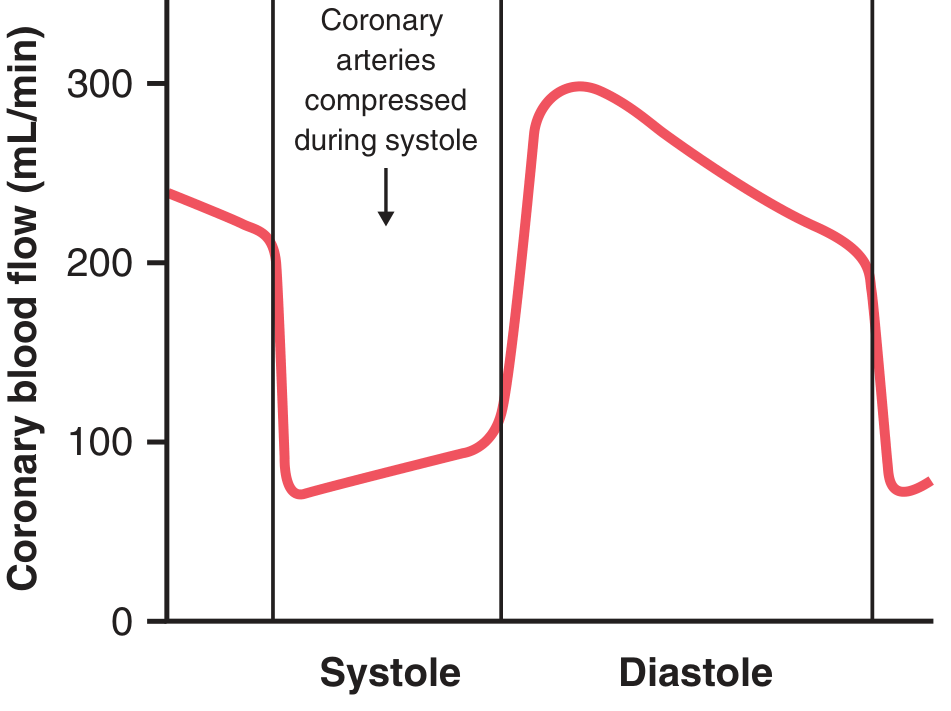
- During systole: Ventricular wall contraction compresses intramuscular coronary vessels - LV capillary flow falls dramatically (nearly to zero at peak systole)
- During diastole: Muscle relaxes, obstruction removed - blood flows rapidly. The left coronary is predominantly diastolic-dependent
- RV coronary flow is less affected because RV wall tension is lower
- After the systolic compression is relieved, reactive hyperemia occurs to repay the O2 debt
Key teaching point: The left coronary artery fills predominantly in diastole. This is why tachycardia (shorter diastole) and aortic regurgitation (reduced diastolic perfusion pressure) impair coronary flow.
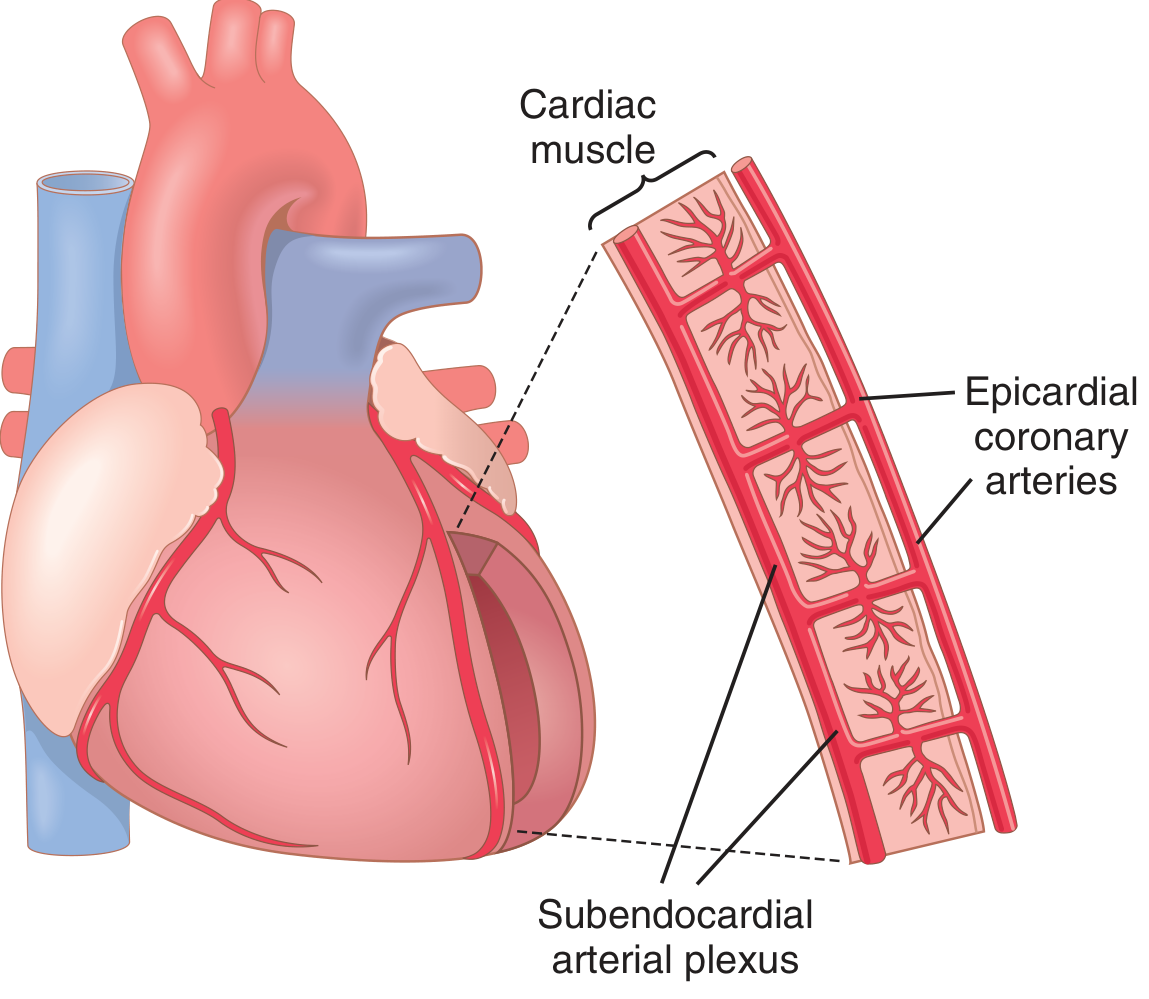
6. Epicardial vs Subendocardial Blood Flow
-
Epicardial arteries: Large surface vessels, act as conduits
-
Intramuscular arteries: Penetrate the myocardium; subject to compression during systole
-
Subendocardial arterial plexus: Lies immediately beneath the endocardium; most vulnerable during systole and in states of elevated end-diastolic pressure
-
The subendocardial plexus has extra vessels to compensate for systolic compression - but this reserve is exhausted in ischemia (subendocardium is first to infarct)
-
Guyton and Hall Textbook of Medical Physiology, p. 269
7. Control of Coronary Blood Flow
A. Local Metabolic Control (Primary Mechanism)
Coronary blood flow is regulated mostly by local arteriolar vasodilation in response to myocardial metabolic needs.
- ~70% of O2 in coronary arterial blood is extracted at rest (nearly maximal extraction)
- When O2 demand increases, there is essentially no reserve to extract more O2 - the only response is to increase blood flow
- The key vasodilator signal is hypoxia itself and adenosine
Mechanism of Adenosine Release:
- Increased metabolic rate → decreased O2 in cells
- ATP degrades → AMP → adenosine released into tissue fluid
- Adenosine causes arteriolar dilation → increased coronary flow → O2 delivery matches demand
- After vasodilation, adenosine is reabsorbed and used to regenerate ATP
Other vasodilators: Adenosine phosphate compounds, K⁺, H⁺, CO2, prostaglandins, nitric oxide
Costanzo Physiology (p. 996): "Blood flow through the coronary circulation is controlled almost entirely by local metabolites, with sympathetic innervation playing only a minor role. The most important local metabolic factors are hypoxia and adenosine."
B. Nervous Control (Secondary, Largely Overridden by Metabolic)
| Stimulus | Direct Vascular Effect | Indirect Effect (via metabolism) | Net Outcome |
|---|---|---|---|
| Sympathetic (NE, Epi) | Epicardial: α1 constriction; Intramuscular: β2 dilation | ↑ HR & contractility → ↑ O2 demand → vasodilation | Net: coronary dilation |
| Vagal (ACh) | Direct dilation of coronary arteries | ↓ HR → ↓ O2 demand → vasoconstriction | Net: coronary constriction |
- Epicardial vessels: Predominance of α1 (constricting) receptors
- Intramuscular arteries: More β2 (dilating) receptors
The indirect metabolic effects usually override the direct neural effects.
8. Cardiac Muscle Metabolism and Ischemia
- At rest, ~70% of cardiac energy comes from fatty acid oxidation (not glucose)
- Under ischemia/anaerobiasis: switches to anaerobic glycolysis - consumes glucose rapidly and produces lactic acid (source of ischemic cardiac pain)
- ATP degrades to ADP → AMP → adenosine during severe ischemia
- If severe ischemia persists >30 minutes, ~half the adenine base is lost from cells
- New adenine is synthesized at only 2%/hour - explaining why reperfusion after 30+ min may be too late to salvage cells
9. Ischemic Heart Disease - Overview
- Most common cause of death in Western countries
- ~35% of Americans aged 65+ die from ischemic heart disease
- Most common cause: atherosclerosis - cholesterol deposition under endothelium → fibrous invasion → plaque → lumen obstruction
PART II: STRUCTURE OF CARDIAC VALVES
The heart has four valves: two atrioventricular (AV) valves and two semilunar valves.
1. Atrioventricular Valves - General Structure
Each AV valve consists of:
-
Leaflets (cusps): Flaps of connective tissue covered on both sides by endocardium, devoid of blood vessels
- Atrial surface: smooth
- Ventricular surface: rough, with chordae tendineae attachments
-
Fibrous annulus: Ring of fibrous tissue to which the base of each cusp is secured; maintains shape of the orifice
-
Chordae tendineae: Fibrous tendinous cords; arise from free margins and inferior surface of leaflets, connecting to papillary muscles
-
Papillary muscles: Conical projections of myocardium; contract simultaneously with the ventricular walls
-
Color Atlas of Human Anatomy Vol. 2, p. 55
2. Tricuspid Valve (Right AV Valve)
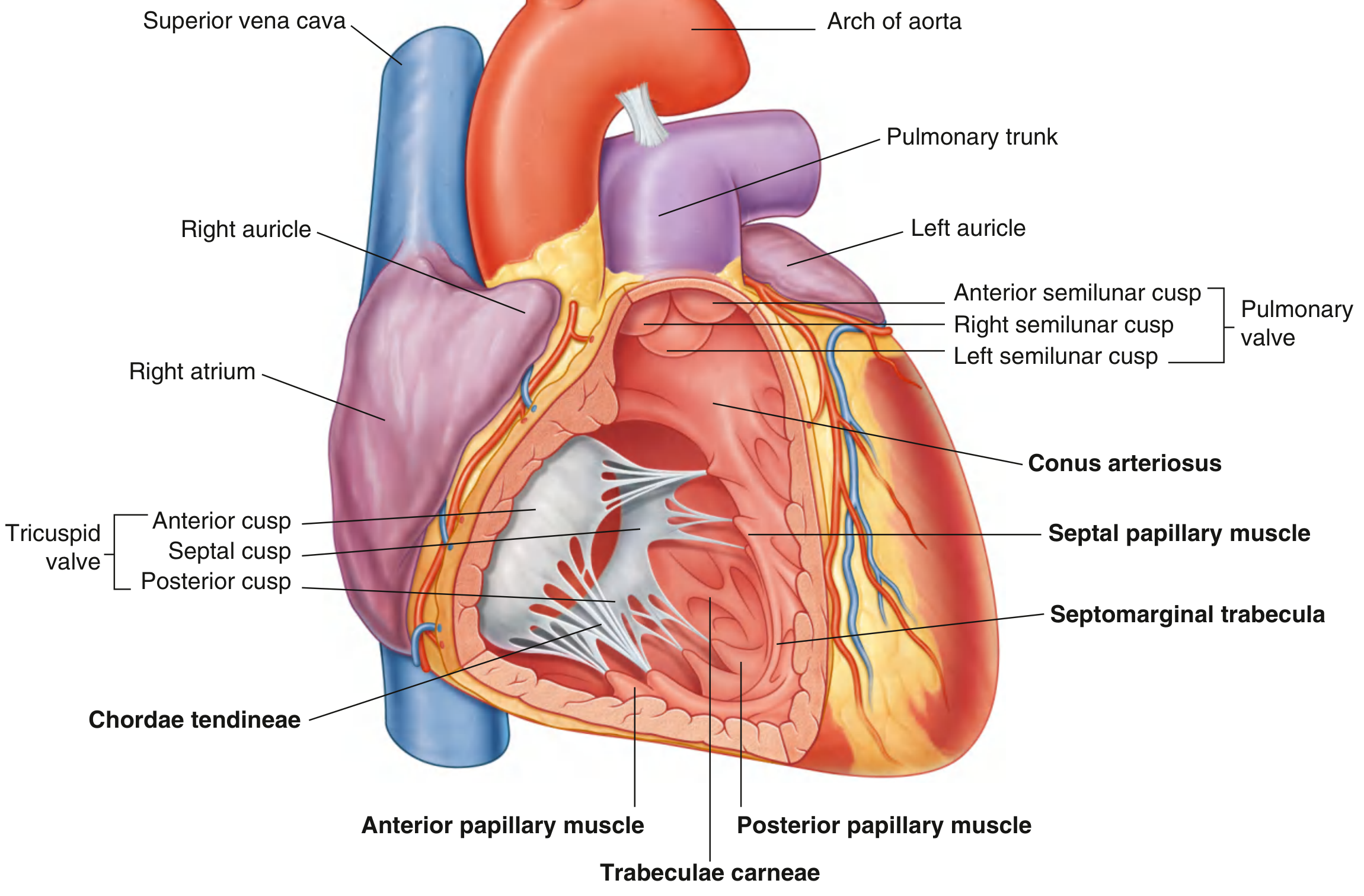
Three cusps (named by position in RV):
| Cusp | Position | Notes |
|---|---|---|
| Anterior | Anterior wall | Largest cusp; chordae attach to anterior papillary muscle |
| Septal | Interventricular septum | Attachment divides membranous septum |
| Posterior | Posterior wall | May have chordae from multiple sources |
Between the three main cusps are small commissural (intermediate) segments that do not reach the fibrous ring.
Three papillary muscles (RV):
- Anterior papillary muscle - largest and most constant; arises from anterior wall; has a direct connection via the septomarginal trabecula (moderator band) - which also carries the right bundle branch
- Posterior papillary muscle - may be one, two, or three structures
- Septal papillary muscle - most inconsistent; often small or absent; chordae may arise directly from septal wall
Functional mechanism:
- During diastole: valve opens, cusps project into RV, blood fills
- During systole: papillary muscles contract simultaneously with myocardium, tightening chordae tendineae
- This prevents cusp eversion into the right atrium (i.e., prevents regurgitation)
- Chordae from two papillary muscles attach to each cusp, preventing cusp separation
Clinical note: Papillary muscle necrosis after myocardial infarction → valve prolapse → acute mitral (or tricuspid) regurgitation
3. Mitral Valve / Bicuspid Valve (Left AV Valve)
Two cusps:
- Anterior (anteromedial) cusp - larger; continuous at its septal origin with the wall of the aorta (aortomitral continuity)
- Posterior (posterolateral) cusp
- Two small commissural cusps do not extend to the fibrous annulus
Subvalvular apparatus:
- Anterior papillary muscle - large, arises from anterolateral LV wall
- Posterior papillary muscle - arises from posterolateral LV wall
- Each papillary muscle supports adjacent sides of both leaflets
- Short and thick chordae tendineae compared to the RV
Mitral valve apparatus (complete functional unit):
- Leaflets
- Fibrous annulus
- Chordae tendineae (marginal/primary from free edges; secondary from undersurface)
- Papillary muscles
- Subjacent myocardium
- Guyton and Hall Textbook of Medical Physiology; Sabiston Textbook of Surgery, p. VALVE ANATOMY
4. Semilunar Valves - General Structure
Both the aortic and pulmonary valves consist of three nearly equally sized semilunar cusps formed by folds of endocardium. Their attachment is curved (semilunar in shape).
Key structural features of each cusp:
| Feature | Description |
|---|---|
| Nodule (of Arantius/nodule of semilunar cusp) | Thickened, fibrous mid-point of free margin; cusps meet here to ensure complete closure |
| Lunule | Thin, crescent-shaped rim on either side of the nodule along the free margin |
| Sinus (of Valsalva) | Pocket-like bulging of the vessel wall opposite each cusp |
5. Pulmonary Valve
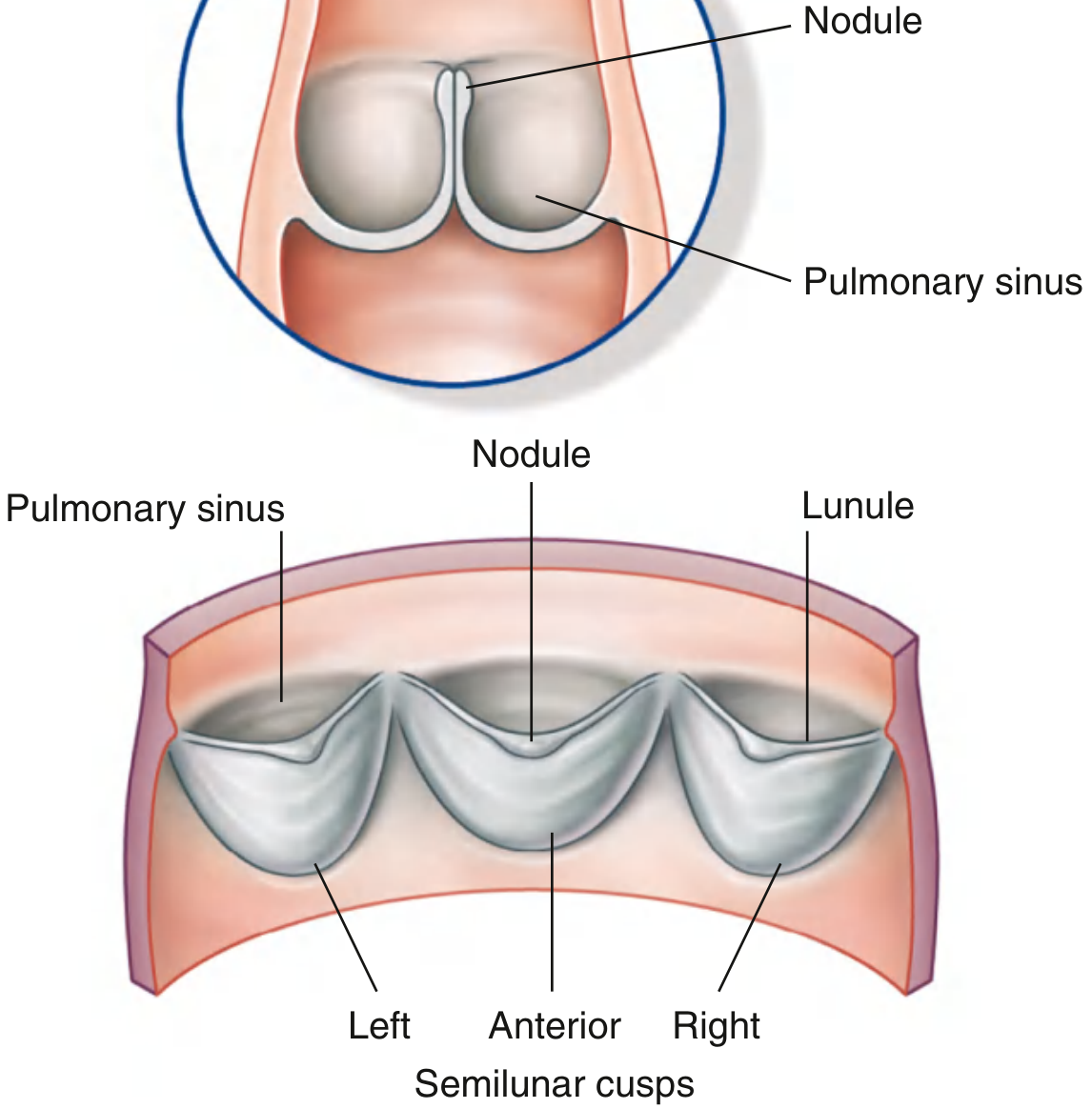
- Located between the infundibulum (conus arteriosus) and the pulmonary trunk
- Three cusps: Anterior, Right, and Left semilunar cusps
- After ventricular contraction ends, blood recoils back and fills the pulmonary sinuses - this forces the cusps to close, preventing backflow into the RV
6. Aortic Valve
- Located between the aortic vestibule and the aorta
- Three cusps: Right, Left, and Posterior (non-coronary) semilunar cusps
- The vessel wall near the cusps bulges outward forming the aortic sinuses (sinuses of Valsalva), which enlarges the luminal diameter (aortic bulb)
- The left coronary artery arises from the aortic sinus of the left semilunar cusp
- The right coronary artery arises from the aortic sinus of the right semilunar cusp
- The posterior sinus has no coronary ostium ("non-coronary sinus")
Key anatomical point: The coronary arteries originate from the sinuses of Valsalva - their position behind the open cusps during systole protects them from being occluded, and the sinus geometry creates eddy currents that initiate cusp closure.
7. Valve Mechanics - Summary Table
| Valve | Type | Cusps/Leaflets | Subvalvular Apparatus | Open During | Closed During |
|---|---|---|---|---|---|
| Tricuspid | AV | 3 (Ant, Sep, Post) | Chordae + papillary muscles | Diastole | Systole |
| Mitral | AV | 2 (Ant, Post) | Chordae + papillary muscles | Diastole | Systole |
| Pulmonary | Semilunar | 3 (Ant, R, L) | None | Systole | Diastole |
| Aortic | Semilunar | 3 (R, L, Post) | None | Systole | Diastole |
8. Functional Anatomy During the Cardiac Cycle
Filling phase (diastole):
- AV valves open - blood flows from atria into ventricles
- Semilunar valves closed - blood in aorta/PA does not reflux back
Ejection phase (systole):
- AV valves closed - papillary muscles contract, chordae taut, preventing leaflet eversion into atria
- Semilunar valves open - blood ejected into aorta and pulmonary trunk
- After ejection ends, recoil of blood fills sinuses of Valsalva, forces semilunar cusps closed
Key Clinical Correlations
| Condition | Mechanism | Valve/Vessel Involved |
|---|---|---|
| Angina / MI | Atherosclerotic plaque occludes coronary lumen | RCA or LAD most commonly |
| Acute MR after MI | Papillary muscle necrosis → leaflet prolapse | Mitral valve (posterior PM more vulnerable - single blood supply from RCA) |
| Aortic stenosis | Calcification/fusion of aortic valve cusps | Aortic valve (semilunar) |
| Rheumatic valve disease | Leaflet thickening, chordae shortening/fusion | Mitral most common, then aortic |
| Subendocardial infarction | Subendocardial plexus most vulnerable to ischemia (highest wall stress, compressed in systole) | Subendocardium of LV |
Sources cited:
- Guyton and Hall Textbook of Medical Physiology (pp. 268-270)
- Costanzo Physiology 7th Edition (p. 996-998)
- Gray's Anatomy for Students (pp. 233-236)
- Color Atlas of Human Anatomy Vol. 2, Internal Organs (pp. 54-55)
- Sabiston Textbook of Surgery, 21st Edition (Valve Anatomy section)
This is a shared conversation. Sign in to Orris to start your own chat.