Liver diseaseas
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Searching the Web
liver diseases clinical overview cirrhosis hepatitis NAFLD 2025 guidelines
Finding Sources
Finding Sources
Searching PubMed
liver disease cirrhosis management
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
I have enough comprehensive data to write a thorough clinical reference. Let me compile the full response now.
Liver Diseases - Clinical Reference
This reference covers the major liver diseases encountered in clinical practice, organized by category.
1. Overview & Classification
The liver diseases are broadly classified as:
| Category | Examples |
|---|---|
| Infectious | Viral hepatitis A, B, C, D, E |
| Steatotic | Alcoholic liver disease (ALD), MASLD/NAFLD/NASH |
| Autoimmune | Autoimmune hepatitis, Primary biliary cholangitis (PBC), Primary sclerosing cholangitis (PSC) |
| Drug/Toxin-induced | Acetaminophen toxicity, drug-induced liver injury (DILI) |
| Inherited/Metabolic | Hemochromatosis, Wilson disease, alpha-1 antitrypsin deficiency |
| Cholestatic | Biliary obstruction, cholestasis of sepsis |
| Vascular | Budd-Chiari syndrome, sinusoidal obstruction syndrome |
| Neoplastic | Hepatocellular carcinoma (HCC), cholangiocarcinoma |
| End-stage | Cirrhosis, acute liver failure |
The most common causes of chronic liver disease, in order of frequency: chronic hepatitis C, alcoholic liver disease, MASLD/NASH, chronic hepatitis B, autoimmune hepatitis, sclerosing cholangitis, primary biliary cholangitis, hemochromatosis. - Harrison's Principles of Internal Medicine, 22E (2025)
2. Clinical Features of Liver Disease
Symptoms
- Fatigue, anorexia, right upper quadrant discomfort
- Jaundice, dark urine, pale stools (cholestatic pattern)
- Pruritus (especially in cholestatic disease)
Physical Examination Signs
Early/moderate disease:
- Icterus (jaundice detectable when bilirubin >2.5 mg/dL)
- Hepatomegaly (firmness and nodularity suggest cirrhosis)
- Splenomegaly (suggests portal hypertension/cirrhosis)
- Spider angiomata (arms, face, upper torso - fill from center outward)
- Palmar erythema
Advanced disease:
- Muscle wasting, ascites, peripheral edema
- Dilated abdominal veins (caput medusae)
- Hepatic fetor, asterixis
- Mental confusion → stupor → coma (hepatic encephalopathy)
- Gynecomastia, testicular atrophy (hyperestrogenemia in alcoholic cirrhosis)
Harrison's Principles of Internal Medicine, 22E
3. Cirrhosis
Pathophysiology
Cirrhosis is the end-stage of any chronic liver disease, characterized by widespread fibrosis and regenerative nodule formation. Collagen deposition in the space of Disse leads to defenestration of sinusoidal endothelial cells ("capillarization"), altered hepatocyte-plasma exchange, and decreased sinusoidal diameter exacerbated by stellate cell contraction. - Goldman-Cecil Medicine
Complications
The two main consequences are portal hypertension and liver insufficiency:
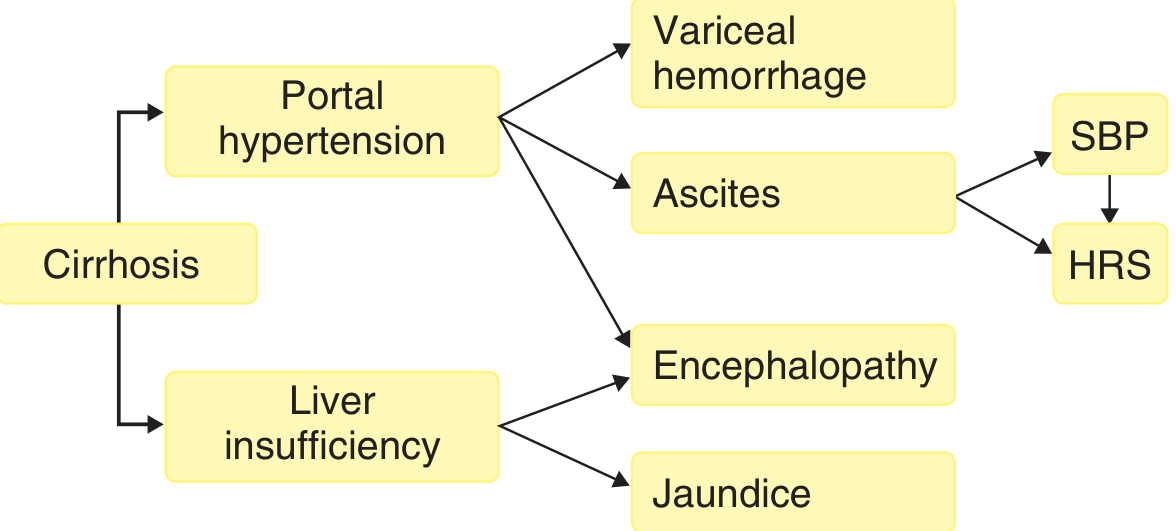
Portal Hypertension
- Results from increased sinusoidal vascular resistance (fixed: fibrosis + nodules; functional: vasoconstriction from intrahepatic NO deficiency) plus increased portal venous inflow from splanchnic vasodilation
- Threshold: hepatic venous pressure gradient (HVPG) >10-12 mmHg for variceal formation; >12 mmHg for ascites formation
Varices and Variceal Hemorrhage
- Gastroesophageal varices form via dilation of coronary and gastric veins
- Variceal rupture risk is proportional to variceal diameter x intravariceal pressure / wall thickness (LaPlace's law)
- Variceal hemorrhage is one of the most dangerous complications of portal hypertension
Ascites
- Secondary to sinusoidal hypertension and sodium retention driven by splanchnic vasodilation and increased NO production
- Progressive: leads to hyponatremia, refractory ascites, and hepatorenal syndrome (HRS)
Spontaneous Bacterial Peritonitis (SBP)
- Infection of ascitic fluid without a hollow viscus perforation
- Mechanism: bacterial translocation from intestinal lumen to mesenteric lymph nodes, facilitated by impaired Kupffer cell function (due to portosystemic shunting)
- Diagnosed by ascitic PMN count >250 cells/mm³
Hepatic Encephalopathy (HE)
- Results from both portal hypertension (portosystemic shunting) and liver insufficiency
- Spectrum: subtle sleep/personality changes → confusion/disorientation → stupor → coma
Goldman-Cecil Medicine; Robbins & Kumar Basic Pathology
4. Viral Hepatitis
| Feature | Hep A | Hep B | Hep C | Hep D | Hep E |
|---|---|---|---|---|---|
| Transmission | Fecal-oral | Parenteral/sexual/vertical | Parenteral | Parenteral (requires HBV) | Fecal-oral |
| Chronicity | None | 5-10% adults | 75-85% | Co-infection: <5%; Superinfection: >70% | None (except immunocompromised) |
| Vaccine | Yes | Yes | No | HBV vaccine prevents | No (in most countries) |
| Key antigen | HAV IgM | HBsAg | Anti-HCV Ab | HDV Ag | HEV IgM |
Chronic Hepatitis B
- Defined as HBsAg persistence for ≥6 months
- Phases: immune tolerant → immune active → inactive carrier → reactivation
- HBV DNA PCR useful for diagnosing early infection (before HBsAg appears), distinguishing active vs. inactive infection, and monitoring treatment response
- Treatment: nucleos(t)ide analogues (tenofovir, entecavir) - viral suppression but rarely cure
Chronic Hepatitis C
- Most common cause of chronic liver disease in many regions
- HCV RNA PCR for confirmation; genotype guides treatment duration
- Treatment: direct-acting antivirals (DAAs) achieve >95% sustained virologic response (SVR = functional cure)
Robbins & Kumar; Yamada's Textbook of Gastroenterology, 7th ed.
5. Steatotic Liver Disease
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) / formerly NAFLD
- Most common chronic liver disease worldwide, affecting ~30% of adults
- Spectrum: simple steatosis → metabolic dysfunction-associated steatohepatitis (MASH/NASH) → fibrosis → cirrhosis → HCC
- Diagnosis: steatosis on imaging or histology, after exclusion of excessive alcohol use
- Histology: macrovesicular steatosis affecting ≥5% of hepatocytes; NASH requires additional ballooning degeneration and lobular inflammation
- Liver biopsy required to distinguish NASH from simple steatosis
- Risk factors: obesity, type 2 diabetes, metabolic syndrome, dyslipidemia
- Management: weight loss (≥7-10% body weight), exercise, treatment of metabolic comorbidities; resmetirom (thyroid receptor-beta agonist) is the first FDA-approved drug for MASH with fibrosis (2024); semaglutide updated into AASLD guidance for MASH in November 2025
Alcoholic/Alcohol-Associated Liver Disease (ALD)
- Spectrum: alcoholic fatty liver (steatosis) → alcoholic hepatitis → alcoholic cirrhosis
- Alcoholic hepatitis: acute presentation with jaundice, fever, tender hepatomegaly, leukocytosis; AST:ALT ratio typically >2:1
- Maddrey Discriminant Function (DF) >32 indicates severe disease - consider corticosteroids
- Abstinence is the cornerstone of all treatment
Robbins, Cotran & Kumar Pathologic Basis of Disease; Yamada's Textbook of Gastroenterology; AASLD 2025
6. Acute Liver Failure (ALF)
Definition: INR ≥1.5 + hepatic encephalopathy in a patient without pre-existing chronic liver disease (onset within 26 weeks of initial liver injury). - Yamada's Textbook of Gastroenterology, 7th ed.
Causes (by frequency in Western countries)
- Acetaminophen overdose (most common in US/UK)
- Hepatitis A, B, C, D, E
- Drug-induced liver injury (DILI)
- Autoimmune hepatitis
- Wilson disease
- Budd-Chiari syndrome
Key Clinical Features
- Rapid onset of encephalopathy + coagulopathy (INR >1.5)
- Cerebral edema (life-threatening in acute vs. chronic liver failure)
- Multi-organ failure: renal failure, respiratory failure, hypoglycemia, coagulopathy
Management Priorities
- Acetaminophen: N-acetylcysteine (NAC) - works even in late presentation
- Supportive ICU care: intracranial pressure monitoring, lactulose/rifaximin for HE, vasopressors, renal replacement therapy
- Liver transplantation: definitive therapy; King's College Criteria guide listing decision
Goldman-Cecil Medicine; Robbins & Kumar
7. Autoimmune & Cholestatic Diseases
Autoimmune Hepatitis (AIH)
- Predominantly in women; elevated IgG, positive ANA/ASMA (Type 1) or anti-LKM-1 (Type 2)
- Treatment: prednisolone ± azathioprine; remission in >80%
Primary Biliary Cholangitis (PBC)
- Anti-mitochondrial antibody (AMA) positive in >90%
- Granulomatous destruction of small intrahepatic bile ducts
- Treatment: ursodeoxycholic acid (UDCA); obeticholic acid for inadequate UDCA response
Primary Sclerosing Cholangitis (PSC)
- Strong association with inflammatory bowel disease (especially ulcerative colitis)
- Multifocal strictures of intra- and extrahepatic bile ducts on MRCP ("beaded" appearance)
- Risk of cholangiocarcinoma (10-15% lifetime risk)
- No effective medical therapy; liver transplantation for end-stage disease
8. Key Laboratory Investigations
| Test | What it reflects |
|---|---|
| ALT, AST | Hepatocellular injury; AST:ALT >2 suggests ALD |
| ALP, GGT | Cholestatic injury |
| Bilirubin (conjugated/unconjugated) | Distinguish hepatocellular vs. cholestatic vs. hemolytic jaundice |
| Albumin, INR/PT | Synthetic function (marker of severity) |
| Platelet count | Portal hypertension/hypersplenism |
| Serum ammonia | Hepatic encephalopathy |
| AFP | HCC screening in cirrhosis |
| Fibroscan/FIB-4/ELF score | Non-invasive fibrosis assessment; ELF ≥9.8 predicts progression to cirrhosis |
9. Liver Transplantation
Indications: end-stage liver disease (MELD score guided), acute liver failure, hepatocellular carcinoma (Milan criteria).
Diseases that recur post-transplant: chronic hepatitis B and C, PBC, PSC, autoimmune hepatitis, alcoholic liver disease, NAFLD/MASLD, Budd-Chiari syndrome, HCC. - Bailey and Love's Short Practice of Surgery, 28th ed.
Key Sources:
- Harrison's Principles of Internal Medicine, 22E (2025)
- Goldman-Cecil Medicine, 27th ed.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Yamada's Textbook of Gastroenterology, 7th ed.
- AASLD Practice Guidance on MASLD (2023, updated 2025) - includes November 2025 semaglutide update and 2024 resmetirom approval
- EASL Clinical Practice Guidelines - covers HBV, HCC, autoimmune hepatitis, liver transplantation
This is a shared conversation. Sign in to Orris to start your own chat.