Non-infectious pulmonary complications of hematopoietic cell transplantation full details for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hematopoietic stem cell transplantation" AND "pulmonary complications" AND "non-infectious"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from both textbooks covering all the major non-infectious pulmonary complications of HCT. Let me compile the full, structured 10-mark MD exam answer.
Non-Infectious Pulmonary Complications of Hematopoietic Cell Transplantation
(Sources: Fishman's Pulmonary Diseases and Disorders, Ch. 94; Murray & Nadel's Textbook of Respiratory Medicine, Ch. 125; 2025 Review, Respir Med PMID 40902833)
Introduction
Hematopoietic cell transplantation (HCT) - both autologous and allogeneic - is a potentially curative therapy for hematologic malignancies, aplastic anemia, autoimmune disorders, and selected solid tumors. Pulmonary complications affect 30-60% of HCT recipients and are among the leading causes of transplant-related morbidity and mortality. Non-infectious complications are organized by the triphasic temporal framework of immune reconstitution:
| Phase | Timing | Immune Status |
|---|---|---|
| Peri-engraftment | 0-30 days | Profound neutropenia |
| Early post-engraftment | 30-100 days | Impaired cell-mediated immunity; risk of acute GVHD |
| Late post-engraftment | >100 days | Combined cell-mediated + humoral defects; chronic GVHD |
EARLY COMPLICATIONS (<100 days)
1. Peri-Engraftment Respiratory Distress Syndrome (PERDS)
Timing: Within 5 days either side of neutrophil engraftment (ANC first reaching >500 cells/mm³ for 3 consecutive days)
Pathogenesis: Cytokine storm and inflammatory mediator release triggered by engraftment - the sudden influx of activated donor neutrophils causes capillary leak and lung injury.
Diagnostic Criteria (all four required):
- New bilateral pulmonary infiltrates
- Hypoxemia
- Syndrome not fully explained by infection, fluid overload, or cardiac failure
- Occurring within 5 days on either side of the engraftment date
Clinical features: Fever, weight gain (fluid retention), hypoxemia, bilateral alveolar opacities. Skin rash and jaundice (hepatic congestion) may coexist.
Treatment: High-dose corticosteroids (methylprednisolone 0.5-1 mg/kg/d); supportive care; diuresis; lung-protective ventilation if intubated.
Prognosis: Generally favorable; mortality <10% with early treatment.
2. Idiopathic Pneumonia Syndrome (IPS)
Definition: A non-infectious, diffuse alveolar injury with multilobar involvement after HCT - essentially exclusion-based ARDS with no identified pathogen.
Diagnostic Criteria (all five required):
- Multilobar opacities on chest X-ray or CT
- Signs and symptoms of pneumonia (fever, cough, dyspnea)
- Abnormal pulmonary physiology: elevated A-a gradient or supplemental O2 requirement
- Absence of lower respiratory tract infection on BAL
- Syndrome not fully explained by fluid overload or cardiac failure
Pathogenesis: Conditioning-regimen injury (total body irradiation + chemotherapy) to alveolar epithelium + endothelium, followed by an alloreactive donor T-cell inflammatory response. BAL typically shows a lymphocytic alveolitis.
Incidence: 2-8% of allogeneic HCT recipients; rare in autologous HCT.
CT findings: Bilateral ground-glass opacities and consolidation, often with a diffuse alveolar damage (DAD) pattern.
Treatment:
- High-dose systemic corticosteroids are the mainstay
- Etanercept (anti-TNF) combined with corticosteroids showed early promise in a Phase II trial (BMT CTN 0403), with improved 28-day survival to 73% vs. historical controls
- Lung-protective ventilation; avoid fluid overload
Prognosis: Mortality remains high (50-80% in mechanically ventilated patients).
3. Diffuse Alveolar Hemorrhage (DAH)
Definition: Alveolar filling with red cells from the pulmonary microvasculature - classified as definite or probable.
Diagnostic Criteria:
- Respiratory failure requiring O2/ventilation
- Bilateral pulmonary infiltrates on imaging
- Definite DAH: Both (a) progressively bloodier return on sequential BAL aliquots AND (b) ≥20% hemosiderin-laden macrophages on cytology
- Probable DAH: Criteria above + only one of (a) or (b)
Pathogenesis: Endothelial injury from conditioning regimen (chemotherapy/TBI); thrombocytopenia amplifies bleeding. More common after autologous HCT (possibly due to myeloablative regimens) and in the peri-engraftment period.
Clinical features: Acute onset dyspnea + hypoxemia; hemoptysis present in only ~20%; dropping hemoglobin despite no external bleeding is a clue.
Radiology: Bilateral alveolar consolidation/ground-glass opacities; CT shows "crazy paving" or bat-wing pattern.
Treatment:
- High-dose corticosteroids (methylprednisolone 500-1000 mg IV)
- Aggressive platelet support (target >50,000)
- rFactor VIIa and aminocaproic acid (antifibrinolytic) used in refractory cases
- IVIG in some protocols
Prognosis: Mortality 60-100% in those requiring mechanical ventilation.
4. Pulmonary Edema
Acute pulmonary edema affects ~5% of autologous HSCT recipients. Pre-existing cardiotoxicity (cyclophosphamide, anthracyclines, prior radiation), endothelial injury from conditioning, aggressive IV fluid administration during mucositis management, and engraftment-related capillary leak all contribute. Management is standard: diuresis, optimization of hemodynamics.
5. Engraftment Syndrome
Closely related to PERDS. Characterized by fever, rash, and non-cardiogenic pulmonary edema occurring during engraftment. Capillary leak from TNF-α, IL-1, and IL-6 release. Responds rapidly to high-dose corticosteroids.
LATE COMPLICATIONS (>100 days)
6. Bronchiolitis Obliterans Syndrome (BOS) - The Most Important Late Complication
Definition: Progressive obliterative bronchiolitis affecting small airways, representing the pulmonary manifestation of chronic GVHD.
Incidence: 2-6% of allogeneic HCT recipients; accounts for substantial late mortality.
NIH Chronic GVHD Consensus Diagnostic Criteria (2014) - all four must be met:
- FEV1/VC <0.7 or below the lower limit of normal
- FEV1 <75% predicted with ≥10% decline over <2 years, not reversible with bronchodilator
- Absence of respiratory tract infection
- At least ONE supporting feature:
- (A) Air trapping on expiratory CT (mosaic attenuation) or hyperinflation
- (B) Residual volume >120% predicted on plethysmography
- (C) Pathological confirmation of constrictive bronchiolitis on biopsy
Pathogenesis: Donor cytotoxic T lymphocytes (CD8+) target host bronchiolar epithelium as part of a GVHD immune response. Donor B-cell alloantibody response also plays a role. Results in submucosal fibrous obliteration of bronchiolar lumen - histology shows constrictive bronchiolitis.
Risk Factors:
- Concomitant extrathoracic chronic GVHD (present in 100% of cases in some series)
- Busulfan-based conditioning regimen
- Peripheral blood stem cell (vs. bone marrow or cord blood) source
- Older donor/recipient age
- Female-to-male transplant
- Acute GVHD history
- Methotrexate use
Protective factors: T-cell depletion with antithymocyte globulin; cord blood transplant
Clinical Features:
- Insidious dyspnea, non-productive cough, exercise intolerance, wheezing
- Up to 20% are asymptomatic at the time of first spirometric abnormality
- Wheezing on exam in ~40%
Radiology:
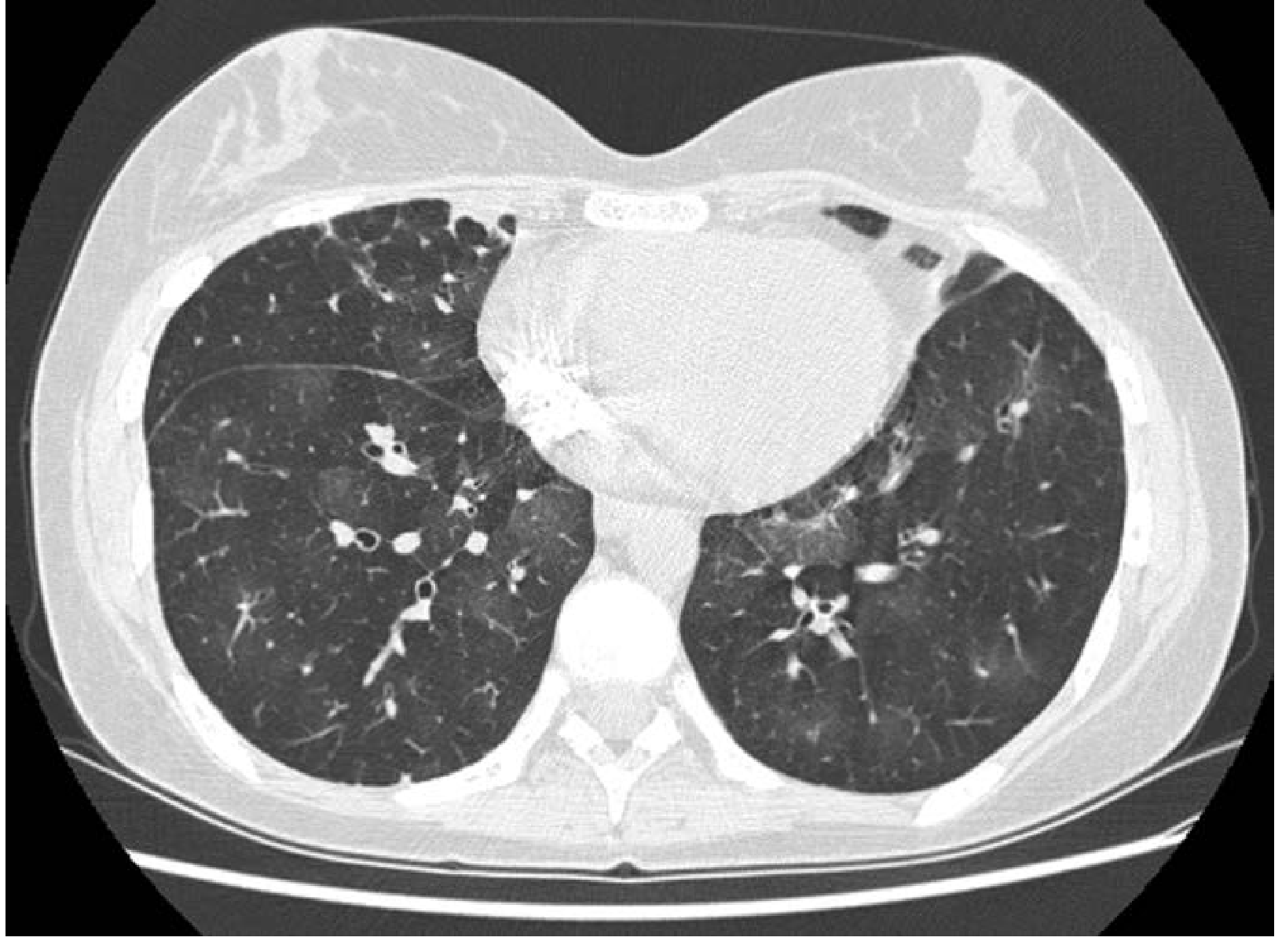
Expiratory CT chest in BOS post-HSCT: mosaic attenuation (darker areas = air trapping), bronchial wall thickening, and mild bronchiectasis (Fishman's, Ch. 94)
- Chest X-ray: normal or hyperinflation
- HRCT (expiratory cuts): mosaic attenuation (air trapping), bronchial wall thickening, bronchiectasis
- Early disease: CT may be normal
Pulmonary Function Tests: Obstructive pattern - reduced FEV1, reduced FEV1/FVC, increased RV and TLC; DLCO may be reduced.
Treatment:
| Agent | Evidence/Role |
|---|---|
| Inhaled corticosteroid + LABA (budesonide/formoterol) | First-line; RCT showed +260 mL FEV1 at 1 month vs +5 mL placebo |
| Systemic prednisone (1-1.5 mg/kg/d) | First-line systemic; taper over months |
| Fluticasone + Montelukast (FAM regimen) | Modest stabilization data; montelukast not routinely recommended |
| Azithromycin | Avoid - ALLOZITHRO trial showed increased relapse + worse survival |
| Extracorporeal photopheresis (ECP) | 50-65% response in steroid-refractory chronic GVHD; promising |
| Cyclosporine, tacrolimus, MMF | Steroid-sparing options in refractory cases |
| Lung transplantation | Last resort in end-stage BOS without active malignancy |
Prognosis: Progressive and often irreversible; 5-year survival ~50% after diagnosis.
7. Cryptogenic Organizing Pneumonia (COP) / Bronchiolitis Obliterans Organizing Pneumonia (BOOP)
Timing: Late post-HCT (>100 days), associated with chronic GVHD.
Pathogenesis: Inflammatory plugs of granulation tissue fill alveolar ducts and alveoli (Masson bodies). May represent GVHD targeting alveolar epithelium, or a reaction to conditioning injury.
Clinical features: Subacute onset fever, dry cough, dyspnea; bibasal crackles.
Radiology: Bilateral peripheral patchy consolidations (peribronchovascular distribution); reverse halo (atoll sign) on CT is characteristic. Restrictive pattern on PFTs; reduced DLCO.
Treatment: High-dose corticosteroids (prednisone 1 mg/kg/d) - excellent response; relapse common on tapering.
8. Pulmonary Veno-Occlusive Disease (PVOD) / Pulmonary Arterial Hypertension
Timing: Late complication; underrecognized.
Pathogenesis: Obliterative fibrous remodeling of pulmonary venules and small veins. Associated with conditioning chemotherapy (especially alkylating agents like busulfan, cyclophosphamide), TBI, and chronic GVHD. Endothelial injury with fibrous occlusion of pulmonary venules.
Clinical features: Progressive exertional dyspnea, fatigue, signs of right heart failure (elevated JVP, peripheral edema, loud P2).
Radiology/investigations: CT shows centrilobular ground-glass nodules, septal lines, mediastinal lymphadenopathy. Echocardiography: elevated PASP. Right heart catheterization: elevated PAP, low PCWP (distinguishes from cardiogenic causes).
Treatment: Pulmonary vasodilators (sildenafil, prostacyclins); avoid aggressive vasodilator therapy in true PVOD (risk of flash pulmonary edema). Lung transplant in end-stage disease.
9. Radiation-Induced Lung Injury (Post-TBI)
Total body irradiation (TBI) used in myeloablative conditioning causes radiation pneumonitis and late pulmonary fibrosis.
Two phases:
| Phase | Timing | Features |
|---|---|---|
| Radiation Pneumonitis | 1-3 months post-TBI | Fever, dry cough, dyspnea; GGO on CT in radiation field |
| Radiation Fibrosis | 6-24 months | Progressive fibrotic restriction; traction bronchiectasis; "honeycomb" on CT |
Risk factors: TBI dose >10 Gy, prior chemotherapy, lung dose >8 Gy, pre-existing lung disease.
Treatment: Corticosteroids in acute pneumonitis phase; supportive care in fibrosis.
10. Drug-Induced Pulmonary Toxicity
Multiple agents used in conditioning and post-HCT management cause lung injury:
| Drug | Pulmonary Toxicity |
|---|---|
| Busulfan | Diffuse alveolar damage / fibrosis; "busulfan lung" |
| Cyclophosphamide | Hemorrhagic cystitis (systemic); acute lung injury; late fibrosis |
| Carmustine (BCNU) | Subacute/late fibrosis; dose-dependent |
| Bleomycin | Hypersensitivity pneumonitis → fibrosis |
| Methotrexate | Hypersensitivity pneumonitis; eosinophilic alveolitis |
| Sirolimus (mTOR inhibitor) | Lymphocytic/eosinophilic alveolitis; OP pattern; 11% incidence in kidney Tx |
| Cyclosporine | Capillary leak; ARDS |
| Tacrolimus | Cryptogenic OP |
11. Restrictive Lung Dysfunction and ILD
Late-onset restrictive dysfunction can arise from:
- Interstitial lung disease (ILD) as a chronic GVHD manifestation
- Truncal sclerosis from extrapulmonary chronic GVHD (scleroderma-like)
- Organizing pneumonia (see above)
- Radiation fibrosis
PFTs show reduced TLC, VC, DLCO with preserved FEV1/FVC ratio.
Summary Table: Non-Infectious Pulmonary Complications of HCT
| Complication | Phase | Key Features | Treatment |
|---|---|---|---|
| PERDS | Peri-engraftment (<30d) | Bilateral infiltrates within ±5 days of ANC engraftment | Corticosteroids, diuretics |
| Pulmonary edema | <30 days | Cardiogenic or non-cardiogenic; fluid overload | Diuresis, cardiac support |
| Engraftment syndrome | Peri-engraftment | Fever + rash + non-cardiogenic edema | Corticosteroids |
| IPS | 30-100 days | Diffuse lung injury, negative BAL | Corticosteroids ± etanercept |
| DAH | 30-100 days | Progressive BAL hemorrhage, ≥20% hemosiderin macrophages | High-dose CS, platelets, rFVIIa |
| BOS | >100 days | Obstructive FEV1↓, air trapping, chronic GVHD | ICS/LABA, ECP, avoid azithromycin |
| COP/BOOP | >100 days | Peripheral consolidation, restrictive, reverse halo | Prednisone (good response) |
| PVOD/PAH | >100 days | Right heart failure, elevated PAP, low PCWP | Vasodilators, lung Tx |
| Radiation fibrosis | 6-24 months | Field-limited fibrosis post-TBI | Supportive; CS in acute phase |
| Drug-induced ILD | Variable | Specific to conditioning agent | Discontinue agent, CS |
High-Yield Points for MD Exam
- BOS = pulmonary chronic GVHD - obstructive pattern, NIH criteria require FEV1 <75% + air trapping on CT; avoid azithromycin (ALLOZITHRO trial harm).
- IPS vs DAH vs PERDS - all overlap clinically; differentiation is by timing (PERDS = ±5 days engraftment), BAL findings (DAH = bloody, progressive), and absence of infection (IPS = clean BAL).
- DAH - hemoptysis is absent in ~80%; diagnosis is bronchoscopic; mortality very high with MV.
- PERDS and engraftment syndrome - cytokine-mediated; rapid response to corticosteroids is both diagnostic and therapeutic.
- BOS risk factor: 100% of affected patients have chronic GVHD; peripheral blood stem cell source > cord blood.
- Busulfan lung = late-onset fibrosis; BCNU/carmustine = dose-dependent pulmonary fibrosis.
- PVOD post-HCT is distinguished from left heart failure by low PCWP on right heart catheterization.
- COP - most steroid-responsive of all; bilateral peripheral consolidation with "atoll sign" on CT.
References: Fishman's Pulmonary Diseases and Disorders (5th ed.), Ch. 94; Murray & Nadel's Textbook of Respiratory Medicine, Ch. 125; Bertini C et al., "Noninfectious pulmonary complications after hematopoietic cell transplantation: a comprehensive review," Respir Med, 2025 [PMID 40902833]
This is a shared conversation. Sign in to Orris to start your own chat.