hernia.(elaborate)
Reading File
Finding Sources
Searching PubMed
"hernia"[MeSH Terms] AND "repair"[MeSH Terms]
Searching Images
hernia types anatomy inguinal umbilical femoral
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all I need to compile a thorough, well-structured answer.
Hernia — Comprehensive Overview
Definition
A hernia is the protrusion of a viscus, or part of a viscus, through an abnormal opening in the wall of the cavity in which it is normally contained. The opening may be congenital or acquired, and the protruding content is enclosed within a sac of peritoneum (except in sliding hernias where the sac wall is partly formed by the viscus itself).
Classification
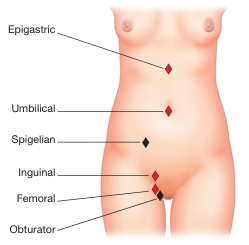
By Location
| Type | Site | Notes |
|---|---|---|
| Inguinal (indirect) | Through deep inguinal ring, along inguinal canal | Most common overall; congenital or acquired |
| Inguinal (direct) | Through Hesselbach's triangle, medial to inferior epigastric vessels | Acquired; due to posterior wall weakness |
| Femoral | Through femoral canal, below inguinal ligament | More common in women; high strangulation risk |
| Umbilical | Through umbilical ring | Congenital (resolves by age 5) or acquired (obesity, ascites) |
| Epigastric | Through linea alba above umbilicus | Usually small, contains preperitoneal fat |
| Spigelian | Lateral edge of rectus muscle, below umbilicus | Rare; risk of strangulation |
| Incisional | Through prior surgical wound | Occurs in ~20% post-laparotomy |
| Parastomal | Adjacent to stoma | Related to stoma formation |
| Hiatal | Stomach herniates through esophageal hiatus | Sliding (most common) vs. para-oesophageal |
| Diaphragmatic | Abdominal contents through diaphragm | Congenital (Bochdalek, Morgagni) or traumatic |
| Obturator | Through obturator canal | Rare; "little old lady" hernia; can compress obturator nerve (Howship–Romberg sign) |
| Internal | Through peritoneum, mesentery, or omentum | Paraduodenal, foramen of Winslow, iatrogenic (post-RYGB) |
| Pantaloon | Combined direct + indirect inguinal hernia | Straddles inferior epigastric vessels |
| Richter's | Only part of bowel wall is incarcerated | Can strangulate WITHOUT complete obstruction |
By Reducibility / Clinical Status
| Term | Definition |
|---|---|
| Reducible | Contents return spontaneously or manually to normal position |
| Irreducible / Incarcerated | Cannot be reduced; no compromise of blood supply per se |
| Obstructed | Incarcerated bowel causes luminal obstruction |
| Strangulated | Ischaemia of the hernial contents due to constriction at the neck |
"Strangulation occurs when any degree of ischaemia or obstruction results from compression of a loop of bowel within the neck of a hernia." — Sleisenger & Fordtran's GI and Liver Disease, p. 2494
Risk of strangulation is inversely proportional to the size of the hernia neck: small-necked hernias (femoral, umbilical) carry the highest risk.
Epidemiology & Risk Factors
- Inguinal hernias are ~10× more common in men than women.
- Femoral hernia is relatively more common in women, though inguinal hernias still predominate in women too.
- Right side more common than left for indirect inguinal (due to later descent of the right testis).
- Risk factors include: male sex, advanced age, previous hernia/repair, connective tissue disorders, increased intra-abdominal pressure (chronic cough, constipation, prostatism, heavy lifting, obesity, ascites, pregnancy), and prior abdominal surgery.
Anatomy of the Inguinal Canal
The inguinal canal is central to understanding groin hernias.
- Deep (internal) inguinal ring: Defect in transversalis fascia, lies midway between anterior superior iliac spine (ASIS) and pubic tubercle, 2–3 cm above and lateral to the femoral artery pulse; inferior epigastric vessels lie just medial to it.
- Superficial (external) inguinal ring: Inverted-V defect in external oblique aponeurosis, just above and lateral to pubic tubercle.
- Conjoint tendon: Fusion of transversus abdominis and internal oblique muscles; forms the posterior wall medially.
- Hesselbach's triangle: Bounded by inferior epigastric vessels (lateral), inguinal ligament (inferior), rectus sheath (medial) — site of direct hernia.
- Indirect hernia passes lateral to inferior epigastric vessels, through the deep ring, along the canal.
- Direct hernia passes medial to inferior epigastric vessels, through Hesselbach's triangle.

Pathophysiology
Indirect Inguinal Hernia
Caused by patent processus vaginalis — a finger-like peritoneal projection that accompanies the testis during descent. Failure of closure allows peritoneal contents to enter the inguinal canal. ~90% of boys with undescended testis have a patent processus vaginalis. All congenital hernias are indirect.
Direct Inguinal Hernia
Results from acquired weakness of the posterior inguinal wall (transversalis fascia) in Hesselbach's triangle. Associated with ageing, chronic raised intra-abdominal pressure, and connective tissue disorders.
Femoral Hernia
Protrudes through the femoral canal (medial to the femoral vein, lateral to the lacunar ligament). The small, rigid canal means incarceration occurs in up to 45% of cases — the highest among common hernias.
Hiatal Hernia
Stomach herniates through the oesophageal hiatus. Promotes GERD by:
- Displacing the LES above the diaphragm → reduced LES pressure
- Eliminating the "pinch-cock" mechanism of the crural diaphragm
- Creating an acid pocket in the hernia sac that acts as a reservoir for acid reflux
- Large (≥3 cm), non-reducible hernias are especially prone to reflux.
Clinical Features
| Feature | Indirect Inguinal | Direct Inguinal | Femoral |
|---|---|---|---|
| Age | Any (common in infants & young men) | Middle-aged/elderly men | Middle-aged women |
| Position of swelling | Above and medial to pubic tubercle | Above and medial to pubic tubercle | Below inguinal ligament, medial thigh |
| Control on pressure | Controlled at deep ring (lateral to epigastric vessels) | Not controlled at deep ring | Not controlled |
| Reducibility | Usually reducible | Usually reducible | Often irreducible |
| Strangulation risk | Moderate (higher with small neck) | Low (wide neck) | Very high (up to 45%) |
Symptoms:
- Dragging or aching discomfort in the groin, especially on standing or straining.
- Visible/palpable bulge that enlarges on coughing (cough impulse).
- Sudden severe pain + irreducibility = incarceration/strangulation — surgical emergency.
Incisional hernias occur in ~20% of patients after abdominal surgery; poor wound healing (e.g., infection) is the major risk factor.
Investigations
- Diagnosis is primarily clinical in most cases.
- USS: Useful for groin hernias, especially in obese patients or when diagnosis is uncertain; useful for distinguishing inguinal hernia from femoral hernia, hydrocele, or lymphadenopathy.
- CT scan: Gold standard for complex or internal hernias; identifies incarceration and strangulation; required in obese patients where clinical examination is unreliable. CT in Roux-en-Y gastric bypass patients should specifically look for internal hernia through mesenteric defects.
- MRI/MRI herniography: Occasionally used for occult hernias.
Special Hernia Types
Richter's Hernia
Only part of the bowel wall is caught in the hernia neck — the bowel can strangulate and undergo necrosis without causing complete intestinal obstruction. Most common in femoral and inguinal hernias.
Maydl's Hernia (Hernia-en-W)
Two loops of bowel are in the sac with an intervening loop inside the abdomen — the segment inside the abdomen can strangulate without any visible signs.
Pantaloon Hernia
Combination of direct + indirect hernia straddling the inferior epigastric vessels; difficult to diagnose pre-operatively, often found at surgery.
Sliding Hernia
Part of the sac wall is formed by a viscus (e.g., sigmoid colon on the left, caecum on the right); sac cannot be ligated in the conventional fashion.
Parastomal Hernia
Bowel herniates alongside a stoma through the fascia; accounts for 15% of emergency hernia surgery, with up to 60% showing strangulation at operation.
Internal Hernias
Through peritoneal, mesenteric, or omental defects. Most common iatrogenic type is through mesenteric defects after Roux-en-Y gastric bypass, colectomy, or pancreaticoduodenectomy. Congenital types: paraduodenal (most common), foramen of Winslow.
Complications
- Incarceration — Irreducible contents; may not compromise blood supply initially.
- Obstruction — Incarcerated bowel causing small bowel obstruction (SBO). Hernia is the second most common cause of SBO (after adhesions) in the West but has a higher rate of strangulation per episode than adhesions.
- Strangulation — Ischaemia/necrosis of contents; surgical emergency. Up to 75% of hernias causing SBO have associated intestinal ischaemia; >25% have intestinal necrosis.
- Incisional hernia recurrence — Open suture repairs: 20–50% recurrence.
Treatment
Conservative
- Watchful waiting for minimally symptomatic inguinal hernias in men (acceptable as initial approach; annual risk of acute incarceration ~0.2–0.3% per year for non-strangulated hernias).
- Never watchful waiting for femoral hernias (too high a risk of strangulation).
- Trusses: Largely obsolete; not recommended for definitive management.
Open Surgical Repair
| Operation | Principle |
|---|---|
| Herniotomy | Sac ligation only; used in children (processus closure) |
| Bassini | Tissue repair — conjoint tendon sutured to inguinal ligament |
| Shouldice | Multi-layer tissue repair; low recurrence in specialist centres (~1%) |
| Lichtenstein | Tension-free flat mesh repair; recurrence <1%; current gold standard for open repair |
| Plug & patch | Not recommended; higher complication rates |
| Stoppa (GPRVS) | Giant prosthetic reinforcement of visceral sac; bilateral hernias |
Laparoscopic Repair
Two approaches — both reduce hernia from behind and place a large mesh (≥10 × 15 cm) in the preperitoneal plane, covering Hesselbach's triangle, deep inguinal ring, and femoral canal:
- TEP (Totally Extraperitoneal): Surgeon develops the extraperitoneal plane without entering the peritoneal cavity.
- TAPP (Transabdominal Preperitoneal): Enter the peritoneal cavity first; incise peritoneum above the hernia defect.
Advantages over open:
- Less post-operative pain (short- and long-term)
- Faster return to normal activity
- Fewer wound complications
- Particularly beneficial for bilateral and recurrent hernias
Robotic repair is increasingly used; comparable outcomes but higher cost, with no proven patient benefit over standard laparoscopy for simple repairs.
Emergency Management (Incarcerated/Strangulated)
- Urgent resuscitation and antibiotics.
- Attempt manual reduction only if no signs of strangulation (no skin erythema, severe tenderness, systemic toxicity) — contraindicated if strangulation suspected.
- Emergency surgery: hernia reduction, bowel viability assessment; resection if necrotic.
- Mesh use in contaminated field is controversial — clean cases: mesh acceptable; contaminated (bowel resection/perforation): tissue repair preferred for primary repair, mesh reserved for later.
Paediatric Considerations
- All congenital inguinal hernias in children are indirect (patent processus vaginalis).
- Incidence higher in premature neonates.
- Incarceration risk is higher in infants due to narrow inguinal ring.
- Operation = herniotomy (sac ligation only); no floor repair needed as the posterior wall is normal.
- Umbilical hernias commonly resolve by age 5 without treatment; surgery if persists beyond 5 years, >2 cm, or incarcerated.
Hernia and Small Bowel Obstruction (SBO)
Hernia is the second most common cause of SBO in the West, after adhesions. Femoral hernias are strangulated in up to 40% of presentations vs. only 2% of incisional hernias and ~60% of umbilical hernias that require emergency surgery. The declining proportion of SBO due to hernia in Western countries reflects the widespread practice of elective hernia repair. — Sleisenger & Fordtran, p. 2494
Summary of Key Numbers
| Fact | Figure |
|---|---|
| Incisional hernia after laparotomy | ~20% |
| Femoral hernia incarceration rate | Up to 45% |
| Umbilical hernia strangulation (emergency) | Up to 60% |
| Inguinal hernia: male:female ratio | ~10:1 |
| Open suture repair recurrence | 20–50% |
| Lichtenstein/laparoscopic recurrence | <1% |
| SBO from incarcerated hernia → intestinal ischaemia | Up to 75% |
| SBO from incarcerated hernia → intestinal necrosis | >25% |
Sources: Bailey and Love's Short Practice of Surgery 28th ed., p. 1086–1091 | Sleisenger & Fordtran's GI and Liver Disease, p. 2493–2496 | Schwartz's Principles of Surgery 11th ed., p. 1771 | Mulholland & Greenfield's Surgery 7th ed., p. 2430 | Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1039–1040
This is a shared conversation. Sign in to Orris to start your own chat.