hi
Hey! How can I help you today?
hyperkalemia step by step treatment
Reading File
Finding Sources
Searching PubMed
hyperkalemia management treatment
Reading File
Reading File
Reading File
Loading Image
Here is a complete step-by-step guide to hyperkalemia treatment, organized by urgency:
Hyperkalemia: Step-by-Step Treatment
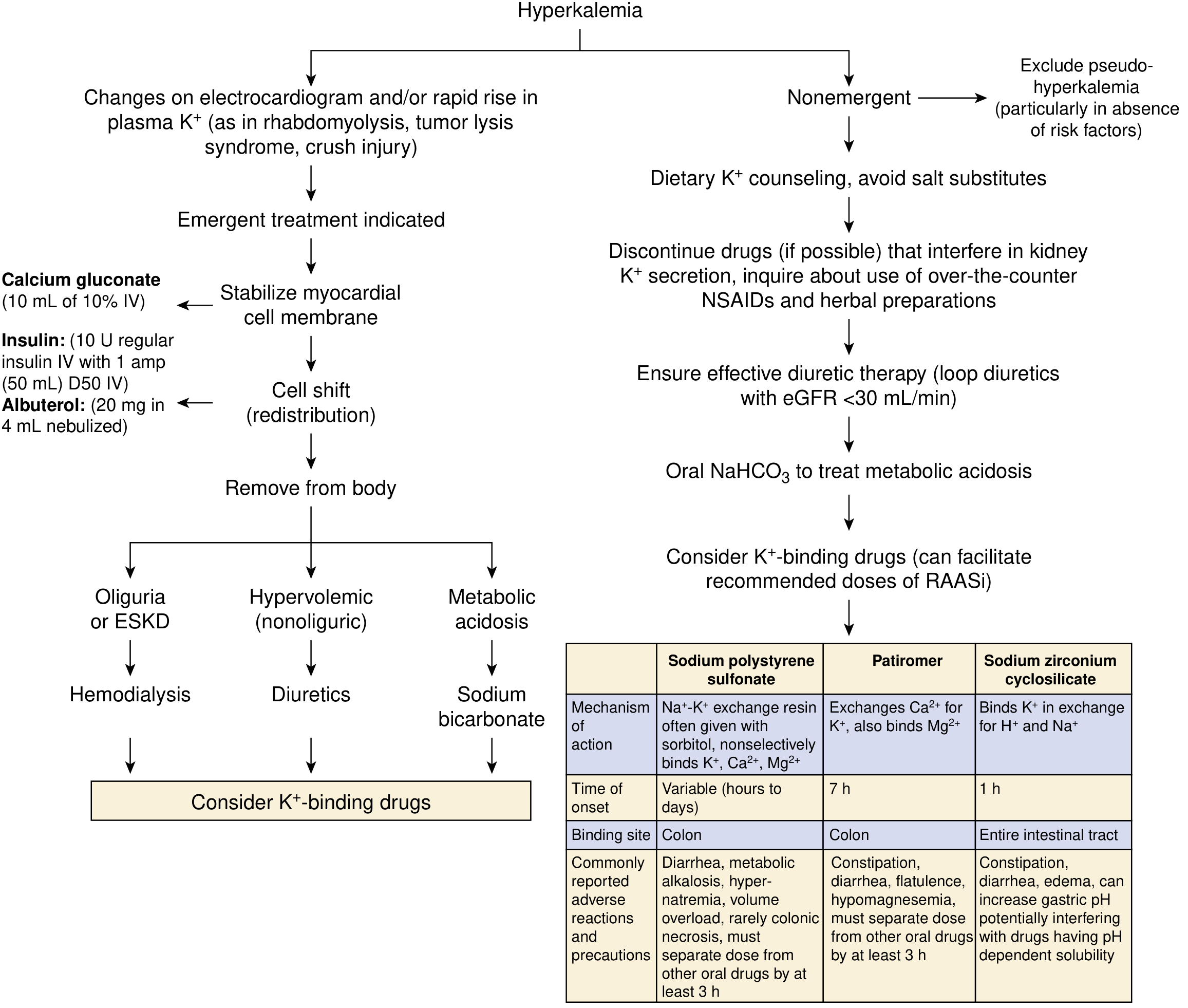
- National Kidney Foundation Primer on Kidney Diseases, 8e
First: Stop All Potassium Input
- Discontinue all IV potassium infusions, K+-containing fluids, and oral potassium supplements immediately.
EMERGENT TREATMENT
(K+ >6-6.5 mEq/L or ECG changes present)
Step 1 - Stabilize the Cardiac Membrane
Goal: Protect the heart NOW (does not lower K+)
| Drug | Dose | Onset | Notes |
|---|---|---|---|
| Calcium gluconate 10% | 10 mL IV over 1-3 min | Immediate | Repeat in 3-5 min if no ECG improvement |
| Calcium chloride 10% | 10 mL IV over 10 min | Immediate | More elemental Ca2+; risk of skin necrosis if peripheral line - prefer central access |
- ECG changes requiring immediate calcium: peaked T waves, widened QRS, loss of P waves, sine wave pattern.
- Calcium does not lower K+ - it only raises the threshold for cardiac excitability.
Step 2 - Shift K+ Into Cells
Goal: Rapidly lower plasma K+ within 15-60 min
(a) Insulin + Glucose - fastest option
- Regular insulin 10 units IV + 50 mL of 50% dextrose (D50) as a bolus
- Follow with D5W at 100 mL/hr to prevent late hypoglycemia
- Onset: 15 minutes; monitor blood glucose closely
- If glucose >300 mg/dL (diabetic): give insulin alone, without dextrose
- Never give dextrose alone - can paradoxically worsen hyperkalemia by osmotic K+ shift
(b) Albuterol (beta-2 agonist) - additive to insulin
- 20 mg nebulized over 10 minutes (concentrated 5 mg/mL solution)
- Onset: 30 minutes
- Note: this dose is much higher than asthma dosing
- Effect is additive to insulin - use both together for maximum K+ lowering
(c) Sodium Bicarbonate - limited role
- 50-100 mEq IV over 10-20 min
- Useful only if severe metabolic acidosis (HCO3- <10 mmol/L) or in non-dialysis patients
- Does NOT enhance insulin or albuterol effects
- Little benefit in patients without residual kidney function
Step 3 - Remove K+ From the Body
Goal: Definitive reduction - these are slower but lasting
| Method | When to use | Details |
|---|---|---|
| Loop/thiazide diuretics | Adequate kidney function present | Furosemide preferred |
| Hemodialysis | No kidney function (AKI/ESKD) or oliguria | Most effective; can't always initiate quickly enough to replace steps 1-2 |
| Potassium binders | Adjunct after emergency measures; chronic prevention | See below |
Potassium Binders (Comparison)
| Drug | Mechanism | Onset | Dose | Key Adverse Effects |
|---|---|---|---|---|
| Sodium polystyrene sulfate (SPS / Kayexalate) | Na+-K+ exchange resin in colon | Hours to days | 50 g PO in sorbitol, or rectal enema | Colonic necrosis (rare, black-box warning with sorbitol), hypernatremia |
| Patiromer | Exchanges Ca2+ for K+ in colon | ~7 hours | 8.4 g once daily PO | Constipation, hypomagnesemia; separate from other meds by 3 hrs |
| Sodium zirconium cyclosilicate (SZC) | Binds K+ throughout intestinal tract | ~1 hour | Per protocol | Edema, constipation; may raise gastric pH |
- Patiromer and SZC are approved for chronic management; not for acute monotherapy.
- SZC has the fastest onset among binders (~1 hr) and 9x higher K+-binding capacity than SPS per gram.
NON-EMERGENT TREATMENT
(Biochemical hyperkalemia, no ECG changes)
- Dietary counseling - restrict high-K+ foods; avoid salt substitutes (often contain KCl)
- Discontinue offending drugs - NSAIDs, ACE inhibitors/ARBs, potassium-sparing diuretics, heparin, TMP/SMX
- Optimize diuretic therapy - loop diuretics especially if eGFR <30 mL/min
- Oral NaHCO3 - if metabolic acidosis is contributing
- Consider chronic K+ binders - patiromer or SZC to allow continued use of RAAS inhibitors
Summary: The "C-BIG-K-Drop" Mnemonic
| Letter | Intervention |
|---|---|
| C | Calcium (membrane stabilization) |
| B | Bicarbonate (if acidotic) |
| I | Insulin + glucose (cell shift) |
| G | Get albuterol (cell shift) |
| K | Kayexalate/binders (remove K+) |
| D | Dialysis (remove K+ - last resort) |
Key reminder: Steps 1 and 2 are temporizing - they buy time. Only Step 3 (removal) achieves true correction. Always address the underlying cause.
- National Kidney Foundation Primer on Kidney Diseases, 8e, pp. 128-129
- Sabiston Textbook of Surgery, 11e, p. 602
This is a shared conversation. Sign in to Orris to start your own chat.