
photo-1784191031479.jpg
Risk factors for post op …
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Your notes capture the topic well. Here is a complete, textbook-level breakdown of Risk Factors for Post-operative Nausea and Vomiting (PONV):
Risk Factors for Post-operative Nausea & Vomiting (PONV)
PONV occurs in ~30% of the general surgical population and up to 70-80% in high-risk patients. Without any prophylaxis this is one of the most common reasons for prolonged PACU stay or unplanned admission.
The Apfel Simplified Risk Score (Adults)
The most widely used scoring tool. Each factor scores 1 point:
| Risk Factor | Points |
|---|---|
| Female sex | 1 |
| Non-smoker | 1 |
| History of PONV or motion sickness | 1 |
| Postoperative opioids expected | 1 |
| Total | 0 - 4 |
Predicted PONV risk by score:
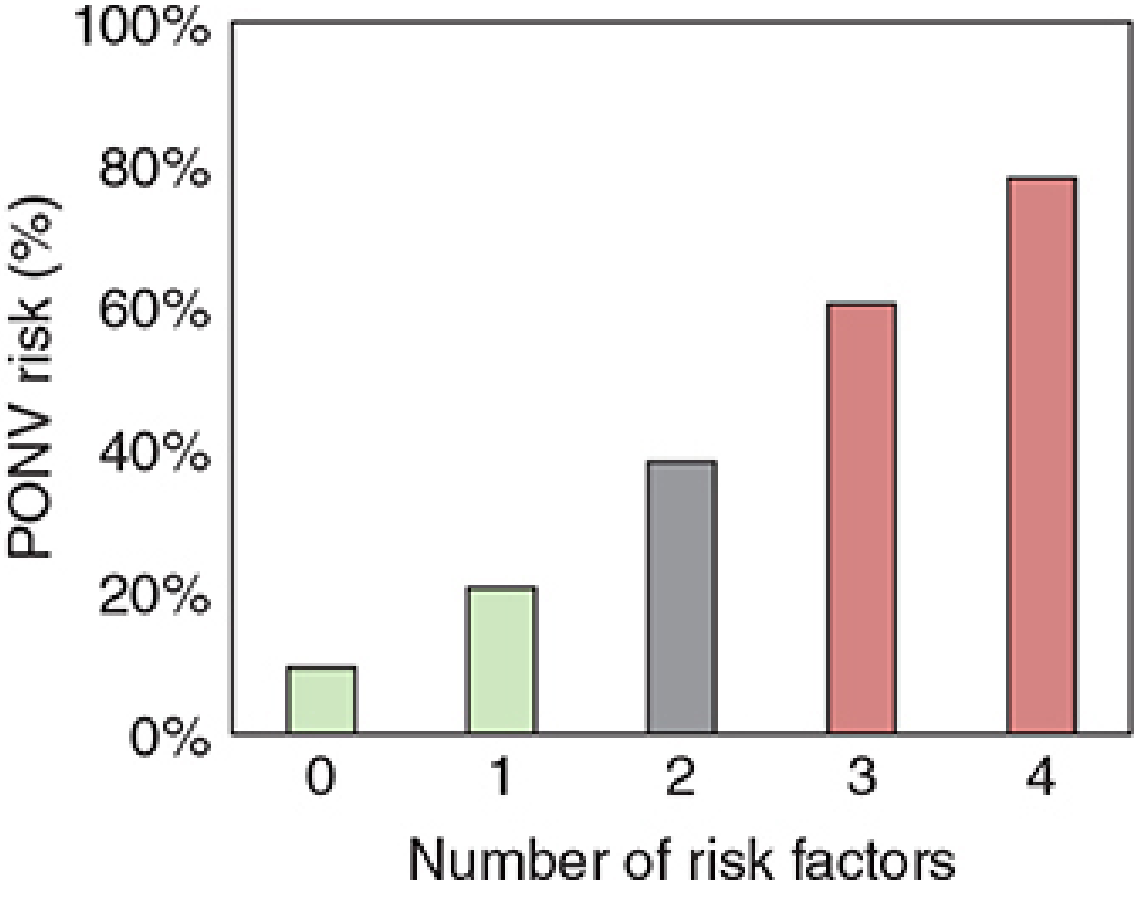
| Score | PONV Risk |
|---|---|
| 0 | ~10% |
| 1 | ~20% |
| 2 | ~40% |
| 3 | ~60% |
| 4 | ~80% |
Note: Obesity, anxiety, and neostigmine reversal are NOT independent risk factors for PONV per current evidence. - Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 516
Detailed Risk Factor Categories
A. Patient Factors (non-modifiable)
- Female sex - strongest independent predictor (evidence grade B1)
- Non-smoker - smoking is actually protective, likely through antiemetic effects of nicotine or altered 5-HT metabolism
- History of PONV or prior motion sickness - the single best predictor of future PONV
- Younger age - children and young adults are at higher risk
- Not BMI - obesity and anxiety are disproven as independent risk factors
B. Anaesthetic Factors (modifiable)
- General anaesthesia vs. regional anaesthesia - highest level evidence (A1); regional/neuraxial reduces PONV significantly
- Volatile (inhalational) agents - e.g., sevoflurane, isoflurane, desflurane (evidence A1)
- Nitrous oxide (N₂O) - independent emetogenic agent (evidence A1)
- Postoperative opioids - dose-dependent emetogenic effect (evidence A1)
- Longer duration of anaesthesia (evidence B1)
- Neostigmine for neuromuscular reversal - conflicting evidence; sugammadex preferred to reduce PONV risk
Propofol (TIVA) reduces PONV by ~20% but does not eliminate it entirely if opioids are still used. - Goldman-Cecil Medicine, p. 4221
C. Surgical Factors
- Gynaecological surgery (laparoscopic or open)
- ENT surgery (especially middle ear/strabismus)
- Ophthalmological surgery
- Laparoscopy (pneumoperitoneum elevates intra-abdominal pressure, stimulates vagal afferents)
- Cholecystectomy
- Longer surgery duration (>30 min) - especially in paediatric patients
Factors with Conflicting Evidence
- ASA physical status
- Menstrual cycle phase
- Anaesthetist experience level
- Muscle relaxant antagonists (neostigmine)
Disproven / Not Clinically Relevant
- BMI / obesity
- Anxiety
- Nasogastric tube use
- Supplemental oxygen
- Perioperative fasting duration
- Migraine history
Paediatric PONV (Eberhart Score)
Four independent predictors for children:
| Factor | Points |
|---|---|
| Surgery duration >30 min | 1 |
| Age >3 years | 1 |
| Strabismus surgery | 1 |
| History of POV in patient or family | 1 |
Risk: 0→9%, 1→10%, 2→30%, 3→55%, 4→70%
Prophylaxis Thresholds (SAMBA Guidelines)
- 1-2 risk factors: dual antiemetic therapy (e.g., ondansetron + dexamethasone)
- ≥3 risk factors: 3-4 agent therapy + consider TIVA (propofol-based)
- Agents: ondansetron (5-HT₃ antagonist), dexamethasone, droperidol (limited by FDA black box warning), aprepitant (NK-1 antagonist)
Your notes correctly identified the key Apfel factors: female sex, non-smoker, history of motion sickness, and added the anaesthetic/surgical context (GA with inhalational agents + opioids; surgeries like gynaec, ENT, ophthal, laparoscopy). These align perfectly with SAMBA consensus guidelines. - Barash Clinical Anesthesia, 9e, p. 1747; Morgan & Mikhail, 7e, p. 514-516
This is a shared conversation. Sign in to Orris to start your own chat.