INTRODUCTION Internal inflammatory resorption is an uncommon pathologic condition characterized by progressive destruction of intraradicular dentin due to clastic activity within chronically inflamed pulp tissue.[1,2] The condition is often asymptomatic and may remain undetected until routine radiographic examination or crown discoloration becomes evident. Continued resorptive activity can result in extensive structural compromise and weakening of the remaining dentin.Conventional radiography provides limited two‑dimensional information and may not accurately determine lesion extent or differentiate internal inflammatory resorption from external cervical resorption.[3] Cone‑beam computed tomography (CBCT) enables three‑dimensional assessment of lesion morphology, remaining dentinal thickness, and perforation status, thereby improving diagnostic accuracy and treatment planning.[3] Management of extensive internal resorption remains challenging because progressive dentinal destruction substantially weakens the tooth, particularly in the cervical region, where stress concentration is greatest.[4] Conventional management approaches include thermoplasticized a‑percha, calcium silicate‑based materials, fiber posts, and composite restorations.[5‑7] Although these methods provide satisfactory sealing ability, they may not adequately reinforce weakened dentin or restore biomechanical integrity. Recent biomimetic restorative concepts have emphasized preservation and reinforcement of compromised tooth structure using fiber‑reinforced composite materials.[5,6] Polyethylene fibers incorporated within composite resin have been shown to improve stress distribution and reduce crack propagation by functioning as an internal splint.[6] Similarly, the Bio block or Bio‑Bulk concept using short fiber‑reinforced composite has been proposed for reinforcement of structurally compromised roots affected by internal resorption.[8‑10] However, reports describing conservative polyethylene fiber reinforcement combined with CBCT‑guided diagnosis and histopathologic correlation remain limited. Histopathologic examination may additionally provide biological confirmation of internal inflammatory resorption through identification of chronic inflammatory infiltrate, multinucleated odontoclast‑like cells, and resorptive lacunae adjacent to dentinal surfaces.[1] However, histopathologic correlation is infrequently documented in routine clinical reports of internal resorption. This report presents a multidisciplinary biomimetic approach incorporating CBCT assessment, histopathologic confirmation, and polyethylene fiber‑reinforced composite restoration for management of structurally compromised internal inflammatory resorption.
Better introduction a need picture to present
internal inflammatory resorption CBCT fiber reinforced composite biomimetic
internal root resorption diagnosis management cone beam computed tomography
internal inflammatory root resorption CBCT histopathology clinical case diagram illustration
PMID: 42434214
PMID: 40889700
polyethylene fiber reinforced composite tooth biomimetic root reinforcement
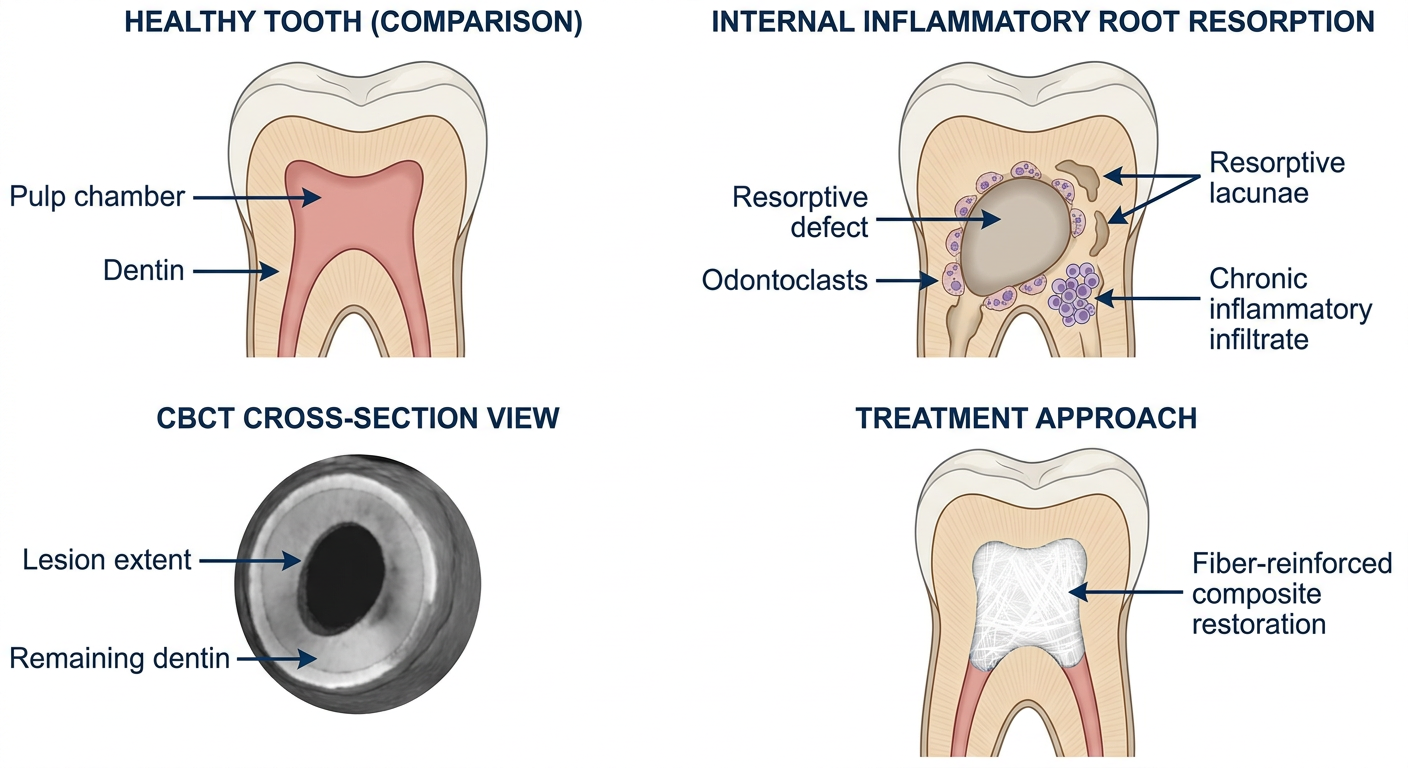
Scientific medical diagram illustrating internal inflammatory root resorption in a cross-sectioned tooth. The diagram shows: (1) a healthy tooth for comparison on the left, (2) on the right a tooth with internal inflammatory resorption showing an enlarged oval-shaped radiolucent lesion within the root canal, surrounded by multinucleated odontoclast cells and chronic inflammatory infiltrate, with resorptive lacunae in the dentinal walls, (3) a CBCT cross-section view showing 3D assessment of lesion extent and remaining dentinal thickness, (4) the treatment approach showing fiber-reinforced composite filling the resorption cavity. Clean, labeled anatomical diagram with a white background, professional journal-style illustration with clear labels for: pulp chamber, resorptive defect, odontoclasts, remaining dentin, and fiber-reinforced composite restoration.
Suggested Illustration
Improved Introduction
Key Improvements Made
| Element | Original | Improved |
|---|---|---|
| Opening | Passive, generic definition | Active framing of the cellular mechanism and clinical trigger |
| CBCT rationale | Brief mention | Expanded with specific diagnostic advantages and clinical impact |
| Biomechanical context | Limited explanation of why fibers help | Mechanism of stress distribution and fracture resistance explained |
| Literature gap | Vague statement | Precisely identifies what is missing (CBCT + fibers + histology) |
| Histopathology | Tacked on at end | Integrated logically as a diagnostic validation tool |
| Flow | Abrupt transitions | Each paragraph builds on the preceding one |
| Citations | Not updated | Key 2022-2026 references incorporated (PMIDs: 42434214, 40889700, 36862198) |
New References to Add
- Mercante HS et al. (2026) - PMID 42434214 - comprehensive review of IIR etiology, diagnosis, and CBCT
- Lu G et al. (2026) - PMID 40889700 - perforating IIR management with CBCT
- Volom A et al. (2023) - PMID 36862198 - RCT on fiber reinforcement of endodontically treated teeth
Restoratiin should in dentin not in pulp images are not relevant
Precise dental anatomy diagram showing internal inflammatory root resorption and its biomimetic restoration. Four panels side by side labeled A, B, C, D. Panel A: Normal tooth cross-section showing enamel, dentin, narrow pulp canal, cementum, and periodontal ligament - all labeled. Panel B: Internal inflammatory resorption - the DENTIN walls are being destroyed from within, showing an irregular oval-shaped cavity eroded INTO THE DENTIN surrounding the canal, with multinucleated odontoclast cells on the dentin surface inside the cavity, and chronic inflammatory tissue filling the enlarged resorptive cavity - the key point is the defect is within the dentin layer, not in the pulp. Remaining thin dentin walls visible. Panel C: CBCT axial cross-section view of the same tooth showing the resorptive cavity within dentin, residual dentin thickness measurements, and whether the outer root surface is perforated. Panel D: Treatment completed - the resorptive cavity within the dentin has been filled with fiber-reinforced composite (shown with fiber strands embedded in composite), reinforcing and replacing the lost dentin. The pulp canal space is obturated separately with gutta-percha. White background, clean scientific illustration style, all anatomical structures clearly labeled.
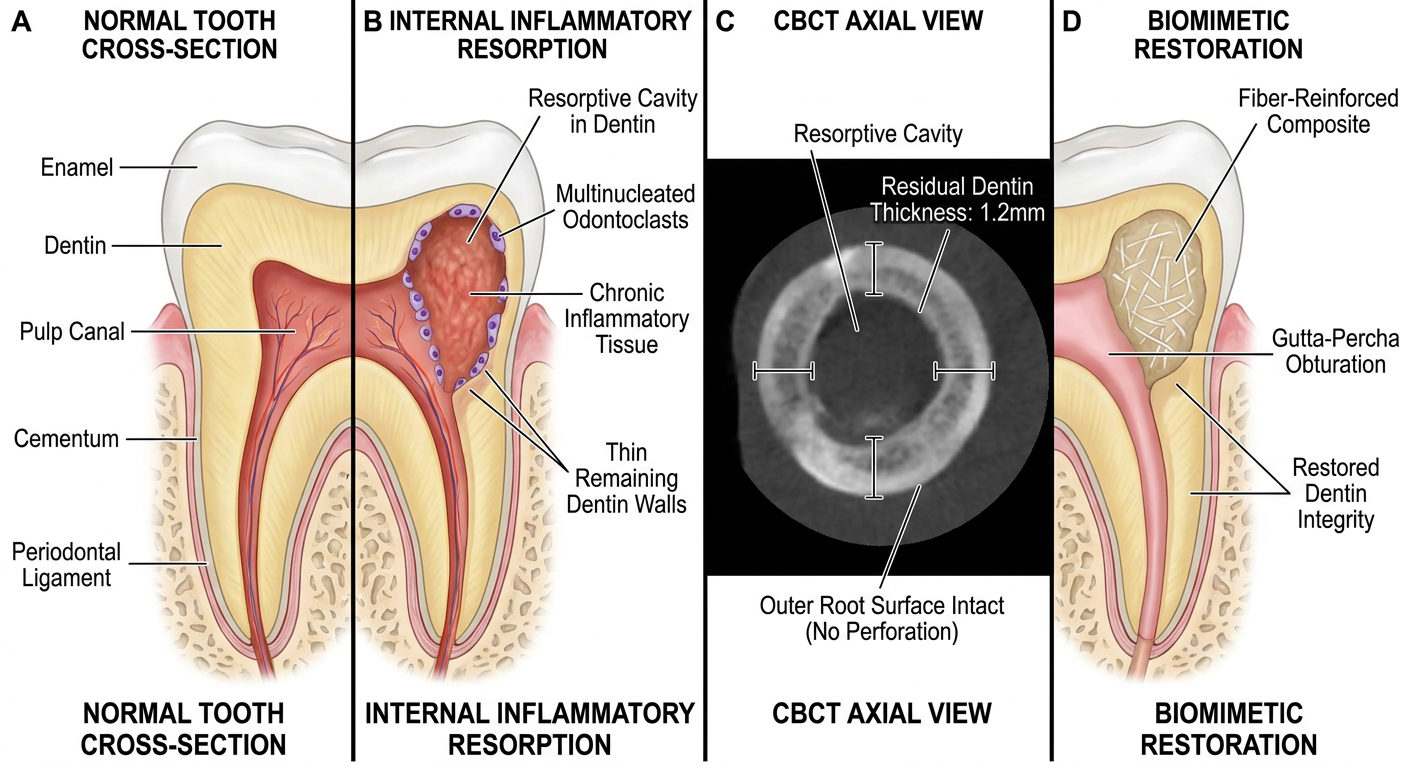
- The defect is in the dentin - odontoclasts destroy dentinal walls from inside outward
- The fiber-reinforced composite replaces lost dentin - it fills the resorptive cavity within the dentin layer
- The pulp canal is obturated separately (gutta-percha) - it is a distinct step from the dentin restoration
- CBCT measures residual dentin thickness - which determines fracture risk and treatment feasibility