Greater sac anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive content from four authoritative textbooks plus excellent diagrams. Here is the complete answer:
Greater Sac - Anatomy
Definition and Overview
The peritoneal cavity is divided into two main subdivisions: the greater sac and the omental bursa (lesser sac). The greater sac constitutes the vast majority of the peritoneal cavity. It begins superiorly at the diaphragm and extends inferiorly into the pelvic cavity. It is entered once the parietal peritoneum has been penetrated.
- Gray's Anatomy for Students, p. 363
The greater and lesser omentum divide the peritoneal cavity into the greater and lesser sacs. The lesser sac is contained behind the lesser and greater omentum, the stomach, and the transverse colon, and communicates with the greater sac through the foramen of Winslow (omental/epiploic foramen).
- Sabiston Textbook of Surgery, p. 1447
Sagittal View - Greater Sac and Relations
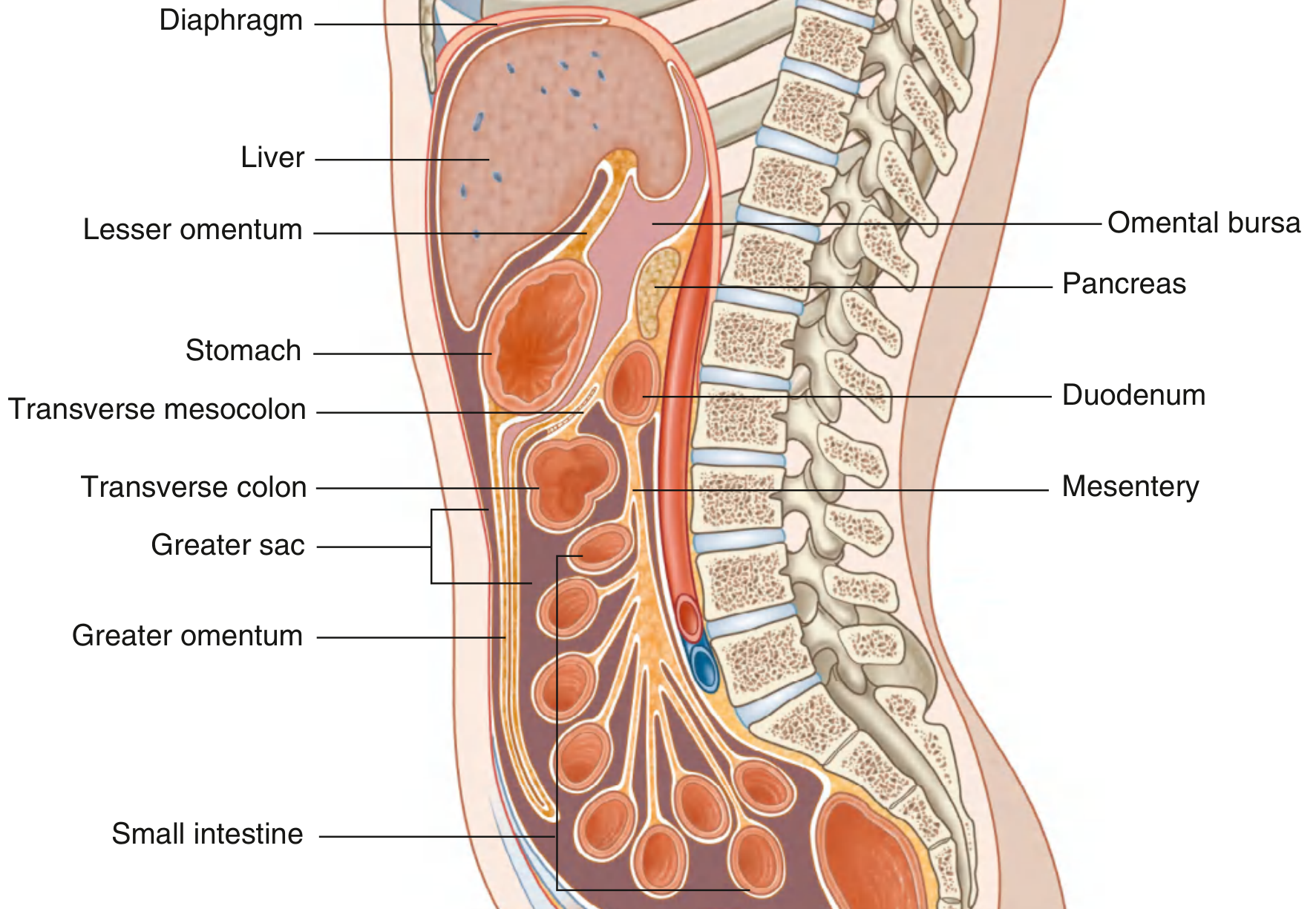
Fig. 4.54 - Greater and Lesser Sacs of the Peritoneal Cavity (Gray's Anatomy for Students)
Transverse Section - Omental Foramen and Boundaries
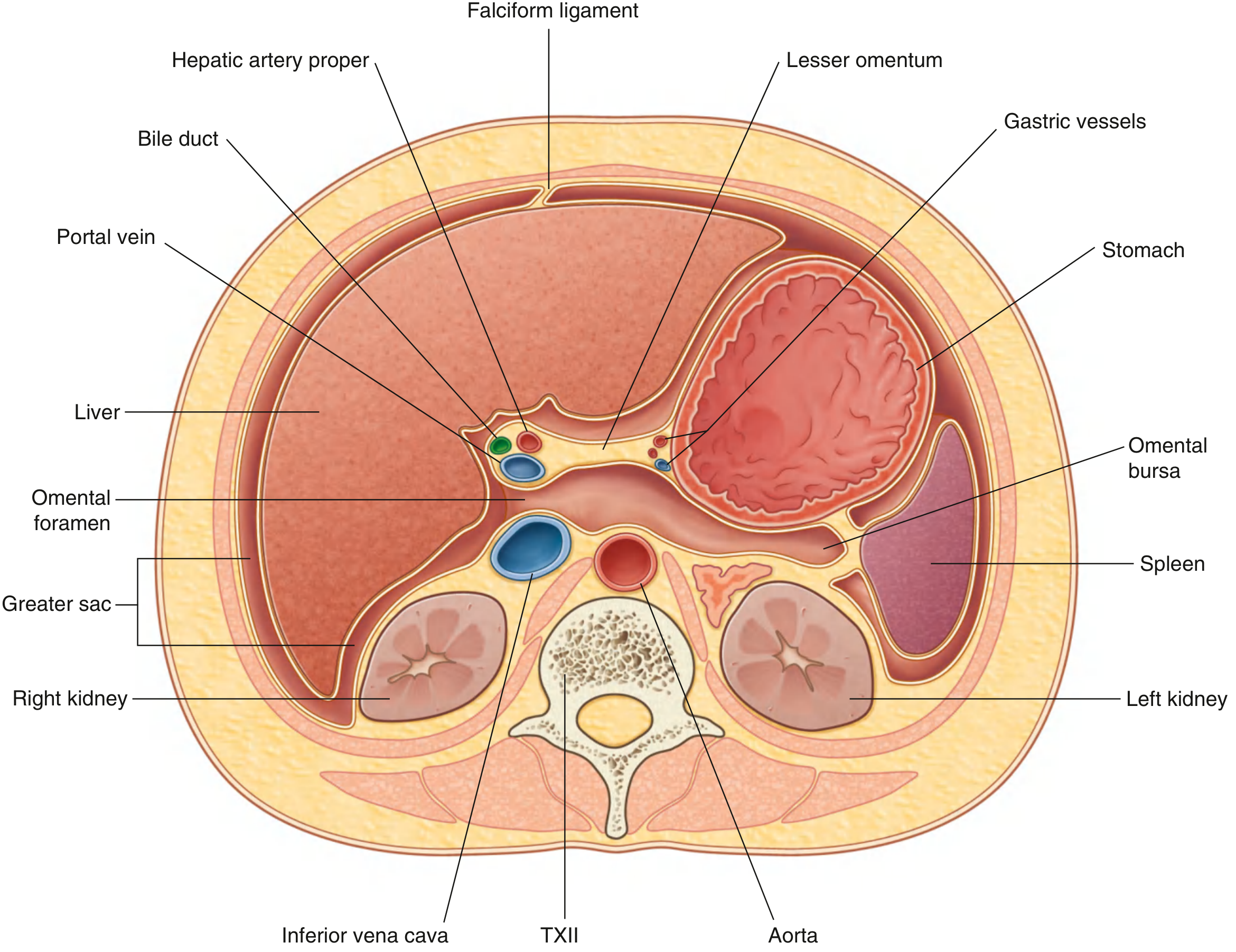
Fig. 4.55 - Transverse Section showing Continuity Between Greater and Lesser Sacs through the Omental (Epiploic) Foramen (Gray's Anatomy for Students)
Omental (Epiploic) Foramen - Boundaries
The omental foramen is the communication between the greater sac and the lesser sac. The structures bordering it (all covered with peritoneum) are:
| Relation | Structure |
|---|---|
| Anterior | Portal vein, hepatic artery proper, bile duct (in the free edge of the lesser omentum) |
| Posterior | Inferior vena cava |
| Superior | Caudate lobe of the liver |
| Inferior | First part of the duodenum |
- Gray's Anatomy for Students, p. 363
Compartments of the Greater Sac
The transverse colon and its mesentery divide the greater sac into a supramesocolic and an inframesocolic compartment.
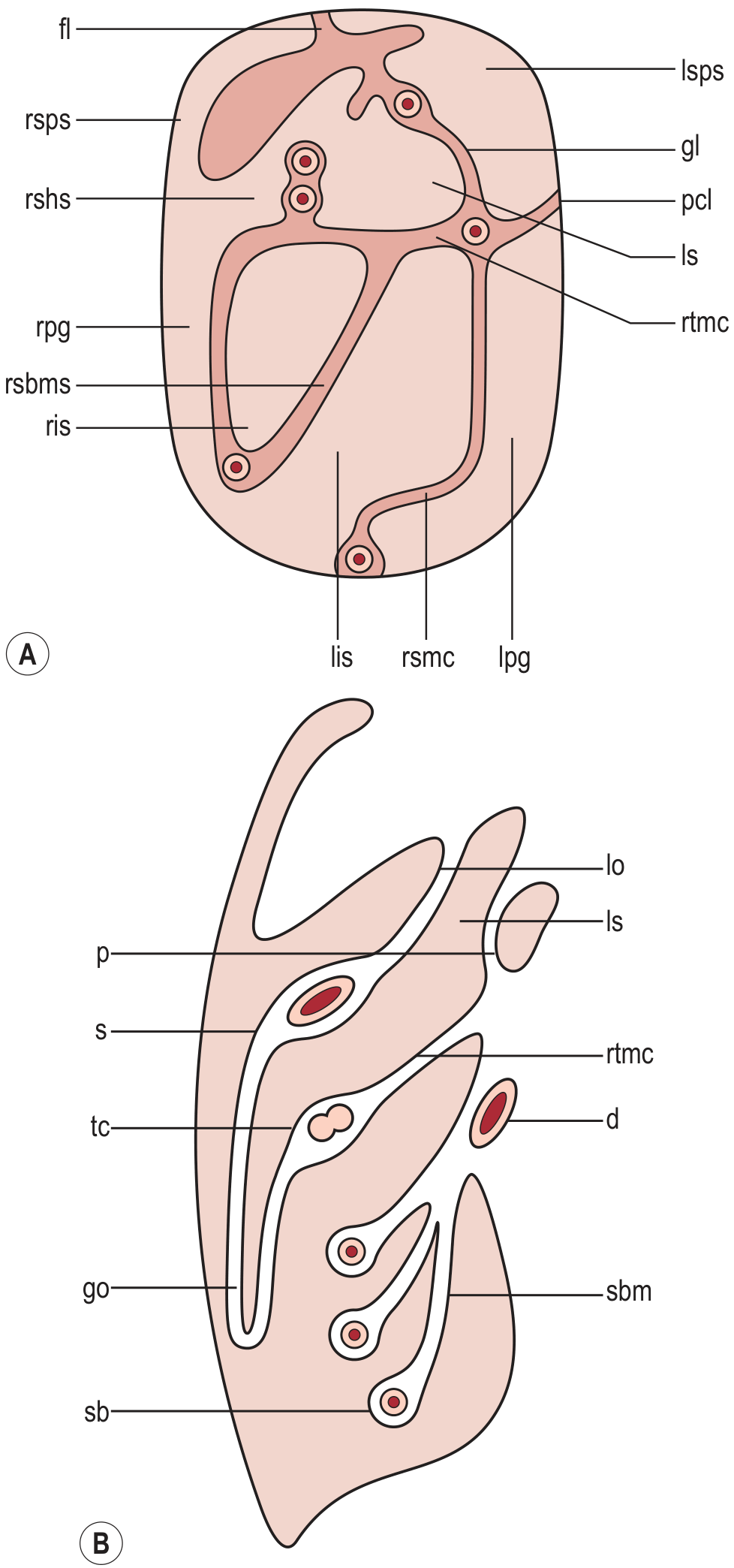
Fig. 21.47 - Division of Peritoneal Cavity (Grainger & Allison's Diagnostic Radiology)
1. Supramesocolic Compartment
(Diaphragm to transverse mesocolon)
Right supramesocolic space:
- Right subphrenic space - over the diaphragmatic surface of the right lobe of liver; limited on the left by the falciform ligament and posteromedially by the right coronary ligament
- Right subhepatic space (Morison's pouch / hepatorenal fossa) - between the liver and the right kidney; the most gravity-dependent space in the supine position; common site for fluid and abscess collection after biliary surgery
Left supramesocolic space (four intercommunicating compartments):
- Left anterior perihepatic space - bounded by falciform ligament (right), liver surface (posteriorly), and diaphragm (anteriorly); affected by left lobe liver or gastric lesions
- Left posterior perihepatic space (gastrohepatic recess) - posterior margin of the lateral segments of the left lobe; close to lesser curve of stomach and anterior duodenal wall
- Left anterior subphrenic space - between anterior stomach wall and left hemidiaphragm; fluid here suggests gastric or splenic flexure perforation
- Left posterior subphrenic / perisplenic space - posterior extension of the anterior subphrenic space
2. Inframesocolic Compartment
(Transverse mesocolon to pelvic rim)
- Right infracolic space - the smaller of the two; terminates at the ileocaecal junction; bounded laterally by the ascending colon
- Left infracolic space - larger; opens into the pelvis except where restricted by the sigmoid mesocolon; bounded laterally by the descending colon
- Right paracolic gutter - alongside the ascending colon; freely continuous with the right perihepatic space superiorly and with the pelvic cavity inferiorly (important route for spread of infection and malignancy)
- Left paracolic gutter - alongside the descending colon; cephalad continuation is partially restricted by the phrenicocolic ligament, limiting upward spread from the left side
3. Pelvic Peritoneal Cavity
-
Lateral paravesical spaces
-
Pouch of Douglas - rectouterine space (females) or rectovesical space (males); the most dependent portion of the entire peritoneal cavity in the erect posture
-
Grainger & Allison's Diagnostic Radiology, pp. 547-548
CT Peritoneogram - Greater Sac in Context
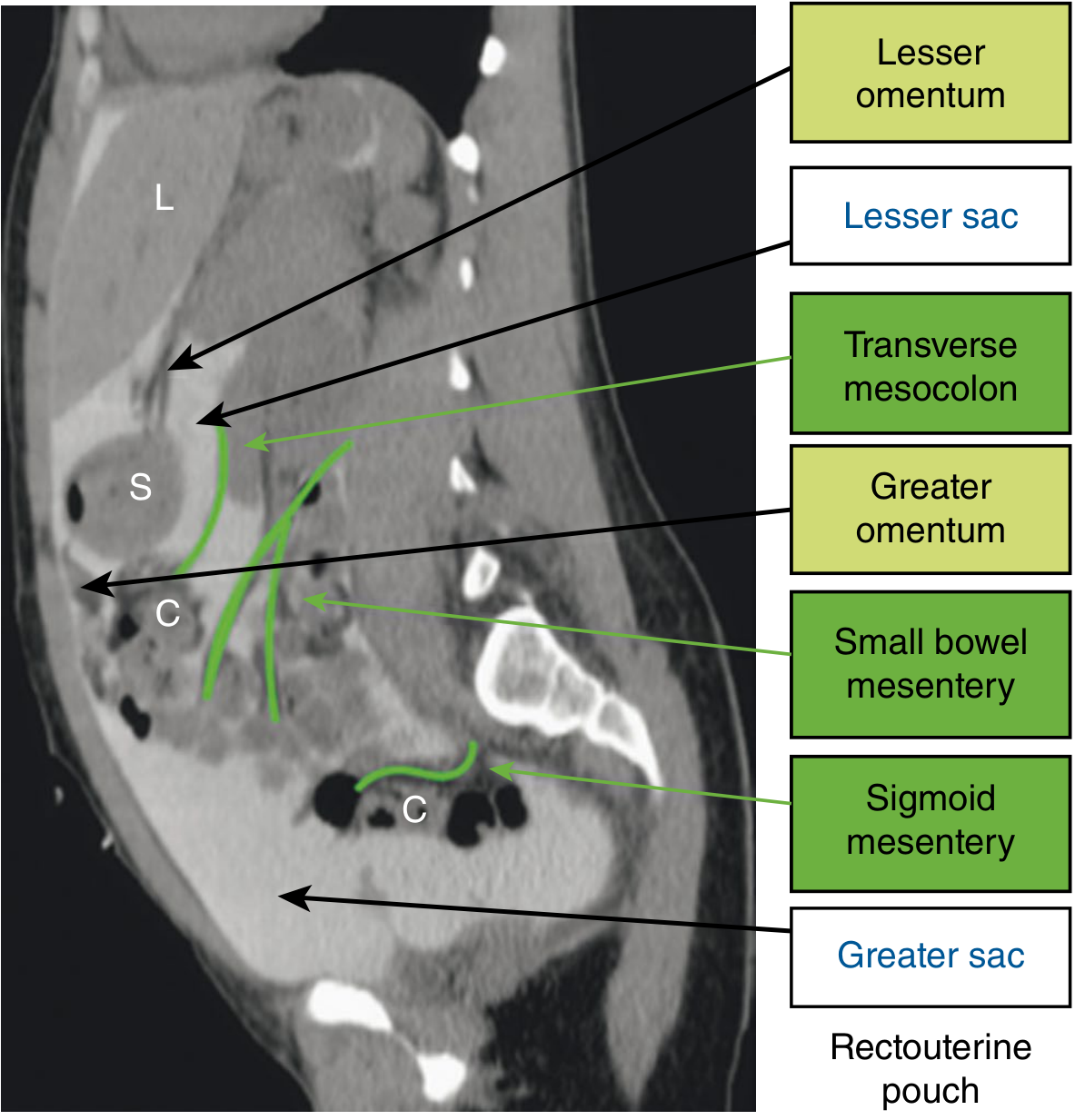
Fig. 70.1 - CT peritoneogram illustrating mesenteries, greater sac, lesser sac, and omenta (Sabiston Textbook of Surgery)
Peritoneal Fluid Circulation
Peritoneal fluid circulates in a clockwise direction within the greater sac. The common sites where fluid (ascites, blood, pus) pools and where peritoneal implants are found are:
- Rectovesical/rectouterine pouch (Pouch of Douglas) - most dependent in erect posture
- Right paracolic gutter - most dependent in supine posture, connects freely with subhepatic space
- Right subhepatic space (Morison's pouch)
- Right subphrenic space
- Left paracolic gutter (less free communication superiorly due to phrenicocolic ligament)
- Sabiston Textbook of Surgery, p. 1447; Yamada's Textbook of Gastroenterology
Histology of the Peritoneum
The peritoneum (lining both greater and lesser sac) consists of:
- Mesothelium - a single layer of simple cuboidal epithelium
- Underlying mesenchymal cells
Functions include: protection of viscera, facilitation of smooth visceral movement, immunologic roles, and tissue repair/scar formation. The peritoneal surface area is very large, which facilitates both disease spread and therapeutic delivery (e.g., peritoneal dialysis, HIPEC).
- Sabiston Textbook of Surgery, p. 1447
Clinical Relevance Summary
| Feature | Clinical Significance |
|---|---|
| Morison's pouch (hepatorenal fossa) | First site of free fluid accumulation on FAST ultrasound in trauma |
| Pouch of Douglas | Palpable on PR/PV exam when fluid, pus, or tumour is present |
| Right paracolic gutter | Pathway for spread of appendicitis/peritonitis to right subphrenic space |
| Phrenicocolic ligament | Limits spread up the left paracolic gutter (contrast with right side) |
| Omental foramen | Bordered by portal triad anteriorly and IVC posteriorly; Pringle manoeuvre compresses it |
| Greater omentum | Acts as a "policeman of the abdomen" - walls off infection and perforations |
This is a shared conversation. Sign in to Orris to start your own chat.