Gout
Reading File
Finding Sources
Searching PubMed
gout management hyperuricemia
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive response. Here is a full, well-structured overview of gout:
Gout
Definition & Epidemiology
Gout is a form of inflammatory arthritis caused by the deposition of monosodium urate (MSU) crystals in joints and periarticular tissues, driven by sustained hyperuricemia (plasma urate >6.8 mg/dL). It affects approximately 4% of U.S. adults - roughly 5% of males and 3% of females - and prevalence increases significantly with age. Risk factors include obesity, hypertension, diabetes, chronic kidney disease, and use of thiazide diuretics or cyclosporine.
- Rosen's Emergency Medicine, 10e
- Robbins & Kumar Basic Pathology
Pathogenesis
Uric Acid Metabolism
Uric acid is the end product of purine catabolism. Purines are produced via two pathways:
- De novo pathway: synthesis from non-purine precursors
- Salvage pathway: recycling of free purine bases from dietary intake or DNA/RNA degradation
Uric acid is filtered by the glomerulus, almost completely reabsorbed by the proximal tubule, with a small fraction secreted by the distal nephron. In primary gout (~90% of cases), reduced renal excretion is the main driver (mechanism usually unknown). In secondary gout, causes include:
- Overproduction: tumor lysis syndrome, HGPRT enzyme defects (partial deficiency = gout; complete absence = Lesch-Nyhan syndrome)
- Reduced excretion: chronic renal disease, diuretics, cyclosporine
Crystal-Induced Inflammation
When urate crystals precipitate in a joint, the sequence is:
- Resident synovial macrophages phagocytose MSU crystals
- Crystals activate the NLRP3 inflammasome
- Caspase-1 is activated, generating active IL-1β
- IL-1β recruits neutrophils, which release cytokines, free radicals, and proteases
- Crystals damage phagolysosomal membranes, causing lysosomal enzyme leakage
- Result: acute synovitis, self-limited but recurrent
Only ~10% of people with hyperuricemia ever develop gout. Contributing factors include age, duration of hyperuricemia, and precipitating events (dietary purine load, alcohol, dehydration, trauma, surgery).
- Robbins & Kumar Basic Pathology
Clinical Stages
| Stage | Features |
|---|---|
| Asymptomatic hyperuricemia | Elevated urate, no symptoms; may persist for 20-30 years |
| Acute gouty arthritis | Sudden, severe monoarthritis; peaks in 1-2 days; resolves in days to weeks |
| Intercritical period | Symptom-free intervals between attacks; attacks become more frequent over time |
| Chronic tophaceous gout | Persistent joint disease; tophi form; bony erosion; joint deformity |
Clinical Features
The classic presentation is podagra - acute, exquisitely painful arthritis of the first metatarsophalangeal (MTP) joint. Other commonly affected joints: knee, ankle, tarsal joints, wrists, and fingers.
Up to 20% of patients present with polyarticular involvement, or associated bursitis and tenosynovitis that can mimic cellulitis.
Tophi are gritty, chalk-like nodules of packed MSU crystals found in subcutaneous tissue, bursae, joint spaces, and soft tissues. They are generally painless but indicate chronic disease.

- Rosen's Emergency Medicine, 10e
Diagnosis
Definitive - Synovial Fluid Analysis
Joint aspiration (arthrocentesis) is the gold standard, especially for a first episode or when septic arthritis cannot be excluded. Under polarized light microscopy, MSU crystals appear needle-shaped and negatively birefringent (yellow when parallel to the polarizer axis).
Laboratory
- Serum uric acid: often elevated, but not reliable during an acute attack (may be normal). Does not correlate well with flare frequency.
- WBC: may be elevated (nonspecific)
- Renal function: important because many treatments are nephrotoxic and there is an association between gout and renal insufficiency
Imaging
- Plain X-ray: acute attacks show only soft-tissue swelling; chronic disease shows asymmetric, sclerotic-appearing punched-out bony erosions outside the joint capsule ("overhanging edge" sign)
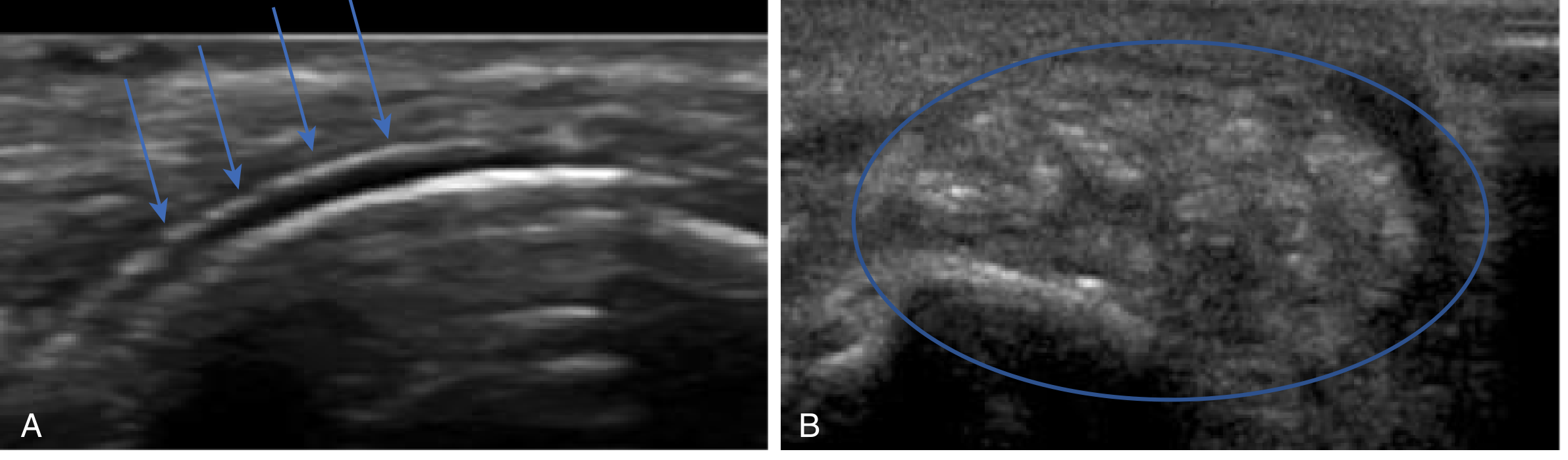
- Ultrasound: highly useful; shows the double contour sign (urate deposition on articular cartilage surface) and tophi with a characteristic "lump of sugar" appearance
- Rosen's Emergency Medicine, 10e
Management
Acute Attack
The goal is rapid anti-inflammatory treatment. Do not initiate urate-lowering therapy during an acute attack, but do continue it if already prescribed (stopping can prolong the flare).
| Agent | Notes |
|---|---|
| NSAIDs (first-line) | Indomethacin, naproxen, ibuprofen. Start promptly; continue 24h after resolution. Avoid in PUD, GI bleeding, renal insufficiency. |
| Colchicine | Inhibits microtubule formation, blocking crystal-induced inflammation. Effective, but narrow therapeutic window; contraindicated in renal/hepatic insufficiency; GI side effects common. |
| Corticosteroids | Prednisone 40 mg/day x 5-7 days, or intra-articular injection (most effective for monoarticular disease; do not use if septic arthritis possible). Avoid concurrent oral steroids + NSAIDs (GI risk). |
| Combination therapy | Intra-articular steroid + colchicine or NSAID reasonable for severe/polyarticular disease. |
Non-pharmacologic: ice, elevation, oral hydration, avoidance of triggers.
- Rosen's Emergency Medicine, 10e
Long-Term / Urate-Lowering Therapy (ULT)
Target serum urate: <6 mg/dL in symptomatic patients (some guidelines target <5 mg/dL for tophaceous disease).
| Drug | Class | Key Points |
|---|---|---|
| Allopurinol | Xanthine oxidase inhibitor (purine analog) | First-line. Start 100 mg/day; titrate up by 50 mg every 4 weeks. Dose-adjust for renal impairment. Avoid or reduce azathioprine dose if co-prescribed. |
| Febuxostat | Xanthine oxidase inhibitor (non-purine analog) | Use in allopurinol-intolerant patients. 40 or 80 mg/day; no dose adjustment for renal impairment. Caution: a large RCT showed higher all-cause and CV mortality vs. allopurinol in high-CV-risk patients. |
| Probenecid | Uricosuric agent | Increases renal urate excretion. Avoid in uric acid overproducers and nephrolithiasis. |
| Pegloticase | Recombinant pegylated uricase | Converts uric acid to allantoin (more soluble). For refractory/tophaceous gout. FDA-approved 2010. Risk of infusion reactions and loss of efficacy due to anti-drug antibodies. |
ULT should not be started during an acute flare. When initiating, co-prescribe low-dose colchicine or NSAIDs for 3-6 months as prophylaxis against flare precipitation.
- Comprehensive Clinical Nephrology, 7e
Lifestyle Modifications
- Reduce purine-rich foods: red meat, organ meats, shellfish, anchovies, beer
- Avoid fructose-sweetened beverages
- Increase hydration
- Reduce alcohol (especially beer)
- Weight loss in obese patients
- Review and discontinue precipitating medications (thiazides, low-dose aspirin) when feasible
Differential Diagnosis
- Septic arthritis: fever + joint swelling; must be excluded by arthrocentesis (joint fluid Gram stain/culture); never treat empirically as gout without ruling this out
- Pseudogout (CPPD): calcium pyrophosphate crystals; positively birefringent (blue when parallel); chondrocalcinosis on X-ray; associated with hyperparathyroidism, hemochromatosis, hypothyroidism
- Reactive arthritis: follows GI/GU infection; asymmetric oligoarthritis
- Rheumatoid arthritis: symmetric, small-joint, chronic; RF/anti-CCP positive
Special Situations
Transplant patients: Cyclosporine significantly reduces renal urate excretion. NSAIDs should be avoided. Allopurinol and febuxostat interact dangerously with azathioprine (reduce AZA dose by ~25% and monitor CBC closely, or switch to mycophenolate). Pegloticase may be an option for refractory cases. - Comprehensive Clinical Nephrology, 7e
Renal impairment: Allopurinol start at lower doses (100 mg/day); titrate cautiously due to oxypurinol accumulation. Febuxostat does not require dose adjustment.
Lesch-Nyhan syndrome: Complete HGPRT deficiency - causes severe hyperuricemia plus neurologic manifestations (self-mutilation, cognitive impairment, choreoathetosis). Classified as secondary gout. - Robbins & Kumar Basic Pathology
Recent Evidence (2024-2026)
A recent systematic review (PMID 39794008) found that SGLT2 inhibitors reduce hyperuricemic events, providing an additional benefit in diabetic patients with gout or at risk. An additional meta-analysis (PMID 39961457) confirmed a significant association between psoriasis/psoriatic arthritis and hyperuricemia/gout, suggesting shared inflammatory pathways and the need for uric acid monitoring in psoriatic patients.
This is a shared conversation. Sign in to Orris to start your own chat.