
Screenshot_20260620-074406.png
Explain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I have enough rich content. Here is the full explanation of PA 30.2 - Carcinoma of the Breast.
Carcinoma of the Breast (PA 30.2)
This covers all the required learning objectives: epidemiology, pathogenesis, classification, morphologic and microscopic features, prognostic factors, hormonal dependency, staging, and spread.
1. Epidemiology
- Breast cancer is the most common malignancy globally, surpassing lung cancer in 2020 with ~2.3 million new cases, accounting for nearly 12% of all new cancer diagnoses worldwide.
- In the United States, lifetime risk is 1 in 8 females (living to age 90).
- Approximately 75% of breast cancers are diagnosed after age 50.
- The disease is rare under age 25, and incidence rises steeply after age 30.
- Geographic variation: Highest incidence in North America, Northern/Western Europe, and Australia/New Zealand. Incidence is rising in low-resource countries due to lifestyle changes (delayed childbearing, fewer pregnancies, reduced breastfeeding).
- Ethnicity matters: Females of European descent have the highest overall incidence (average diagnosis age 63); females of African descent tend to be diagnosed younger (average 59) and have higher proportions of aggressive subtypes.
Key risk factors:
| Category | Factors |
|---|---|
| Hormonal | Early menarche, late menopause, nulliparity, late first pregnancy, hormone replacement therapy (HRT), oral contraceptives |
| Genetic (12% of cases) | BRCA1, BRCA2 mutations (account for 50% of familial cases); also PTEN, TP53, CDH1, PALB2 |
| Other | Increasing age, prior breast biopsy with atypical hyperplasia, radiation exposure, obesity (postmenopausal), alcohol |
2. Pathogenesis
Familial Breast Cancer
- BRCA1 (chromosome 17q): Tumor suppressor involved in DNA repair by homologous recombination. Loss leads to genomic instability. BRCA1-mutated cancers are frequently high-grade, ER-negative, and "basal-like" (triple negative).
- BRCA2 (chromosome 13q): Also a DNA repair gene. Mutations increase risk of both female and male breast cancer. BRCA2-mutated tumors more often ER-positive.
- Other genes: PTEN (Cowden syndrome), TP53 (Li-Fraumeni syndrome), CDH1 (lobular carcinoma + gastric signet ring carcinoma), PALB2.
Sporadic (Nonfamilial) Breast Cancer
- Driven by somatic mutations accumulating in breast ductal/lobular epithelium.
- Most luminal (ER-positive) cancers have mutations in PIK3CA and CDH1 and amplification of cyclin D1.
- HER2-positive cancers: amplification of the HER2 gene (chromosome 17q), leading to overexpression of HER2 receptor tyrosine kinase, which drives cell proliferation.
- Triple-negative breast cancer (TNBC): Characterized by TP53 mutations, BRCA1 epigenetic silencing, massive genomic instability, high tumor neoantigen burden, and pronounced immune infiltrates - making them more immunogenic and responsive to immunotherapy.
3. Classification
Classification is done at three levels:
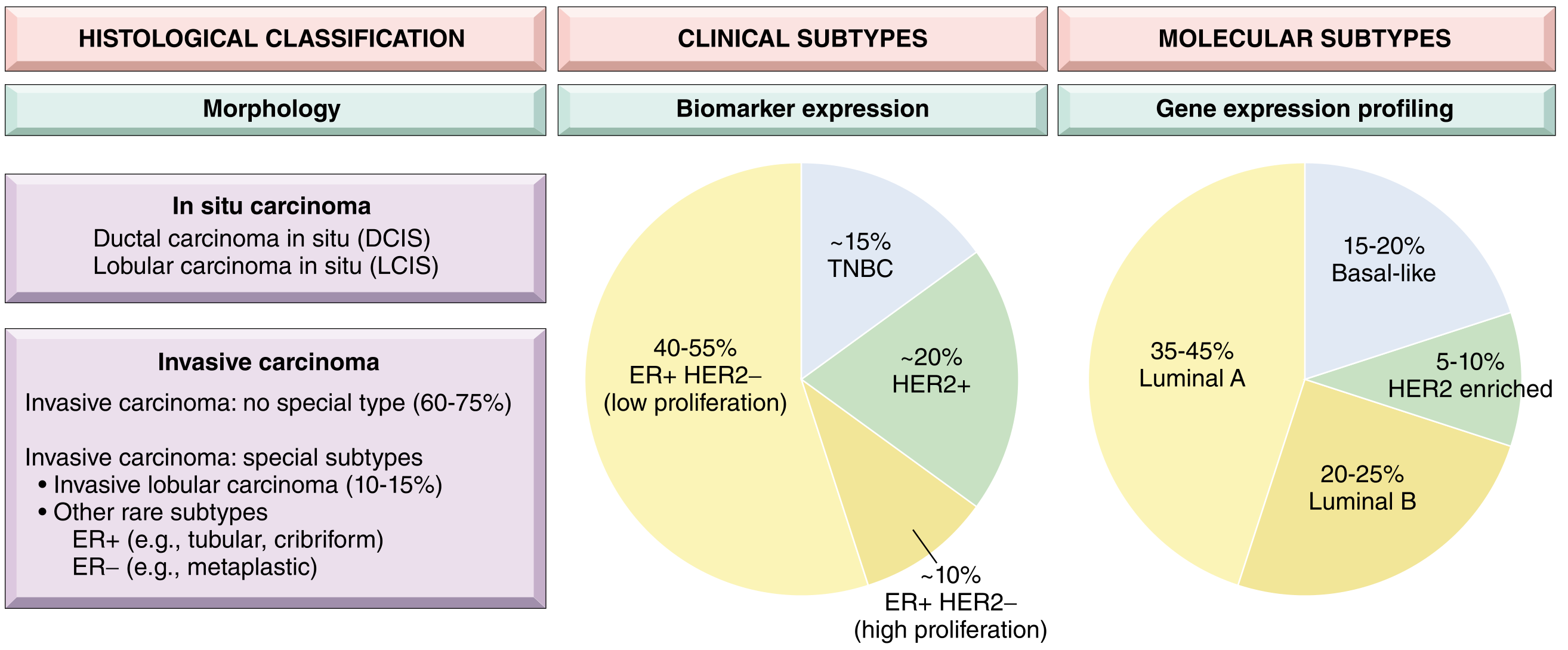
A. Morphological (Histological) Classification
In situ carcinoma:
- DCIS (Ductal carcinoma in situ): Precursor to invasive ductal carcinoma. Most often detected by mammography as calcifications. If untreated, progresses to invasive ductal carcinoma in the same breast.
- LCIS (Lobular carcinoma in situ): Marker of increased risk and precursor lesion. Risk of subsequent invasive carcinoma is bilateral (2/3 ipsilateral, 1/3 contralateral). Cells lack E-cadherin expression (same as invasive lobular carcinoma).
Invasive carcinoma:
- No special type (NST) - formerly "invasive ductal carcinoma NOS": ~75% of all invasive breast cancers.
- Special histologic types - see Section 4 below.
B. Clinical (Biomarker) Classification
| Subtype | Biomarkers | Frequency |
|---|---|---|
| Luminal (ER+/HER2-) | ER-positive, PR-positive, HER2-negative | ~50-65% |
| HER2+ | HER2 amplified/overexpressed | ~20% |
| TNBC | ER-, PR-, HER2- | ~15% |
C. Molecular (Intrinsic) Subtypes
Based on gene expression profiling:
- Luminal A: ER+/HER2-, low proliferation - best prognosis
- Luminal B: ER+/HER2-, higher proliferation - intermediate prognosis
- HER2 enriched: HER2 amplified - aggressive
- Basal-like: Mostly TNBC, high grade - poor prognosis
- Normal-like and Claudin-low: Rarer subtypes
4. Morphologic and Microscopic Features
Gross Morphology
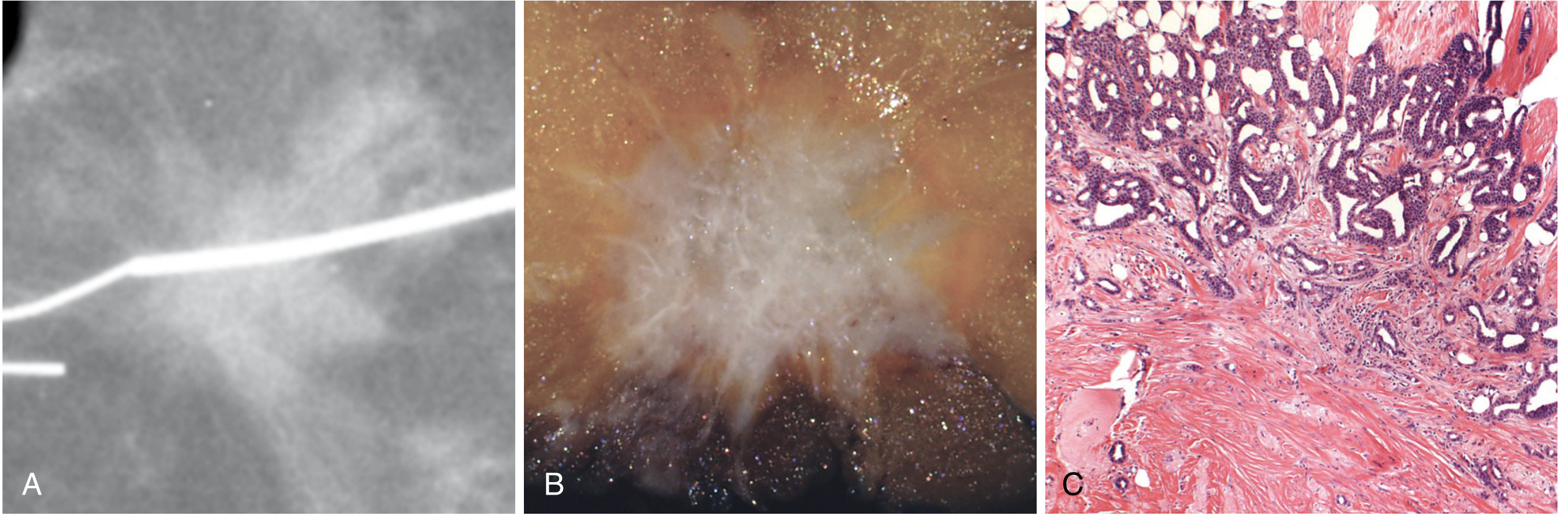
- Most common presentation: hard, irregular mass with spiculated margins (star-like) on mammography.
- Cut surface: gritty, chalky-white due to desmoplastic stroma and foci of calcification.
- Less common: well-circumscribed soft mass (seen in high-grade tumors with lymphocyte infiltrate, "medullary pattern").
Histologic Grading (Nottingham Score)
All invasive carcinomas are graded on 3 parameters (each scored 1-3):
- Tubule/gland formation (how much of the tumor forms glandular structures)
- Nuclear pleomorphism (size and shape variability of nuclei)
- Mitotic rate
| Grade | Score | Description |
|---|---|---|
| Grade 1 (well differentiated) | 3-5 | Tubular/cribriform pattern; small uniform nuclei; rare mitoses |
| Grade 2 (moderately differentiated) | 6-7 | Mixed tubules and solid nests; moderate pleomorphism |
| Grade 3 (poorly differentiated) | 8-9 | Ragged sheets; large irregular nuclei; frequent mitoses; necrosis |
Special Histologic Subtypes
| Type | Key microscopic feature | Biomarker | Prognosis |
|---|---|---|---|
| Invasive lobular carcinoma (10-15%) | Dyscohesive cells in single-file "Indian file" linear cords; signet ring cells; minimal desmoplasia | ER+, E-cadherin negative | Intermediate |
| Mucinous (colloid) | Tumor cell clusters floating in large lakes of mucin; soft, gelatinous gross appearance | ER+ | Favorable |
| Tubular | Exclusively well-formed tubules; may mimic benign sclerosing lesion | ER+ | Very favorable |
| Cribriform | Invasive nests with cribriform architecture | ER+ | Favorable |
| Papillary | True papillary fronds lined by tumor cells | ER+ | Favorable |
| Apocrine | Cells resembling sweat gland cells; enlarged round nuclei, prominent nucleoli, eosinophilic granular cytoplasm | Often HER2+ | Variable |
| Invasive micropapillary | Hollow balls of cells floating in intercellular fluid (mimic papillae but no fibrovascular core) | Often HER2+ | Poor |
| Metaplastic | Squamous or mesenchymal (spindle, chondroid, osseous) differentiation | TNBC | Poor |
| Inflammatory carcinoma | Diffuse dermal lymphovascular plugging by tumor cells; peau d'orange; NOT a histologic type | Usually high-grade | Very poor |
5. Hormonal Dependency
Breast cancer has a well-established hormonal dependence, particularly for ER-positive (luminal) tumors, which account for 50-65% of all cases.
- Estrogen drives proliferation of luminal cells. ER-positive tumor cells respond to estrogen signaling by upregulating genes involved in cell division.
- Endogenous estrogen excess (from obesity, HRT, early menarche/late menopause) increases risk.
- Anti-estrogen therapies are effective cytostatic treatments for ER-positive cancers:
- Tamoxifen - competitive ER blocker (used in pre- and post-menopausal women)
- Aromatase inhibitors (letrozole, anastrozole) - block peripheral estrogen synthesis (used in post-menopausal women)
- Fulvestrant - ER degrader
- CDK4/6 inhibitors (palbociclib, ribociclib, abemaciclib) - used in combination with endocrine therapy for advanced ER+ disease
- Progesterone receptor (PR) status is assessed alongside ER - PR positivity generally indicates a functioning ER signaling pathway and correlates with better response to endocrine therapy.
- HER2 (human epidermal growth factor receptor 2) is technically not a hormone receptor but represents a growth factor signaling axis. HER2 overexpression (due to gene amplification on chromosome 17q) drives proliferation, and is treated with targeted agents (trastuzumab, pertuzumab, lapatinib, trastuzumab-deruxtecan).
6. Staging and Spread
Staging (AJCC TNM System)
The breast cancer staging system integrates anatomic factors (TNM) with biologic factors (grade, ER, PR, HER2 status):
| Component | Description |
|---|---|
| T (Tumor size) | T1: ≤2 cm; T2: 2-5 cm; T3: >5 cm; T4: involves chest wall/skin |
| N (Node status) | N0: No nodal involvement; N1: movable ipsilateral axillary nodes; N2: fixed axillary nodes or internal mammary nodes; N3: infraclavicular, supraclavicular, or both |
| M (Metastasis) | M0: no distant metastasis; M1: distant metastasis |
Note: Anatomic stage alone is used only when ER, PR, HER2, and grade are unavailable - because biologic subtype dramatically affects prognosis and survival.
Routes of Spread
Local spread:
- Direct invasion into adjacent breast parenchyma, skin, nipple, and chest wall.
- Cooper ligament involvement leads to skin dimpling.
- Nipple involvement causes nipple retraction.
- Skin lymphatic infiltration causes peau d'orange (orange-peel appearance) - classic of inflammatory carcinoma.
Lymphatic spread (most common):
- Axillary lymph nodes (most frequent) - involved in ~50% of cases at diagnosis.
- Internal mammary nodes.
- Supraclavicular and infraclavicular nodes.
- Axillary node status is the single most important prognostic factor for early-stage disease.
Hematogenous spread (distant metastasis):
Most common sites:
- Bone (most common - especially spine, pelvis, ribs; causes pathological fractures and hypercalcemia)
- Lung
- Liver
- Brain
- Adrenal glands
Special metastatic patterns by subtype:
- Invasive lobular carcinoma has unique tendency to metastasize to peritoneum, retroperitoneum, leptomeninges (carcinomatous meningitis), GI tract, ovaries, and uterus.
- TNBC and HER2+ cancers metastasize earlier and more aggressively than luminal cancers.
7. Prognostic Factors
| Factor | Favorable | Unfavorable |
|---|---|---|
| Lymph node status | Node negative | Node positive (increasing N) |
| Tumor size | ≤1 cm | >5 cm |
| Histologic grade | Grade 1 | Grade 3 |
| Biomarker subtype | Luminal A (ER+, low grade) | TNBC or HER2+ |
| Molecular subtype | Luminal A | Basal-like, claudin-low |
| ER/PR status | Positive | Negative |
| HER2 | HER2- (without targeted therapy) | HER2+ (without targeted therapy) |
| Ki-67 index | Low proliferation | High proliferation |
| Age | Older (postmenopausal) | Younger (<35 years) |
| BRCA mutations | - | Associated with high-grade aggressive disease |
| Inflammatory carcinoma | - | Very poor prognosis |
| Margin status | Clear margins | Positive margins |
Gene expression assays (e.g., Oncotype DX, MammaPrint) provide additional prognostic and predictive information particularly for ER+/HER2-negative tumors, guiding decisions about chemotherapy.
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (Chapter 23); Robbins & Kumar Basic Pathology; Bailey and Love's Short Practice of Surgery 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.