Adrenal gland in surgery
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive material from multiple authoritative surgical textbooks. Let me compile the full response.
The Adrenal Gland in Surgery
Anatomy and Embryology
The adrenal glands are paired, orange/yellow structures positioned superior and slightly medial to the kidneys in the retroperitoneum. Each gland has two embryologically distinct components: the cortex (from coelomic mesothelium) and the medulla (from neural crest cells). This dual origin explains why tumors can arise at extraadrenal sites - particularly pheochromocytomas/paragangliomas, which can occur anywhere along the sympathetic chain.
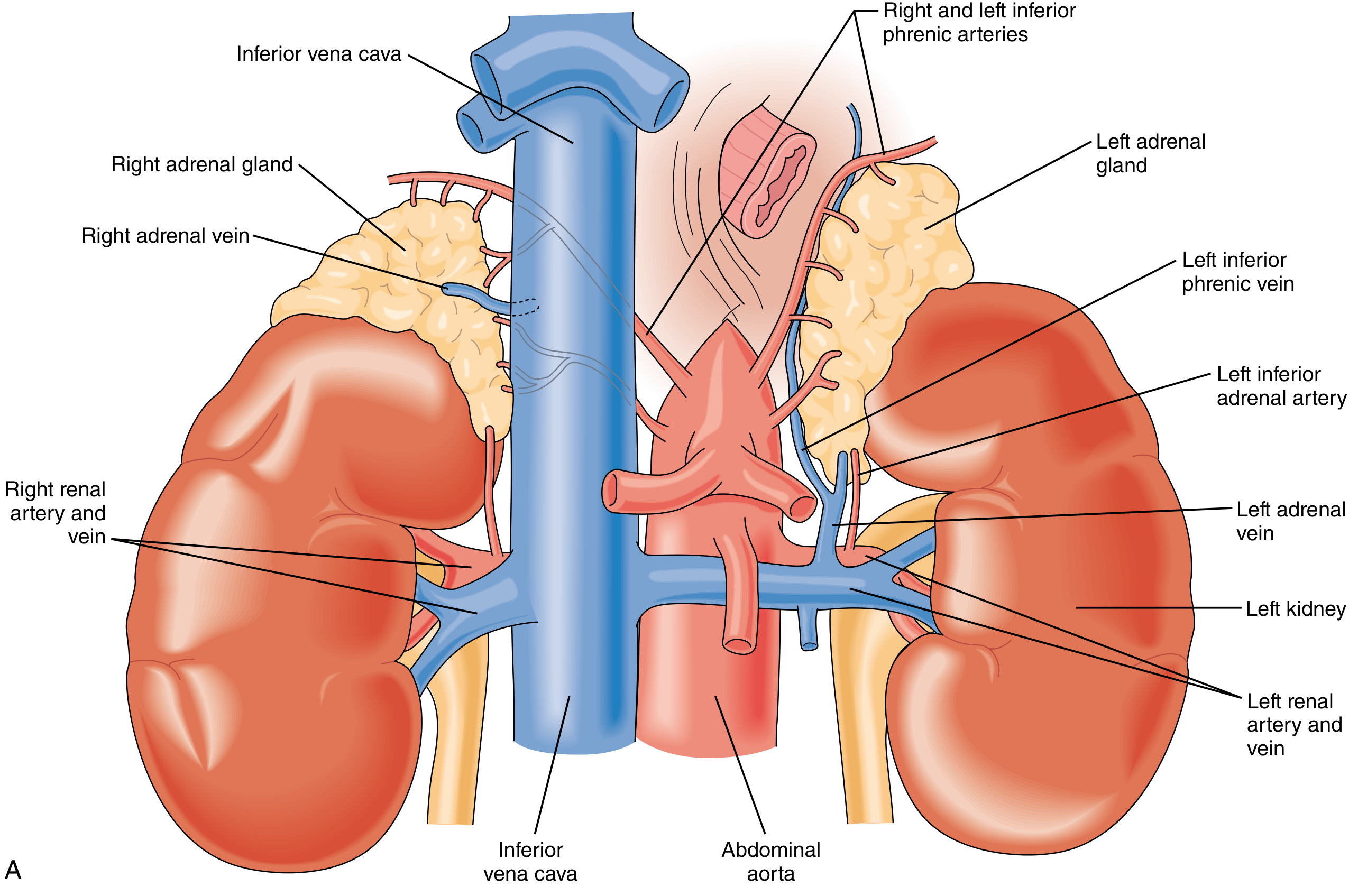
Relationships (surgically important):
- Right adrenal: abuts the posterolateral surface of the retrohepatic IVC; bounded by the right kidney inferolaterally, diaphragm posteriorly, and bare area of the liver anterosuperiorly
- Left adrenal: lies between the left kidney and aorta; its inferior limb extends toward the renal hilum; posterior to the diaphragm, anterior to the tail of pancreas and splenic hilum
Vascular anatomy (critical for surgery):
-
Arterial supply is diffuse (three sources): superior adrenal arteries from inferior phrenic arteries; middle adrenal arteries from the juxtaceliac aorta; inferior adrenal arteries from the renal arteries
-
Venous drainage is solitary: the left adrenal vein (~2 cm long) drains into the left renal vein after joining the inferior phrenic vein; the right adrenal vein is very short (~0.5 cm) and drains directly into the IVC - a critical surgical challenge
-
In ~20% of individuals the right adrenal vein may drain into an accessory right hepatic vein near the IVC confluence
-
Sabiston Textbook of Surgery, p. 1555-1556
Surgical Conditions of the Adrenal Gland
1. Adrenal Incidentaloma
Defined as an adrenal mass discovered on imaging done for another indication. Found in 1-8% of adults; incidence increases with age.
Two-step evaluation:
- Risk of malignancy (imaging characteristics, size)
- Hormonal activity (biochemical workup)
Size thresholds:
| Size | Risk of ACC | Management |
|---|---|---|
| <4 cm | ~2% | Surveillance if benign-appearing, non-functional |
| 4-6 cm | ~6% | Controversial - adrenalectomy or surveillance |
| >6 cm | ~25% | Adrenalectomy in most cases |
Biochemical screening for functionality:
| Syndrome | Screening Test | Positive Threshold |
|---|---|---|
| Cushing's syndrome | 1-mg overnight DST | AM cortisol ≥1.8 μg/dL |
| Pheochromocytoma | Plasma free metanephrines/normetanephrines | ≥2-4× ULN |
| Primary hyperaldosteronism | Aldosterone-to-renin ratio (ARR) | ARR >20 |
Surgery is indicated for: functional tumors, adrenocortical carcinoma (no distant mets), and indeterminate/large/symptomatic tumors.
- Current Surgical Therapy 14e, p. 855
2. Cushing's Syndrome (Hypercortisolism)
Cortisol excess from a zona fasciculata adenoma. Features include central obesity, "buffalo hump," "moon face," hypertension, DM, easy bruising, abdominal striae, proximal muscle weakness, hirsutism. Adrenalectomy is indicated for adrenal-source hypercortisolism (suppressed ACTH + elevated cortisol).
3. Primary Hyperaldosteronism (Conn's Syndrome)
From zona glomerulosa. Presents with hypertension (often refractory), hypokalemia (in ~9-37%), muscle weakness, polyuria.
- Screening: ARR >20
- Confirmation: saline suppression test or 24-hr urine aldosterone on high-sodium diet
- Adrenal venous sampling (AVS) is required in surgical candidates >35 years to lateralize the hyperseceting gland before adrenalectomy
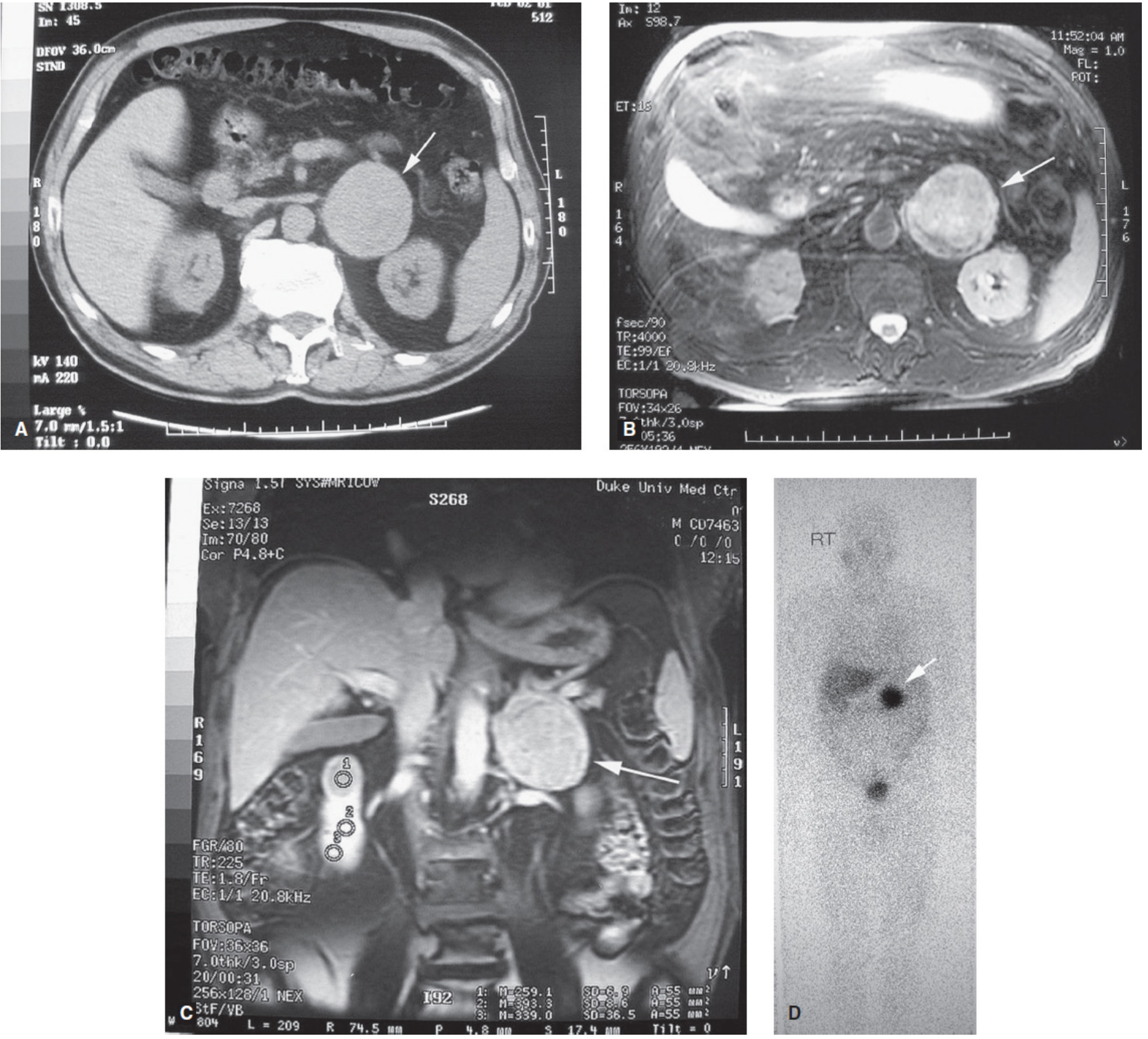
4. Pheochromocytoma
Tumor of the adrenal medulla producing excess catecholamines (epinephrine, norepinephrine). The "10% rule" (10% bilateral, 10% malignant, 10% extraadrenal - i.e., paraganglioma) is classically cited, though modern studies show higher rates.
Classic symptoms: paroxysmal hypertension, diaphoresis, headache, palpitations, anxiety. Present in >60% of patients.
Diagnosis:
- 24-hr urine fractionated catecholamines and metanephrines: sensitivity and specificity ~98%
- Plasma-fractionated metanephrines: sensitivity 99%, specificity 85%
- CT/MRI for localization: CT sensitivity 87-100%; MRI T2 brightness >3× liver is highly specific
- 131-I MIBG scan for extraadrenal, malignant, or equivocal cases; 68Ga-DOTATATE PET-CT now preferred for better sensitivity/resolution
Preoperative preparation (mandatory before surgery):
- Alpha-adrenergic blockade first - phenoxybenzamine 10 mg BD, increasing by 10-20 mg/day until BP normalizes and orthostasis develops (1-3 weeks preoperatively). Alternatives: doxazosin, terazosin (cheaper, better tolerated); calcium channel blockers (less effective)
- Beta blockade only after alpha blockade - propranolol for tachycardia/arrhythmia. Starting beta before alpha causes unopposed alpha stimulation and reflex hypertension
- Volume loading - oral salt tablets/high-salt diet several days before surgery to restore intravascular volume and reduce intraoperative hemodynamic shifts
- Metyrosine (tyrosine hydroxylase inhibitor) can be added in the week before surgery for patients with very high catecholamine excess - expensive but effective
- Preoperative echocardiogram if longstanding or very elevated catecholamines (catecholamine-excess cardiomyopathy)
Intraoperative requirements: arterial line, central venous access, anesthesiologist experienced with pheochromocytoma
Postoperative: hypotension and hypoglycemia are common after tumor removal. ICU for 48 hrs; 20-70% require vasopressor support.
- Mulholland and Greenfield's Surgery 7e, p. 4181-4183; Fischer's Mastery of Surgery 8e, p. 371-372
5. Adrenocortical Carcinoma (ACC)
Rare (1-2 per million/year), but ACC carries ~50% 5-year disease-specific survival. <2% of adrenal tumors are ACC.
- Open adrenalectomy is the approach of choice (laparoscopic is contraindicated in suspected ACC) - allows optimal exposure for wide local excision and vascular reconstruction if needed
- Key concern: capsular rupture leads to incurable peritoneal spread
Adrenalectomy: Surgical Approaches
1. Laparoscopic Transabdominal Adrenalectomy (Gold Standard for Most)
- Patient in lateral decubitus position, affected side up
- Table flexed at the waist to open rib-iliac crest space
- 3-4 ports placed transversely from lateral rectus sheath to midaxillary line
- Right adrenalectomy: mobilize liver, retract right lobe anteromedially; identify and ligate the short right adrenal vein into the IVC
- Left adrenalectomy: mobilize splenic flexure, colon, and spleen; retract spleen/pancreas/stomach medially en bloc; identify left adrenal vein (drains to left renal vein)
- Hand-port modification available for large or friable tumors
2. Posterior Retroperitoneoscopic Adrenalectomy (PRA)
- Patient in prone jackknife position, hips and knees at 90° angles
- Three ports placed at/near the 12th rib; pneumoretroperitoneum to 20-24 mmHg
- Avoids abdominal cavity completely - ideal for patients with prior abdominal surgery
- Can do bilateral adrenalectomy without repositioning
- Adrenal vein identification is reportedly easier than transabdominal approach
- NOT suitable for tumors >6 cm or suspected malignancy
3. Anterior Open Adrenalectomy
- Bilateral subcostal (Chevron) incision or ipsilateral subcostal
- Explore for metastatic disease
- Right: mobilize right hepatic lobe; enter retroperitoneum behind liver; ligate right adrenal vein at IVC
- Left: mobilize spleen + pancreatic tail + left colon; retract medially en bloc; divide left adrenal vein
- Indications: large tumors (>6-8 cm), suspected ACC, intraoperative conversion from laparoscopic
4. Combined Thoracoabdominal Approach
- Less common; used for very large ACC or extensive local invasion
Key Surgical Principles (All Approaches)
| Principle | Rationale |
|---|---|
| Confirm correct surgical site (timeout) | Prevent wrong-side surgery |
| Minimal tumor handling | Prevents catecholamine surges (pheo) and capsular rupture |
| Early isolation and ligation of adrenal vein | Reduces catecholamine flooding into circulation |
| No capsular rupture | Rupture causes incurable spread even in benign tumors |
| Surgeon volume ≥6 adrenalectomies/year | Associated with better outcomes |
| Convert laparoscopic to open if needed | Safety principle |
- Mulholland and Greenfield's Surgery 7e, p. 4185-4188; Sabiston Textbook of Surgery, p. 1555-1560
Postoperative Considerations
- After unilateral adrenalectomy for Cushing's: contralateral adrenal suppression - administer perioperative and postoperative glucocorticoid cover, taper slowly over weeks-months
- After pheochromocytoma resection: monitor for hypotension, hypoglycemia; most require ICU for ~48 hrs
- After bilateral adrenalectomy: lifelong glucocorticoid and mineralocorticoid replacement (hydrocortisone + fludrocortisone)
- Stress-dose steroids: patients on chronic steroids or with adrenal insufficiency need stress-dose cover perioperatively
This is a shared conversation. Sign in to Orris to start your own chat.