Paediatrics research
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"micronutrient deficiency" AND children
Finding Sources
Finding Sources
Searching PubMed
"iron deficiency" AND children AND treatment
Searching PubMed
"vitamin D deficiency" AND children AND supplementation
Finding Sources
Finding Sources
Searching PubMed
"zinc deficiency" AND children AND growth
Searching PubMed
"vitamin A deficiency" AND children
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Here is a full research summary on paediatric micronutrient deficiencies, integrating authoritative textbook content and recent peer-reviewed evidence.
Paediatric Micronutrient Deficiencies: Research Summary
Micronutrient malnutrition ("hidden hunger") affects an estimated 2 billion people globally, with children under five being the most vulnerable group. The major deficiencies with clinical relevance in paediatrics are iron, vitamin D, vitamin A, zinc, and iodine.
1. Iron Deficiency and Iron Deficiency Anaemia (IDA)
Epidemiology & Clinical Impact
Iron deficiency anaemia is the most widespread micronutrient deficiency, affecting all age groups regardless of gender, caste, creed, or religion. Even mild anaemia reduces resistance to fatigue and has a profound effect on psychological and physical behaviour in children. - Park's Textbook of Preventive and Social Medicine, p. 641
At-Risk Paediatric Groups
- Infants 6-24 months (rapid growth, low dietary iron density)
- Preterm/low birth weight neonates (depleted stores)
- Adolescent girls (menstrual losses)
- Children with malabsorptive or inflammatory bowel conditions
Prevention and Treatment Dosing
Per national programme guidance:
-
Infants 6 months to 5 years: 20 mg elemental iron + 100 mcg folic acid per day for 100 days/year
-
Children 6-10 years: 30 mg elemental iron + 250 mcg folic acid for 100 days/year
-
>10 years: adult dose schedule
-
Park's Textbook of Preventive and Social Medicine, p. 513
Recent Evidence
- A 2025 systematic review and meta-analysis (PMID 39951396) specifically addressing optimal dose and duration of iron supplementation for children and adolescents with IDA found that standard oral iron therapy is effective, but dosing frequency and duration vary widely in practice - this review provides guidance on optimising regimens.
- A 2024 Polish Paediatric Society practice guideline (PMID 39519457) gives updated recommendations for diagnosis (serum ferritin, Hb thresholds) and treatment of IDA in children, including when to escalate to IV iron.
- A 2023 meta-analysis (PMID 36728680) on ferrous bisglycinate showed this chelated form significantly raises Hb and ferritin compared with placebo, with potentially better GI tolerability than ferrous sulphate.
- A 2024 BMJ Global Health meta-analysis (PMID 38599666) found that overnutrition/obesity is a risk factor for iron deficiency (due to hepcidin-mediated sequestration) but not for zinc or vitamin A deficiency in children.
2. Vitamin D Deficiency and Rickets
Pathophysiology
Vitamin D is synthesised in skin from 7-dehydrocholesterol under UVB radiation, then hydroxylated in the liver to 25(OH)D and subsequently in the kidney to the active form 1,25(OH)2D (calcitriol). Calcitriol stimulates intestinal calcium absorption via TRPV6 channels, renal calcium reabsorption via TRPV5, and regulates osteoblast/osteoclast activity through the RANKL-RANK pathway. When vitamin D is deficient, hypophosphataemia persists despite secondary hyperparathyroidism, impairing bone mineralisation. - Robbins, Cotran & Kumar Pathologic Basis of Disease
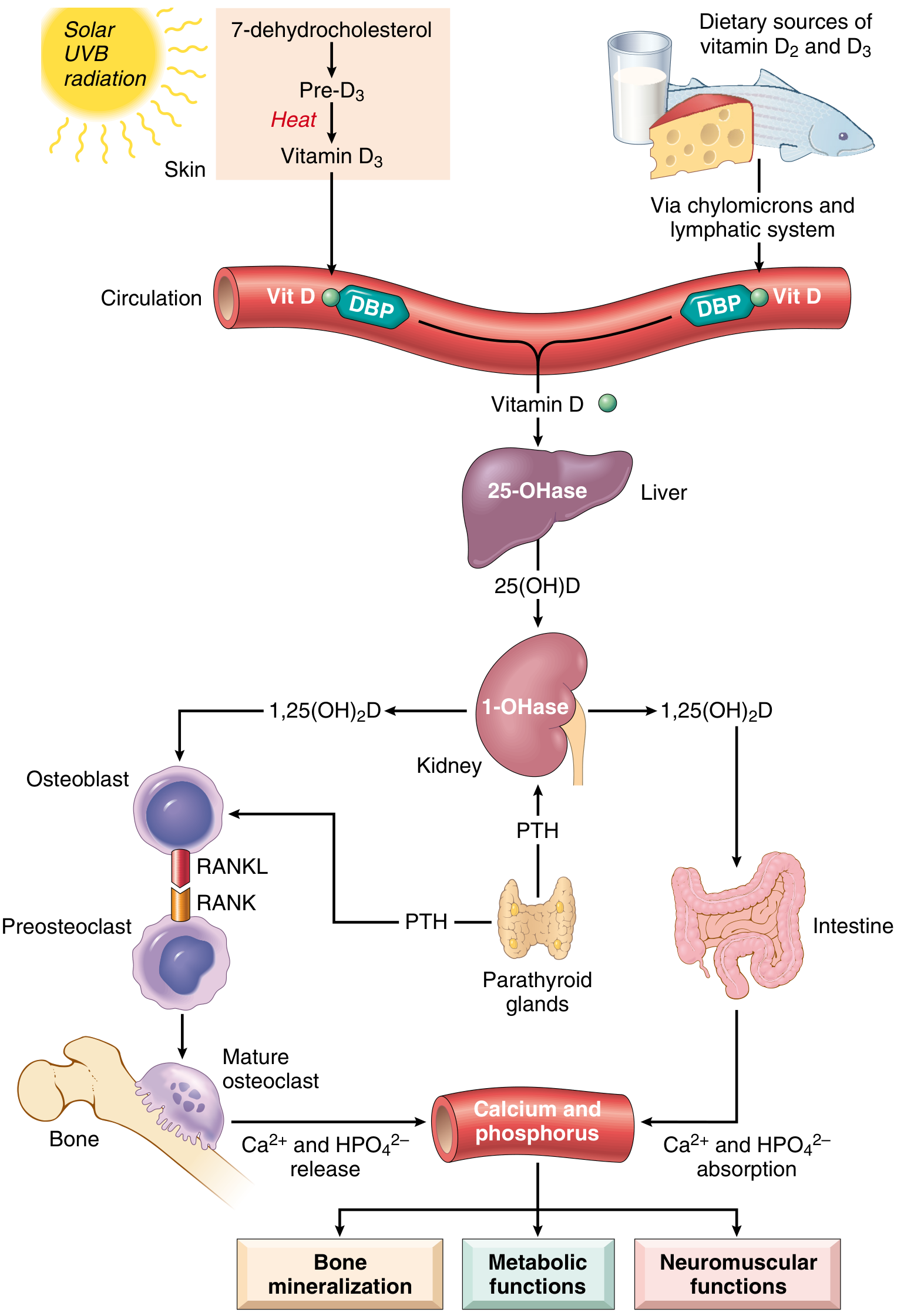
Deficiency Threshold
25-(OH)-D < 20 ng/mL constitutes vitamin D deficiency. - Robbins, Cotran & Kumar
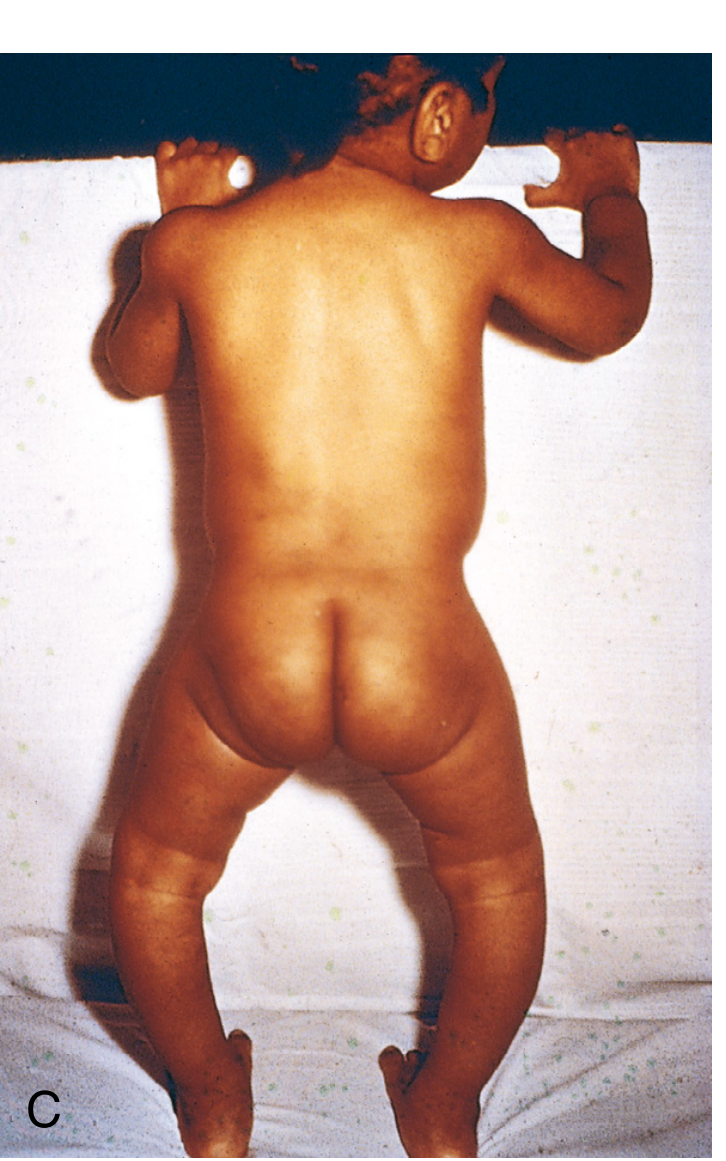
Rickets in Children
Rickets is a disease in children attributable to vitamin D deficiency, characterised by:
- Continued osteoid formation without mineralisation
- Deformity of long bones (bow legs, knock knees)
- Rachitic rosary (costochondral junction enlargement)
- Craniotabes, widened epiphyses, delayed dentition
Causes include: dietary deficiency, limited sunlight exposure (northern latitudes, heavily veiled mothers), prematurity, malabsorption, and rare inherited disorders (vitamin D-dependent and vitamin D-resistant/hypophosphataemic rickets). Treatment with vitamin D 1000-6000 IU daily (weight-based) resolves most deformities. - Miller's Review of Orthopaedics, 9th Edition
Classic clinical photo of rickets (genu varum/bow legs):
Toxicity Warning
Megadoses of oral vitamin D cause hypervitaminosis D - in children this manifests as metastatic calcification of soft tissues (particularly the kidney). - Robbins, Cotran & Kumar
Recent Evidence
- A 2023 individual participant data meta-analysis (PMID 37661104) confirmed vitamin D supplementation significantly improves bone density in vitamin D-deficient children and adolescents.
- A 2024 Cochrane-style meta-analysis (PMID 37428896) found high-dose oral vitamin D in children under 5 reduced the incidence of respiratory tract infections.
- A 2025 systematic review (PMID 41129483) showed maternal vitamin D supplementation during pregnancy has positive downstream effects on childhood bone health and immune function.
3. Vitamin A Deficiency
Epidemiology
Vitamin A deficiency is the single most common cause of preventable blindness among pre-school children in developing countries. Young children are at greatest risk because their requirements are proportionately higher and because infections deplete vitamin A stores. Severe, blinding corneal destruction (xerophthalmia) is most common in children aged 6 months to 6 years. Around 20% of children with deficiency face increased mortality risk from common infections. - Park's Textbook of Preventive and Social Medicine, p. 641
WHO/National Supplementation Programme
- First dose: 1 lakh (100,000) IU at 9 months (with measles vaccination)
- Second dose: 2 lakh (200,000) IU after 9 months
- Subsequent doses: 2 lakh IU every 6 months up to age 5
- Additional dose for severe malnutrition
Clinical Features
| Stage | Finding |
|---|---|
| Night blindness | Earliest sign |
| Xerosis (conjunctival/corneal) | Bitot's spots |
| Keratomalacia | Corneal ulceration/melting - can cause permanent blindness |
| Increased infection susceptibility | Measles severity, diarrhoeal deaths |
Recent Evidence
- A 2024 Cochrane review (PMID 38738639) found that oral vitamin A supplementation does not significantly prevent acute upper respiratory tract infections in children under 7, despite immunological plausibility.
- A 2025 Cochrane systematic review (PMID 40433851) evaluated laboratory biomarkers for vitamin A deficiency and found retinol-binding protein is a practical, cost-effective surrogate for serum retinol, particularly in low-resource settings.
4. Zinc Deficiency
Clinical Significance
Zinc is required for over 300 enzymatic reactions. In children, deficiency causes:
- Growth stunting (height and weight faltering)
- Impaired immune function
- Diarrhoeal disease and increased susceptibility to pneumonia
- Delayed sexual maturation
- Acrodermatitis enteropathica (severe inherited deficiency)
Protein deficiency (kwashiorkor) also leads to growth stunting; children with kwashiorkor are actually less stunted than those with marasmus since oedema masks the weight deficit. - Harper's Illustrated Biochemistry, 32nd Ed
Treatment
Zinc supplementation (10-20 mg/day depending on age) is recommended alongside ORS in childhood diarrhoea (WHO/UNICEF protocol). It is also used in severe acute malnutrition management.
Recent Evidence
- A 2023 meta-analysis (PMID 37612628) of zinc supplementation in healthy children over 2 years showed modest but statistically significant improvements in height-for-age Z-scores and weight-for-age, supporting routine supplementation in zinc-deficient populations.
- A 2024 BMJ Global Health meta-analysis (PMID 38599666) noted zinc deficiency is not associated with overnutrition/obesity, distinguishing it from iron deficiency.
5. Iodine Deficiency
Iodine deficiency remains the most common cause of preventable hypothyroidism and goitre worldwide. About 1.5 billion people live in iodine-deficient environments. Consequences in children include:
- Cretinism (severe intellectual disability, deafness, physical stunting) from in-utero deficiency
- Goitre
- Subclinical cognitive impairment and apathy even without overt cretinism
- At least 30,000 stillbirths and 120,000 mentally retarded births per year globally
Prevention: Universal salt iodisation (USI) is the primary strategy. - Park's Textbook of Preventive and Social Medicine, p. 641; Scott-Brown's Otorhinolaryngology
Summary Table: Key Paediatric Micronutrient Deficiencies
| Micronutrient | Key Clinical Manifestation | High-Risk Age Group | Primary Prevention |
|---|---|---|---|
| Iron | Anaemia, fatigue, cognitive impairment | 6 mo - 2 yr; adolescent girls | Supplementation, fortified foods |
| Vitamin D | Rickets, hypocalcaemic seizures | Infants, veiled/dark-skinned children | 400-1000 IU/day supplementation |
| Vitamin A | Xerophthalmia, blindness, infection severity | 6 mo - 6 yr | 6-monthly mega-dose programme |
| Zinc | Stunting, diarrhoea, immune deficiency | Under-5s, low-income settings | Dietary diversification, supplementation |
| Iodine | Goitre, cretinism, cognitive dullness | Fetal/neonatal period; school age | Iodised salt |
Key Recent Evidence (PubMed, 2023-2026)
| PMID | Study | Key Finding |
|---|---|---|
| 39951396 | SR/MA - IDA treatment in children (2025) | Establishes optimal iron dose and duration |
| 39519457 | Practice guideline - IDA paediatrics (2024) | Polish Paediatric Society diagnostic and treatment recommendations |
| 37661104 | IPD meta-analysis - Vit D supplementation (2023) | Significantly improves bone density in deficient children |
| 37428896 | Meta-analysis - High-dose Vit D under-5s (2024) | Reduces respiratory infection incidence |
| 37612628 | SR/MA - Zinc supplementation & growth (2023) | Improves height-for-age and weight in children |
| 38738639 | Cochrane - Vit A & RTIs (2024) | No benefit of Vit A for upper respiratory infections |
| 40433851 | Cochrane - Vit A biomarkers (2025) | Retinol-binding protein is a valid surrogate measure |
Sources: Park's Textbook of Preventive and Social Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease; Harper's Illustrated Biochemistry, 32nd Ed; Miller's Review of Orthopaedics, 9th Ed; PubMed systematic reviews and meta-analyses (2023-2026).
This is a shared conversation. Sign in to Orris to start your own chat.