Lobar pneumonia
Reading File
Finding Sources
Searching PubMed
"lobar pneumonia" AND "community-acquired pneumonia"
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have rich content from multiple authoritative sources. Let me compile a comprehensive answer.
Lobar Pneumonia
Definition and Overview
Lobar pneumonia is an acute bacterial infection characterized by consolidation of an entire lobe (or large portion thereof) of the lung. It is distinguished from bronchopneumonia, which shows patchy, multifocal consolidation. The distinction can be blurry in practice - the same organisms may produce either pattern depending on host susceptibility, and patchy bronchopneumonia may become confluent and mimic a lobar pattern.
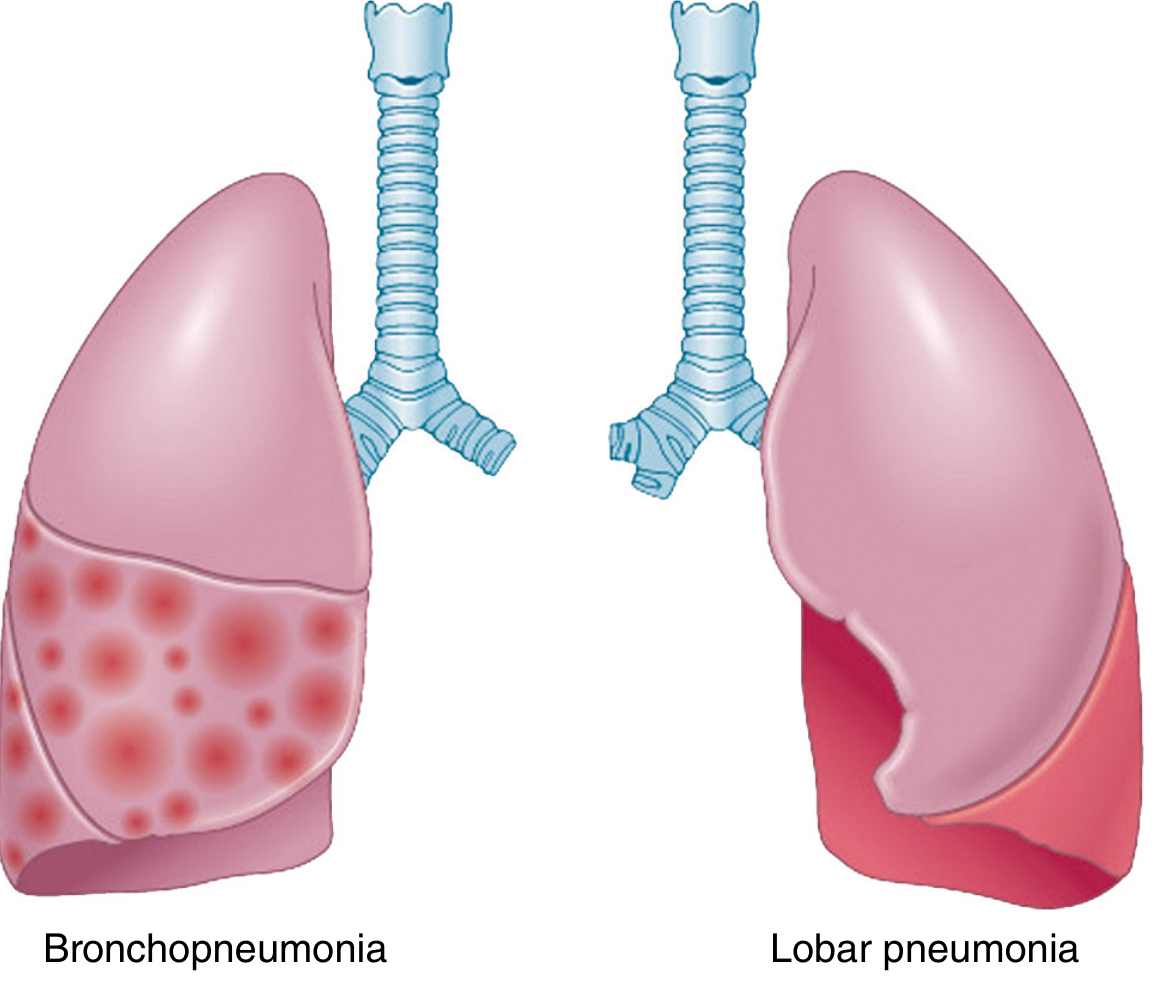
Fig. 15.28 - Comparison of bronchopneumonia and lobar pneumonia (Robbins, Cotran & Kumar Pathologic Basis of Disease)
Etiology
The most common and classic cause is Streptococcus pneumoniae (pneumococcus), responsible for ~one-third of all community-acquired pneumonia (CAP) cases and the organism most typically associated with the lobar pattern.
Other organisms producing lobar consolidation include:
| Organism | Key Context |
|---|---|
| Klebsiella pneumoniae | Alcoholics/malnourished; classic RUL; bulging fissure |
| Legionella pneumophila | Transplant recipients, immunocompromised, contaminated water exposure |
| Haemophilus influenzae | COPD exacerbations |
| Staphylococcus aureus | Post-viral (influenza), neutropenic patients |
| Pseudomonas aeruginosa | Cystic fibrosis, burn victims, neutropenia |
S. pneumoniae infections peak in winter/spring, often preceded by a viral respiratory illness. Risk factors include extremes of age, chronic cardiopulmonary disease, immunosuppression, alcoholism, institutionalization, and prior splenectomy. - Grainger & Allison's Diagnostic Radiology, p. 3279
Pathogenesis
The infective organism induces inflammatory edema within the alveoli. Bacteria spread through the alveolar pores of Kohn across the entire lobe, bypassing the bronchi - this is why the airways remain patent (giving the characteristic air bronchogram) while surrounding alveoli fill with exudate. - Fishman's Pulmonary Diseases and Disorders, p. 193
Morphology - The Four Classic Stages
Lobar pneumonia evolves through four sequential stages of the inflammatory response:
1. Congestion (Day 1-2)
- Lung is heavy, boggy, and red
- Vascular engorgement + intra-alveolar edema fluid
- Few neutrophils; numerous bacteria
- Microscopically: protein-rich fluid, sparse inflammatory cells
2. Red Hepatization (Day 2-4)
- Massive confluent exudation: neutrophils + red cells + fibrin fill alveolar spaces
- Gross: lobe is red, firm, airless, liver-like consistency (hence "hepatization")
- Microscopically: densely packed neutrophils and RBCs within alveoli (Panel A below)
3. Gray Hepatization (Day 4-8)
- Red cells progressively lysed and degraded
- Persistence of a fibrinopurulent exudate; dominant cell = neutrophil
- Gross: lobe turns grayish-brown
- Microscopically: fibrin strands + degenerate neutrophils; fewer RBCs (Panel B below)
4. Resolution (Day 8+)
- Exudate broken down by enzymatic digestion → granular, semifluid debris
- Debris is resorbed, ingested by macrophages, or expectorated
- Fibroblasts may organize residual exudate
- Pleural fibrinous reaction may resolve or leave fibrous adhesions (Panel C below)
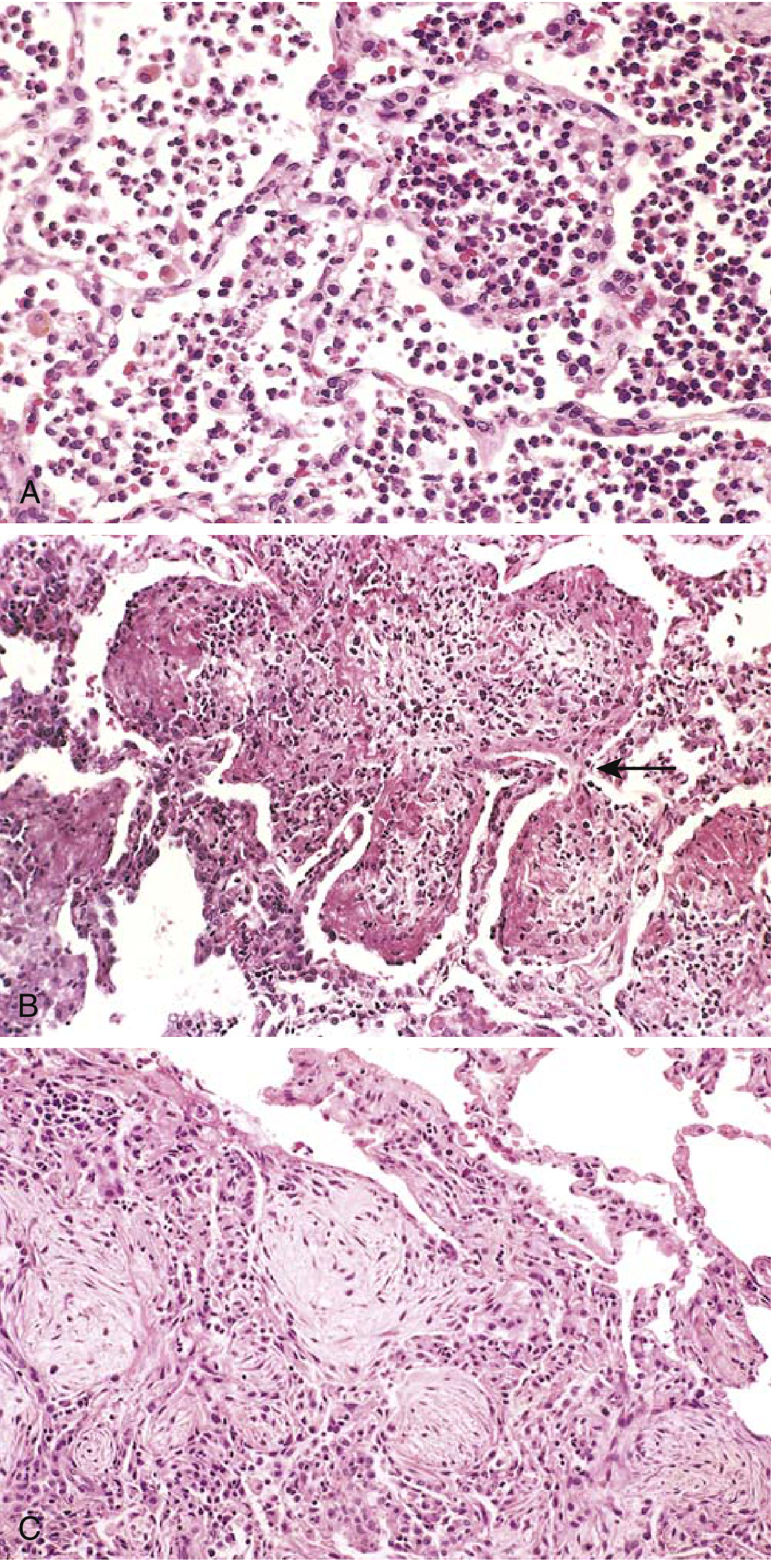
Fig. 15.30 - The three histologic stages of lobar pneumonia: red hepatization (A), gray hepatization (B), and resolution (C). (Robbins Basic Pathology)
Bacterial pneumonias are characterized by predominantly intra-alveolar neutrophilic inflammation, distinguishing them from viral pneumonias (interstitial lymphocytic inflammation). - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 3608
Clinical Features
| Feature | Detail |
|---|---|
| Onset | Abrupt - fever, rigors/chills |
| Cough | Initially dry, then productive (rusty sputum in pneumococcal) |
| Pleuritic chest pain | Due to involvement of pleura |
| Dyspnea | From consolidation + reduced lung volume |
| Signs | Decreased breath sounds, dullness to percussion, bronchial breathing, increased vocal fremitus over affected lobe |
In the elderly, classic features may be absent - pneumonia may mimic or be confused with congestive heart failure, pulmonary embolism, or malignancy. - Grainger & Allison's, p. 3279
Radiology
Chest X-ray:
- Homogeneous non-segmental consolidation (crosses segmental boundaries, respects lobar boundaries)
- Air bronchogram - the hallmark sign: airway outline made visible as surrounding alveoli fill with fluid/exudate
- Minimal or no volume loss (distinguishes from atelectasis)
- Pleural effusion in up to 50% of S. pneumoniae cases
CT findings:
- Dense homogeneous consolidation with prominent air bronchograms
- CT angiogram sign: enhancement of branching pulmonary vessels within the low-attenuation consolidated parenchyma (also seen in lepidic adenocarcinoma)
- Round pneumonia: spherical consolidation that can simulate a mass
Klebsiella pneumonia classically shows RUL consolidation with bulging of the fissure (due to volume increase), sharp margins, and early abscess formation - though these features are not pathognomonic without bacteriologic confirmation. - Grainger & Allison's, p. 3290
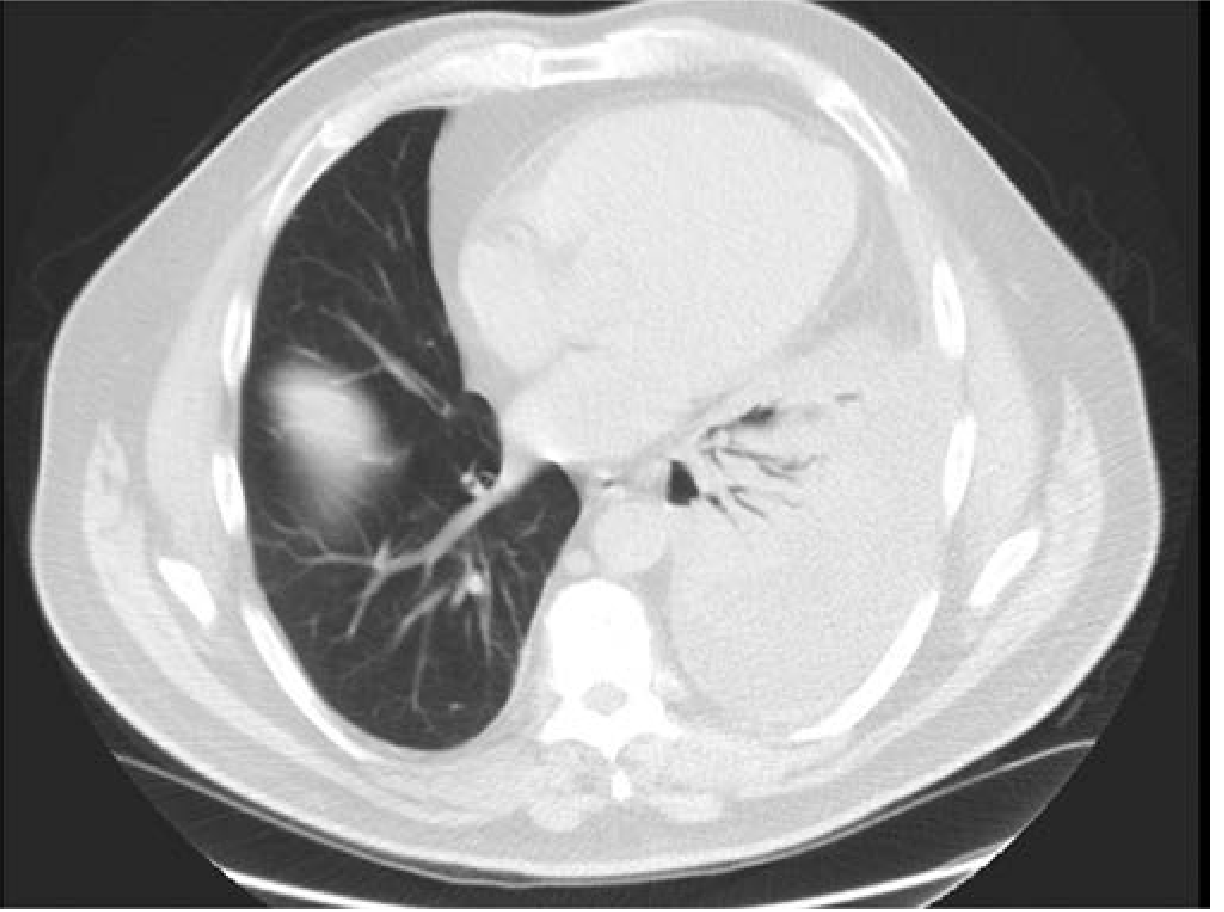
CT scan of left-sided lobar pneumonia - note the complete left lower lobe consolidation with visible air bronchograms (Fishman's Pulmonary Diseases)
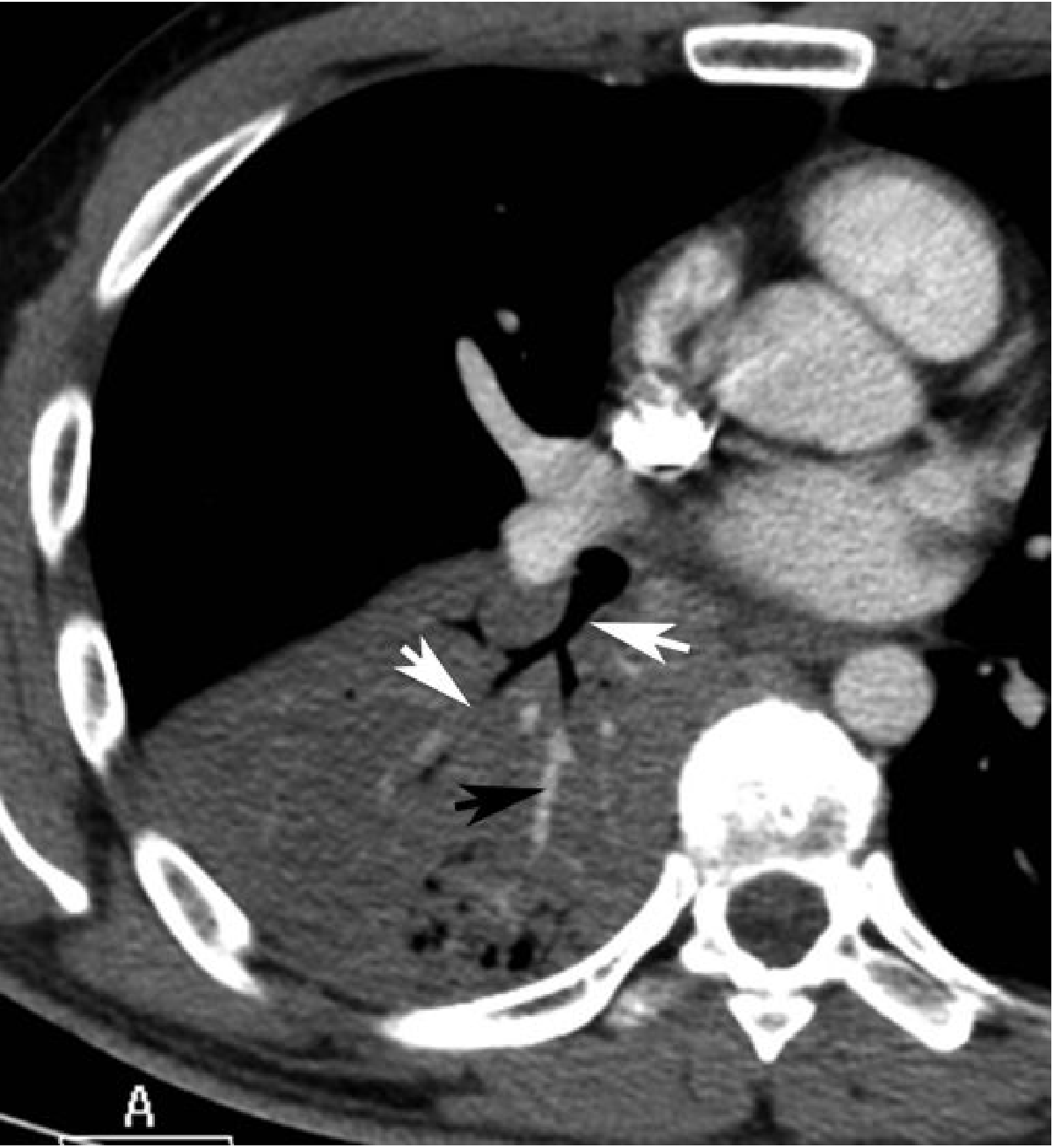
Fig. 5.7 - Lobar pneumococcal pneumonia: dense consolidation, air bronchogram (white arrows), CT angiogram sign (black arrow) (Grainger & Allison's Diagnostic Radiology)
Investigations
- Blood cultures - frequently positive in lobar bacterial pneumonia
- Sputum Gram stain and culture
- Urinary antigen tests - for S. pneumoniae and Legionella
- CBC - leukocytosis with neutrophilia
- CRP/procalcitonin - elevated
- Severity scoring - CURB-65 or PSI/PORT score for risk stratification
A lobar consolidation pattern has a specificity of 90% and LR+ of 5.6 for bacterial pneumonia (vs. PCP or pulmonary TB). - Symptom to Diagnosis, p. 8600
Complications
- Pleural effusion / Empyema - parapneumonic effusion common; empyema requires drainage
- Lung abscess - particularly with S. aureus, Klebsiella, anaerobes
- Bacteremia / Sepsis
- ARDS - with extensive bilateral involvement
- Organizing pneumonia - if resolution is incomplete
- Fibrous pleuritis - from pleural inflammation
Lobar Pneumonia vs. Bronchopneumonia
| Feature | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Pattern | Entire lobe consolidated | Patchy, multifocal |
| Spread | Via alveolar pores | Via airways |
| Air bronchograms | Prominent | Less prominent |
| Volume loss | Absent/minimal | Variable |
| Classic organism | S. pneumoniae | S. aureus, H. influenzae, Gram-negatives |
| Setting | Community-acquired | HAP, aspiration, post-viral |
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease | Fishman's Pulmonary Diseases and Disorders | Grainger & Allison's Diagnostic Radiology | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.