Brachial plexus palsy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"brachial plexus" AND palsy
Reading File
Reading File
Searching Images
brachial plexus anatomy diagram Erb Klumpke palsy
Reading File
I now have comprehensive, authoritative content from multiple textbooks. Here is a complete synthesis:
Brachial Plexus Palsy
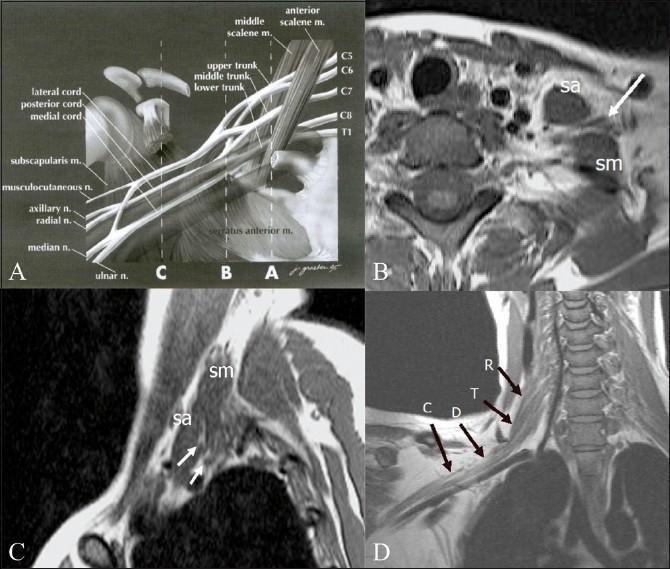
Anatomy Overview
The brachial plexus arises from nerve roots C5–T1, forming trunks → divisions → cords → terminal branches that supply the entire upper extremity. Injury anywhere along this chain produces characteristic patterns of motor and sensory deficit.
Classification by Level
Three clinically recognized patterns:
| Type | Roots | Deformity | Prognosis |
|---|---|---|---|
| Erb-Duchenne palsy | C5, C6 | "Waiter's tip" — shoulder adducted + internally rotated, elbow extended | Best; most common |
| Klumpke palsy | C8, T1 | "Claw hand" — intrinsic hand muscle weakness; ± Horner syndrome | Poor |
| Total plexus palsy | C5–T1 | Complete arm paralysis | Worst |
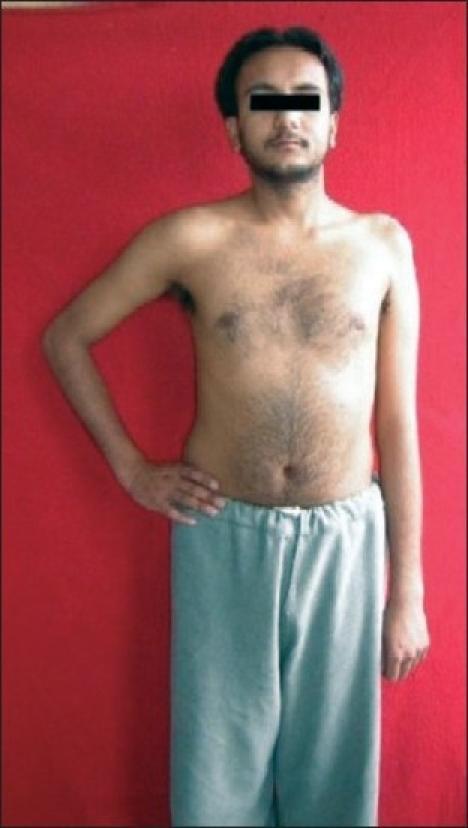
Erb's Palsy (C5, C6)
- Most common form (~90% of birth palsies)
- Loss of shoulder abduction/external rotation and elbow flexion
- Arm hangs at side, internally rotated ("waiter's tip" or "bellhop's tip" position)
- Biceps reflex absent; asymmetric Moro reflex
- Hand movements typically spared
Klumpke's Palsy (C8, T1)
- Rare; results from stretch or compression of lower plexus
- Claw hand deformity; intrinsic hand muscle weakness (resembles ulnar nerve injury)
- Grasp reflex absent
- Associated with Horner syndrome (ptosis, miosis, anhidrosis) from T1 sympathetic fiber involvement
Etiology
Birth (Obstetric) Brachial Plexus Palsy
- Incidence: ~2 per 1,000 live births
- Risk factors: large neonate, shoulder dystocia, forceps/vacuum delivery, breech presentation, prolonged labor
- Mechanism: lateral neck stretch during delivery forces head away from shoulder, stretching the plexus
- May co-occur with: fractured clavicle or humerus, cervical cord injury, facial palsy, diaphragmatic paralysis (C3–C5 injury)
Adult/Traumatic Brachial Plexus Injury
- Motorcycle accidents (high-energy traction/avulsion)
- Glenohumeral joint dislocation
- Fall on outstretched hand (abrupt shoulder girdle movement)
- Penetrating/sharp injury
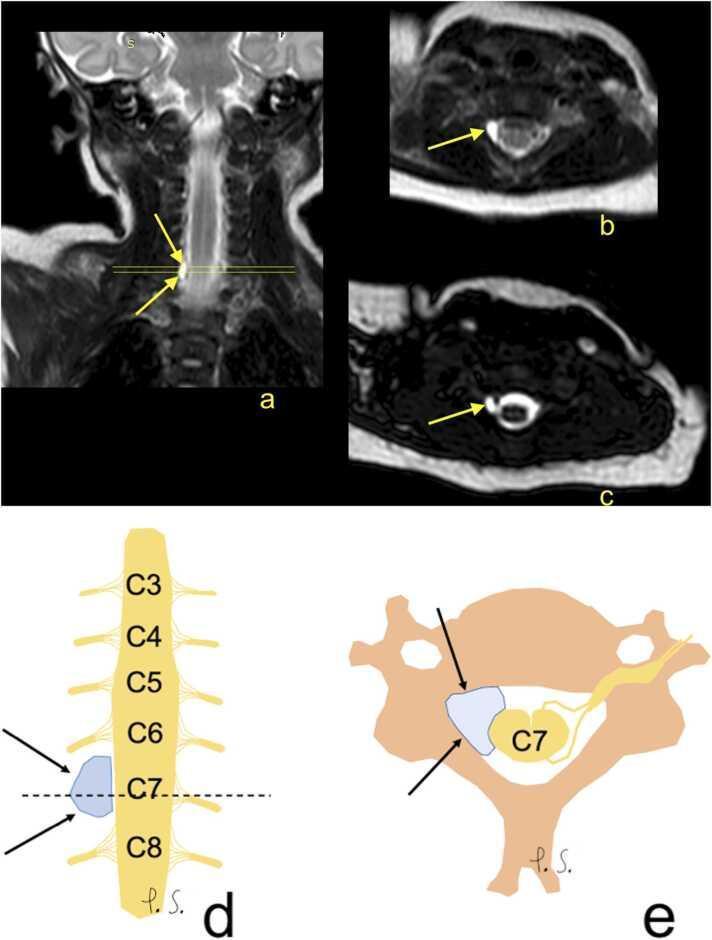
- Pancoast tumor (apical lung tumor — compressive, lower trunk)
Pathology of Nerve Injury (Sunderland/Seddon)
| Grade | Type | Definition | Recovery |
|---|---|---|---|
| I | Neurapraxia | Temporary failure, no axonal disruption | Hours to months (often 2–4 weeks) |
| II | Axonotmesis | Axon disrupted, endoneurium intact; Wallerian degeneration distally | Possible; axons regenerate at ~1 mm/day |
| III | Neurotmesis | Axons + endoneurium disrupted; epineurium may or may not be intact | Poor without surgery; neuroma formation common |
Nerve root avulsion (preganglionic) is the most severe form — radiologically seen as pseudomeningocele on MRI/CT myelography.
Clinical Features
- Shoulder: internal rotation contracture; progressive glenoid hypoplasia in ~70% of children with significant contracture
- Elbow and wrist: flexion contractures
- Posterior subluxation of the humeral head with glenoid erosion — must be actively prevented
- Hand function varies with level of injury
Investigations
- Serial clinical examination is the cornerstone (EMG/NCS technically challenging in neonates)
- EMG/NCS: perform at 3–6 weeks post-injury if deficits persist (before 3 weeks, Wallerian degeneration is incomplete, making results uninformative)
- Axillary lateral radiograph: evaluate humeral head position in glenoid
- CT scan: preferred over MRI for surgical planning of shoulder reconstruction (better bone detail)
- MRI: identifies pseudomeningocele and nerve root avulsion in severe cases
Prognosis
| Factor | Implication |
|---|---|
| Improvement within 2–4 weeks | Full recovery likely |
| Absent biceps function at 3 months | Indication for surgical reconstruction |
| Absent biceps function at 6 months | Poor prognosis |
| Horner syndrome | Poor prognosis |
| Total plexus palsy | Worst prognosis |
-
90% of birth palsy cases eventually resolve without intervention
- ~25% of patients have persistent deficits
Treatment
Conservative (First-line)
- Passive range of motion (ROM) exercises — key to preventing contractures
- Focus on: passive elbow motion, shoulder elevation, abduction, and external rotation
- Occupational + physical therapy at specialized multidisciplinary center by 1 month of age
- Await return of motor function up to 18 months
Surgical Options
Early surgery (nerve-focused):
- Microsurgical nerve grafting — typically using sural nerve as graft (sensory only, minor donor deficit)
- Indicated if no spontaneous recovery by 3 months
- Intraoperative electrical testing: if conduction present → observe; if absent → resect and anastomose
Late surgery (deformity correction):
- Latissimus dorsi and teres major transfer to external rotators of shoulder (L'Episcopo procedure)
- Tendon transfers for elbow flexion — Clark pectoral transfer, Steindler flexorplasty
- Pectoral and subscapularis release for internal rotation contracture + glenoid hypoplasia (< 5 years old)
- Subscapularis tendon release before age 2 → improved active external rotation
- Proximal humerus rotational osteotomy (> 5 years old)
Key Exam Points (High-Yield)
- Erb palsy = C5/C6 = waiter's tip = most common = best prognosis
- Klumpke palsy = C8/T1 = claw hand + Horner syndrome = poor prognosis
- No biceps function at 3 months → consider surgery; at 6 months → poor prognosis
- Horner syndrome = poor prognostic sign
- Glenoid hypoplasia develops in 70% of children with significant internal rotation contracture
- Axon regeneration rate = 1 mm/day; recovery window up to 18 months
- EMG/NCS: wait 3–6 weeks before performing (Wallerian degeneration must be complete)
Sources: Miller's Review of Orthopaedics 9th Ed., p. 260; Bradley & Daroff's Neurology in Clinical Practice, p. 2870; Schwartz's Principles of Surgery 11th Ed., p. 1804
This is a shared conversation. Sign in to Orris to start your own chat.