Explain me follicles stimulating hormone
Reading File
Finding Sources
Searching the Web
follicle stimulating hormone FSH physiology mechanism of action
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough, well-sourced answer. Here it is:
Follicle-Stimulating Hormone (FSH)
1. What Is FSH?
FSH is a gonadotropin - a glycoprotein polypeptide hormone synthesized and secreted by gonadotropic cells of the anterior pituitary gland. It works closely with luteinizing hormone (LH) to regulate reproduction, gametogenesis, and sex steroid synthesis in both males and females.
2. Structure
FSH is a heterodimer consisting of two non-covalently linked subunits:
- Alpha (α) subunit - 96 amino acids, identical to the α-subunit of LH, TSH, and hCG. This shared subunit explains why very high levels of one glycoprotein hormone can sometimes weakly activate receptors of another (e.g., very high hCG in pregnancy can stimulate TSH receptors, causing transient hyperthyroidism).
- Beta (β) subunit - 111 amino acids, hormone-specific. The β-subunit confers FSH's unique biological activity and determines its receptor binding. The gene encoding FSHβ is on chromosome 11p13.
Goldman-Cecil Medicine, p. 1832
3. Regulation - The HPG Axis
FSH secretion is governed by the hypothalamic-pituitary-gonadal (HPG) axis:
| Signal | Effect on FSH |
|---|---|
| GnRH (pulsatile) from hypothalamus | Stimulates FSH release |
| GnRH (continuous) | Suppresses FSH (used pharmacologically) |
| Inhibin B (from granulosa/Sertoli cells) | Inhibits FSH (negative feedback) |
| Activin | Enhances FSH synthesis |
| Estrogen (low-moderate levels) | Inhibits FSH (negative feedback) |
| Estrogen (high sustained levels) | Positive feedback - triggers LH/FSH surge |
The hypothalamus releases GnRH in a pulsatile manner into the hypophyseal portal circulation. GnRH acts on G-protein-coupled receptors on gonadotropes to stimulate FSH and LH secretion. During puberty, this pulsatile pattern is initiated, triggering the pubertal increase in FSH and LH.
4. Mechanism of Action
FSH acts through G-protein-coupled receptors (GPCR) on target cell membranes. The receptor has:
- An extracellular domain that binds FSH
- A transmembrane domain
- An intracellular domain that transduces the signal (via cAMP/PKA pathway)
Mutations in the extracellular domain can cause constitutive receptor activation (FSH-like state even without FSH present - e.g., precocious puberty). Conversely, loss-of-function mutations render the receptor insensitive, causing primary hypogonadism despite high FSH levels.
Goldman-Cecil Medicine, p. 1832
5. Physiological Actions
In Females
FSH receptors are located on granulosa cells of ovarian follicles.
Two-Cell, Two-Gonadotropin Theory (the central concept of ovarian steroidogenesis):
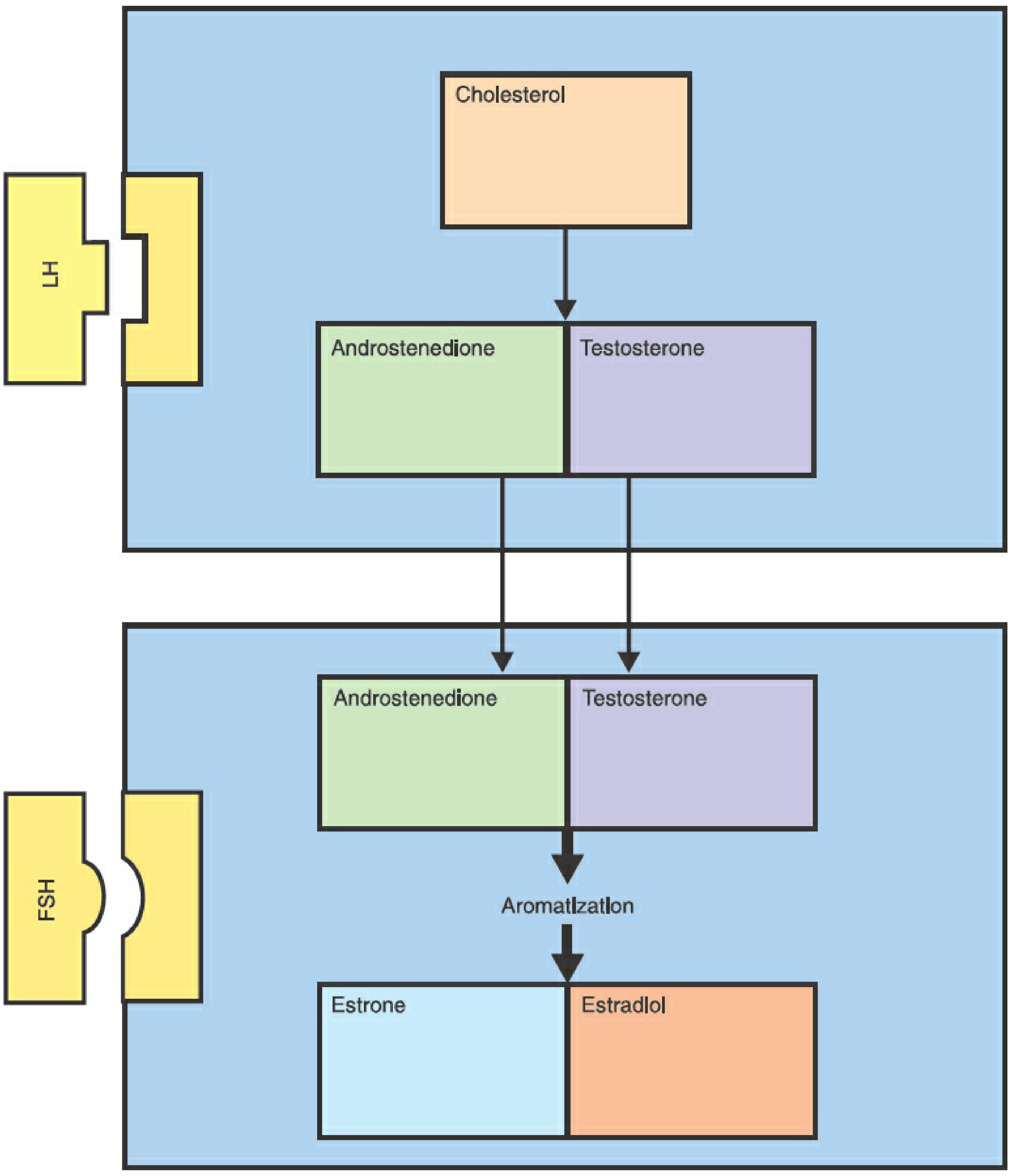
- LH stimulates theca cells to convert cholesterol → androstenedione and testosterone
- These androgens diffuse into the adjacent granulosa cells
- FSH stimulates granulosa cell aromatase, converting those androgens → estrone and estradiol
- The two cell types must cooperate: granulosa cells lack the early steroidogenic enzymes; theca cells lack aromatase
Berek & Novak's Gynecology, p. 289
FSH during the menstrual cycle:
- Early follicular phase - FSH stimulates growth of a cohort of primordial follicles from primary to antral stage
- Positive feedback loop - estrogen in the follicle induces more FSH receptors on granulosa cells, making them more sensitive to FSH
- FSH + estrogen promote LH receptor expression on granulosa cells, priming them for the LH surge
- Dominant follicle selection - rising estrogen and inhibin B decrease FSH. Only the follicle with the most FSH receptors (richest estrogenic microenvironment) survives; all others undergo atresia
- Pre-ovulatory surge - FSH rises 2-3x alongside the major LH surge (~16 hours before ovulation)
Guyton & Hall Medical Physiology, pp. 1017-1018; Berek & Novak's Gynecology, p. 290
In Males
FSH receptors are located on Sertoli cells (and seminiferous tubules).
- FSH stimulates Sertoli cells to support sperm maturation and spermatogenesis
- Sertoli cells produce inhibin B, which feeds back to suppress FSH
- LH acts on Leydig cells to produce testosterone, which also supports spermatogenesis
- Together, FSH + LH are required for complete, normal spermatogenesis
Goldman-Cecil Medicine, p. 1834
6. Normal Reference Ranges
FSH levels vary significantly by sex and life stage:
| Condition | Approximate FSH Level |
|---|---|
| Adult males | 1.5 - 12.4 IU/L |
| Follicular phase (females) | 3.5 - 12.5 IU/L |
| Ovulatory surge | Up to ~20 IU/L |
| Luteal phase | 1.7 - 7.7 IU/L |
| Postmenopause | 25 - 135 IU/L (markedly elevated) |
| Prepubertal children | <2 IU/L |
7. Clinical Significance
High FSH
- Menopause / premature ovarian insufficiency (POI) - loss of ovarian follicles removes negative feedback
- Primary hypogonadism in males (e.g., Klinefelter syndrome) - testicular failure removes inhibin feedback
- FSH-secreting pituitary adenoma - rare; usually presents as a non-functional mass causing hypogonadism due to ineffective gonadotropin stimulation; men may develop testicular enlargement
Low FSH
- Hypogonadotropic hypogonadism - failure at the hypothalamus or pituitary (e.g., Kallmann syndrome, pituitary tumor, anorexia nervosa)
- Amenorrhea with low FSH and LH points to a central (hypothalamic or pituitary) cause, not an ovarian cause
FSH in Polycystic Ovary Syndrome (PCOS)
- Chronic androgen excess suppresses hypothalamic-pituitary FSH secretion
- Impaired FSH signaling prevents dominant follicle development → chronic anovulation
8. Pharmacological Uses
FSH preparations are used clinically for ovulation induction and assisted reproduction:
| Preparation | Source | Route |
|---|---|---|
| Urofollitropin | Purified from postmenopausal urine | SC (previously IM) |
| Follitropin alfa (recombinant) | Recombinant DNA (mammalian cells) | SC |
| Follitropin beta (recombinant) | Recombinant DNA (differs in glycosylation) | SC |
| Menotropins (hMG) | Urine-derived; contains both FSH and LH | IM or SC |
Indications:
- Controlled ovarian hyperstimulation for IVF
- Infertility due to hypogonadotropic hypogonadism (females and males)
Key toxicity: Ovarian hyperstimulation syndrome (OHSS) - excessive follicular development causing fluid shifts, ovarian enlargement, and risk of thrombosis. Multiple pregnancies are also a risk.
Katzung Basic & Clinical Pharmacology, p. 80-82; Goodman & Gilman, p. 954
Summary
FSH is the master regulator of follicular development in females and spermatogenesis in males. It operates within the HPG axis, stimulated by pulsatile GnRH and inhibited by inhibin and estrogen. Its two core actions - aromatase induction in granulosa cells (females) and Sertoli cell support (males) - make it indispensable for fertility. Clinically, FSH levels help distinguish between central (low FSH) and gonadal (high FSH) causes of reproductive failure, and recombinant FSH preparations are a cornerstone of modern assisted reproduction.
This is a shared conversation. Sign in to Orris to start your own chat.