Serological markers of hepatitis b
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
hepatitis B serological markers timeline HBsAg HBeAg antibodies
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
I now have comprehensive information. Let me compile the full answer.
Serological Markers of Hepatitis B
Hepatitis B virus (HBV) infection generates a characteristic sequence of antigens and antibodies in serum. Interpreting these markers allows you to determine the phase of infection, infectivity, immune status, and response to therapy.
The Key Markers at a Glance
| Marker | What it is | Clinical meaning |
|---|---|---|
| HBsAg | Surface antigen (envelope protein) | Active infection (acute or chronic) |
| Anti-HBs | Antibody to surface antigen | Immunity (resolved infection or vaccination) |
| HBcAg | Core antigen | Not detected in serum (intrahepatic only) |
| IgM Anti-HBc | IgM antibody to core antigen | Acute infection / window period marker |
| IgG Anti-HBc (Total Anti-HBc) | IgG antibody to core antigen | Past or ongoing infection |
| HBeAg | e antigen (precore protein) | Active viral replication, high infectivity |
| Anti-HBe | Antibody to e antigen | Reduced replication, seroconversion |
| HBV DNA | Viral genomic DNA (PCR) | Quantifies viral load; guides therapy |
Acute Hepatitis B — Serological Sequence
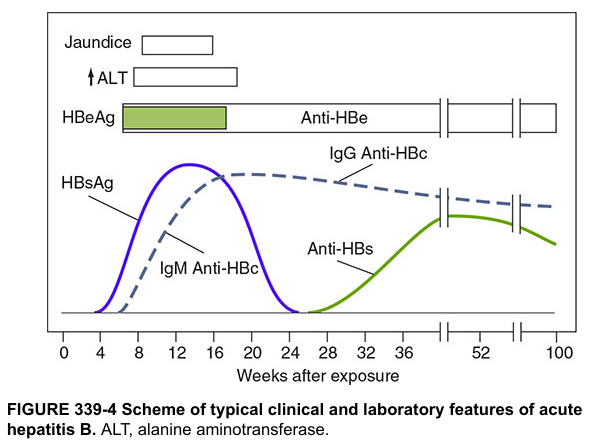
1. HBsAg appears in serum 2–10 weeks after exposure, before symptoms or ALT elevation. In self-limited infection it clears by 4–6 months. Persistence beyond 6 months = chronic infection. — Sleisenger & Fordtran's GI and Liver Disease, p. 1479
2. HBeAg appears early alongside HBsAg, indicating active replication and high infectivity. It disappears at or just after peak ALT. Persistence ≥3 months suggests progression to chronic infection.
3. IgM Anti-HBc rises with HBsAg, peaks around weeks 12–16, and persists for 4–6 months (rarely up to 2 years). This is the key marker of acute infection and the only marker detectable during the window period (when HBsAg has cleared but anti-HBs has not yet appeared). It can also re-emerge during exacerbations of chronic hepatitis B.
4. Anti-HBe appears as HBeAg clears — marking seroconversion to lower-replication state.
5. Anti-HBs appears weeks to months after HBsAg disappears. It indicates immunity and recovery. Persists for life in most patients. Also the marker produced by vaccination (anti-HBs positive, anti-HBc negative = vaccinated).
6. IgG Anti-HBc (Total Anti-HBc) replaces IgM anti-HBc and persists lifelong, indicating prior or ongoing infection.
The "Window Period"
The window period occurs between disappearance of HBsAg and appearance of anti-HBs. During this gap:
- HBsAg: negative
- Anti-HBs: negative
- IgM Anti-HBc: POSITIVE ← diagnostic key
Without testing for IgM anti-HBc, this phase can be missed entirely.
Chronic Hepatitis B — Serological Course
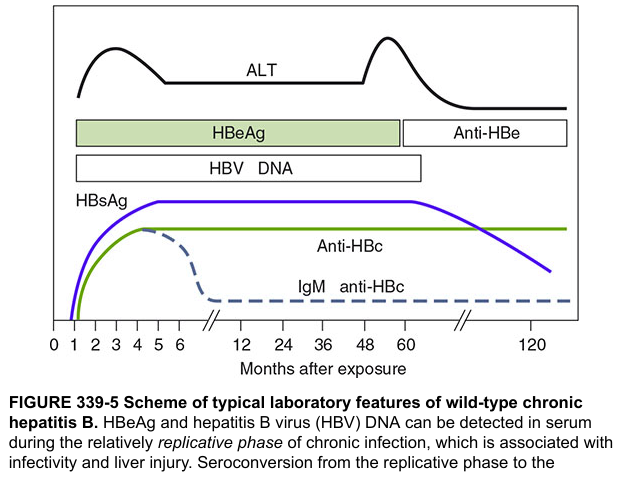
In chronic infection (HBsAg positive >6 months), two main phases are distinguished by HBeAg status:
| Phase | HBsAg | HBeAg | Anti-HBe | HBV DNA | ALT |
|---|---|---|---|---|---|
| Immune tolerant | + | + | − | Very high (up to 10¹²–¹³ IU/mL) | Normal |
| Immune active (HBeAg+) | + | + | − | High (≥20,000 IU/mL) | Elevated |
| Inactive carrier | + | − | + | Low/undetectable | Normal |
| HBeAg-negative chronic hepatitis | + | − | + | Detectable (fluctuating) | Elevated/fluctuating |
| Resolved infection | − | − | ± | Undetectable | Normal |
HBeAg seroconversion (HBeAg → Anti-HBe) signals a shift from high to low replication, but does not mean eradication — HBsAg remains positive.
Isolated Anti-HBc — Interpretations
When only anti-HBc is positive (HBsAg and anti-HBs both negative), possible interpretations include:
| Interpretation | Key Features |
|---|---|
| Resolved/remote infection | Common in endemic areas; HBV DNA undetectable |
| Window period of acute HBV | IgM anti-HBc positive; HBV DNA also detectable |
| False-positive | Weakly reactive; repeat in 3–6 months |
| Occult HBV infection | Rare; HBV DNA detectable at low levels |
— Sleisenger & Fordtran's GI and Liver Disease, Table 79.3, p. 1479
HBV DNA
Quantitative HBV DNA (real-time PCR; sensitivity 5–10 IU/mL) is essential for:
- Establishing indication for antiviral therapy
- Monitoring treatment response
- Detecting drug resistance (HBeAg-negative patients with rising DNA on therapy)
HBsAg quantification (licensed in many countries): HBsAg < 1000 IU/mL in anti-HBe-positive patients distinguishes true inactive carriage from relapsing disease. — Sleisenger & Fordtran's, p. 1480
Summary: Common Patterns
| HBsAg | Anti-HBs | IgM Anti-HBc | Total Anti-HBc | HBeAg | Interpretation |
|---|---|---|---|---|---|
| + | − | + | + | + | Acute HBV infection |
| − | − | + | + | − | Window period |
| − | + | − | + | − | Resolved past infection |
| − | + | − | − | − | Vaccination (immune) |
| + | − | − | + | + | Chronic HBV, replicative |
| + | − | − | + | − | Chronic HBV, low replication / inactive carrier |
| − | − | − | + | − | Isolated anti-HBc (see table above) |
Sources:
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, pp. 1479–1480
- Harrison's Principles of Internal Medicine, 21st ed., Figs. 339-4 & 339-5
- Medical Microbiology, 9th ed., Chapter 55
Ascites
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.