Explain diabetes
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetes mellitus"[MeSH Terms] AND "pathophysiology"[MeSH Terms]
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-cited answer. Let me compile it.
Diabetes Mellitus - A Complete Overview
What Is Diabetes?
Diabetes mellitus (DM) is a group of metabolic diseases characterized by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both. Without insulin to facilitate glucose uptake into cells, glucose accumulates in the blood, causing short- and long-term damage to virtually every organ system.
Classification (4 Types)
Per the American Diabetes Association (ADA), there are four clinical categories:
| Type | Mechanism |
|---|---|
| Type 1 DM (T1DM) | Autoimmune destruction of pancreatic beta cells → absolute insulin deficiency |
| Type 2 DM (T2DM) | Progressive beta-cell secretory failure, usually on a background of insulin resistance |
| Gestational DM (GDM) | Diabetes first diagnosed during pregnancy, not clearly overt beforehand |
| Other specific types | Monogenic syndromes (MODY, neonatal diabetes), exocrine pancreatic disease (e.g., cystic fibrosis), drug-induced (glucocorticoids, HIV treatment, post-transplant) |
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1466
Type 1 Diabetes Mellitus
Epidemiology & Presentation
T1DM accounts for 5-10% of all diabetes cases. Mean age of onset is the early teenage years, but it can appear from infancy to the fourth decade. Classic presentation is in a lean patient with:
- Polyuria (excess urination)
- Polydipsia (excess thirst)
- Polyphagia (excess hunger)
- Weight loss and fatigue
Pathophysiology
T1DM is a chronic autoimmune disease driven by destruction of beta cells in the islets of Langerhans. Key features:
-
Markers of autoimmunity include islet cell autoantibodies, anti-insulin antibodies, anti-GAD65 antibodies, and anti-IA-2 antibodies
-
Genetic susceptibility is multigenic - HLA region genes (especially those encoding antigen-presenting molecules) carry the greatest risk
-
Concordance in identical twins is less than 100%, meaning environmental triggers also play a role - enteroviruses are strongly suspected
-
In genetically at-risk individuals who develop 2+ diabetes-related autoantibodies, the risk of progression to T1DM is 75% over 10 years and approaches certainty over 20 years
-
A brief "honeymoon period" may occur after diagnosis, but exogenous insulin is always ultimately required
-
Mulholland & Greenfield's Surgery, p. 2031-2039
Type 2 Diabetes Mellitus
Epidemiology
T2DM is far more common, accounting for ~90-95% of all cases. Onset is typically after age 30 (classically 50-60 years), but rising obesity has driven a steady increase in T2DM among younger people, including children.
Pathophysiology
The mechanism is more complex than simple insulin deficiency:
- Insulin resistance develops first - peripheral tissues (muscle, liver, fat) become insensitive to insulin. The pancreas compensates by secreting more insulin (hyperinsulinemia).
- Beta-cell exhaustion - Over time, beta cells cannot keep up with demand. This is driven by:
- Glucotoxicity (chronic hyperglycemia damages beta cells)
- Lipotoxicity (fatty acids, lipoproteins, cytokines promote apoptosis)
- Oxidative and endoplasmic reticulum stress
- Beta-cell dedifferentiation - stressed beta cells lose beta-cell-specific gene expression and may begin secreting non-beta-cell hormones (glucagon, somatostatin)
- Progressive beta-cell mass loss ensues, worsening hyperglycemia
T2DM is associated with obesity, visceral fat accumulation, and the metabolic syndrome (hypertension, dyslipidemia, central obesity, hyperglycemia). Many patients have irreversible complications at the time of diagnosis due to the insidious onset.
- Guyton & Hall Textbook of Medical Physiology, p. 3002-3024
- Tietz Textbook of Laboratory Medicine 7e, p. 3282
Diagnosis
| Test | Normal | Prediabetes | Diabetes |
|---|---|---|---|
| Fasting Plasma Glucose (FPG) | <100 mg/dL | 100-125 mg/dL (IFG) | ≥126 mg/dL |
| 2-hr OGTT Glucose | <140 mg/dL | 140-199 mg/dL (IGT) | ≥200 mg/dL |
| HbA1c | <5.7% | 5.7-6.4% | ≥6.5% |
| Random glucose + symptoms | - | - | ≥200 mg/dL |
Abnormal tests should be repeated on a separate visit to confirm the diagnosis (unless two different tests are both abnormal simultaneously).
- Quick Compendium of Clinical Pathology 5e, p. 2415-2426
Classic Symptoms of Hyperglycemia
When blood glucose is persistently elevated, the hallmark symptoms are:
- 3 Ps: Polyuria, Polydipsia, Polyphagia
- Unexplained weight loss (increased protein/fat catabolism)
- Fatigue and blurred vision
Severe uncontrolled diabetes leads to:
- Diabetic ketoacidosis (DKA) - mainly T1DM; ketone bodies accumulate from fat metabolism, dropping blood pH to <7.0, causing coma and death
- Hyperosmolar hyperglycemic state (HHS) - mainly T2DM; extreme hyperglycemia without significant ketosis
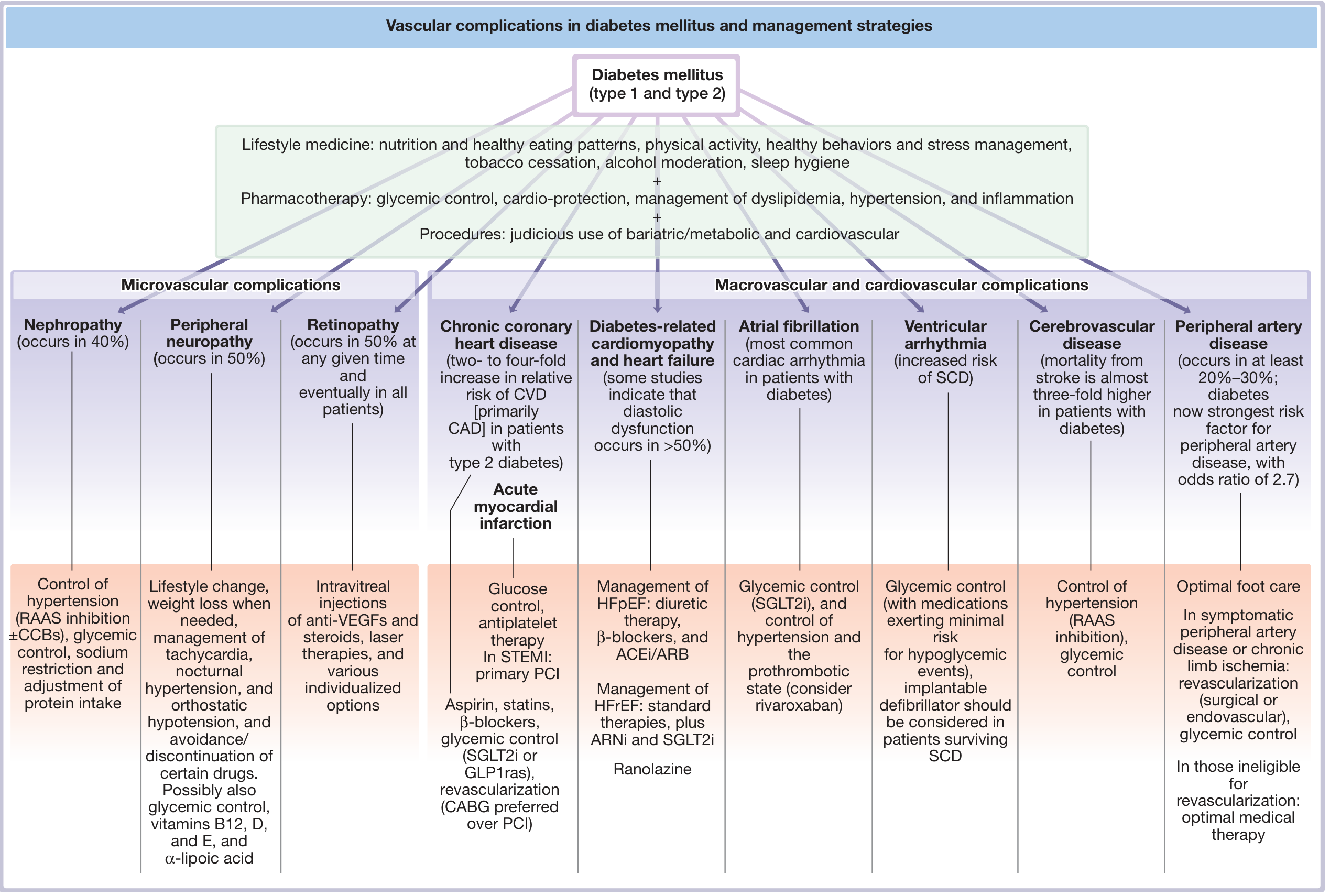
Complications
The chronic complications of diabetes are among the most clinically significant. They are divided into vascular and non-vascular.
- Fuster & Hurst's The Heart, 15th Edition
Microvascular Complications (diabetes-specific)
| Complication | Detail |
|---|---|
| Diabetic retinopathy | Occurs in ~50% at any given time, eventually in ALL long-standing patients. Leading cause of blindness. |
| Diabetic nephropathy | Occurs in ~40%. Responsible for nearly 40% of all end-stage renal disease (ESRD) cases. |
| Diabetic neuropathy | Occurs in ~50%. Peripheral, autonomic, and focal forms. Leading cause of non-traumatic lower-limb amputations. |
Mechanism: Chronic hyperglycemia drives excess glucose through the polyol pathway (aldose reductase) → sorbitol accumulation → reduced myoinositol → impaired Na+/K+ ATPase activity and advanced glycation end-products (AGEs) that damage nerves and vessel walls.
Macrovascular Complications (shared with general population but accelerated)
- Atherosclerotic cardiovascular disease (ASCVD) - 2-4x greater risk of MI; chronic coronary disease risk doubled to quadrupled
- Peripheral artery disease (PAD) - at least 20-30% occurrence; DM is now the strongest risk factor for PAD (OR 2.7)
- Cerebrovascular disease - stroke mortality nearly 3x higher
- Heart failure - diabetic cardiomyopathy; diastolic dysfunction in >50%
ASCVD events correlate with both fasting glucose levels and HbA1c. The landmark DCCT trial proved that intensive glycemic control (HbA1c 7.3% vs 9.1%) prevented microvascular complications in T1DM. A "metabolic memory" (legacy effect) of early tight control persists for decades.
- Harrison's Principles of Internal Medicine 22e (2025), p. 1518-1534
- Mulholland & Greenfield's Surgery 7e, p. 2062
Treatment Overview
Type 1 DM
- Requires exogenous insulin - always, lifelong
- Basal-bolus regimen: long-acting insulin once/twice daily + short-acting at mealtimes
- Insulin pump therapy is an alternative
- Goal HbA1c: <7% for most patients
Type 2 DM - Stepwise Approach
- Lifestyle modification - dietary change, physical activity, weight loss (cornerstone)
- Metformin (first-line pharmacotherapy) - reduces hepatic glucose output, improves insulin sensitivity; also has cardiovascular and weight benefits; approved down to age 10
- Additional agents added when metformin is insufficient:
- SGLT2 inhibitors (empagliflozin, dapagliflozin) - especially with heart failure or CKD
- GLP-1 receptor agonists (semaglutide, liraglutide) - especially with obesity or ASCVD
- DPP-4 inhibitors, sulfonylureas, thiazolidinediones
- Insulin is added if oral agents fail to achieve targets
Monitoring: HbA1c at least twice yearly (target <7%), annual lipids, annual microalbuminuria + eGFR, annual dilated eye exam, foot exams.
- Lippincott Illustrated Reviews: Pharmacology, p. 991-1170
- Brenner & Rector's The Kidney, p. 3815
Key Numbers to Remember
| Parameter | Target |
|---|---|
| HbA1c | <7% (most adults) |
| Blood pressure | <130/80 mmHg |
| LDL cholesterol | <70 mg/dL (high-risk) |
| Fasting glucose | 80-130 mg/dL |
| Post-meal glucose | <180 mg/dL |
Summary
Diabetes is not a single disease but a spectrum of conditions unified by hyperglycemia. T1DM is autoimmune and requires insulin from the start. T2DM is driven by insulin resistance and beta-cell failure, is strongly tied to obesity and lifestyle, and is managed progressively from diet to oral medications to insulin. Both types, if poorly controlled, cause devastating microvascular (retinopathy, nephropathy, neuropathy) and macrovascular (heart attack, stroke, PAD) complications. The evidence is clear: tight glycemic control from early in the disease course dramatically reduces complication risk and preserves quality of life.
This is a shared conversation. Sign in to Orris to start your own chat.