Abdominal tuberculosis
Reading File
Finding Sources
Searching PubMed
"abdominal tuberculosis" diagnosis treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information to write a thorough, well-sourced answer. Let me compile everything.
Abdominal Tuberculosis
Abdominal tuberculosis (TB) is the commonest form of extrapulmonary TB, accounting for approximately 11% of extrapulmonary cases. It encompasses involvement of the gastrointestinal tract, peritoneum, and mesenteric lymph nodes. Its incidence is rising in resource-rich countries due to migration and immunosuppression (HIV, anti-TNF agents, glucocorticoids).
Causative Organisms and Pathogenesis
- Mycobacterium tuberculosis - responsible for the vast majority of cases
- Mycobacterium bovis - via contaminated dairy products (uncommon in Western countries)
- M. avium intracellulare - increasing with HIV co-infection
Routes of infection:
- Swallowing of infected sputum (direct mucosal penetration) - the classic route
- Ingestion of contaminated milk/food
- Hematogenous (miliary) spread
- Direct extension from adjacent organs (e.g., renal TB, fallopian tube TB in women)
Classification
Abdominal TB is divided into two broad categories:
A. Intestinal Tuberculosis
The ileocaecal region (terminal ileum + caecum) is involved in 75% of cases. Both sides of the ileocaecal valve are usually affected, causing valve incompetence - a key distinguishing feature from Crohn disease.
Three gross morphological types:
| Type | Frequency | Features |
|---|---|---|
| Ulcerative | 60% | Multiple superficial transverse ulcers; confined to epithelial surface; long axis lies transversely |
| Hypertrophic | 10% | Scarring, fibrosis, heaped-up mass lesions; can mimic carcinoma |
| Ulcerohypertrophic | 30% | Combined ulceration + scar formation |
Healing of ulcers leads to fibrosis and stricture formation.
B. Tuberculosis of Mesenteric Lymph Nodes
Rare; mainly seen in children. Bacilli (both human and bovine type) enter through Peyer's patches. Can present as:
- Chronic central abdominal pain/discomfort (enlarged nodes palpable to the right of the umbilicus)
- General symptoms: weight loss, anorexia, evening pyrexia
- Intestinal obstruction (loop adherent to caseating node)
- Mimicry of appendicitis (RIF pain, but Rovsing's sign negative, no high WBC/pulse)
- Pseudomesenteric cyst (cold abscess between mesenteric leaves after caseation)
- Calcified lymph nodes on plain X-ray
C. Tuberculous Peritonitis
50-80% of patients with abdominal TB have peritoneal involvement. Peritoneal spread occurs via mesenteric lymph nodes, contiguous spread from gut or genital TB, or hematogenous seeding.
Three forms of peritoneal TB:
- Wet ascitic type (90%) - generalised or loculated exudative ascites; multiple tubercle deposits on both peritoneal layers
- Dry/plastic type - fibrotic fixed loops with matted bowel and omentum; no ascites; presents with subacute intestinal obstruction
- Mixed form
Clinical Features
The presentation can be acute, chronic, or acute-on-chronic. TB is "the great masquerader" and can mimic almost any GI disease.
Symptoms:
- Chronic non-specific abdominal pain: 80-90% of patients
- Weight loss, fever (evening rise), night sweats
- Diarrhoea or constipation
- Blood in stool (occult bleeding more than frank haematochezia)
- Abdominal distension (ascites)
Signs:
- Palpable RLQ mass in 25-50% (ileocaecal involvement)
- Perianal fistulae (should prompt evaluation for rectal TB)
- Enlarged, firm, discrete lymph nodes in the umbilical region (in mesenteric node disease)
Complications: Intestinal obstruction (most common), perforation, haemorrhage, fistula formation, malabsorption (from SIBO secondary to obstruction).
Note: Chest film is often normal at the time of intestinal TB diagnosis - active concurrent pulmonary disease is now uncommon.
Histopathology
The hallmark lesion is the caseating granuloma - found in 50-80% of intestinal TB biopsies.
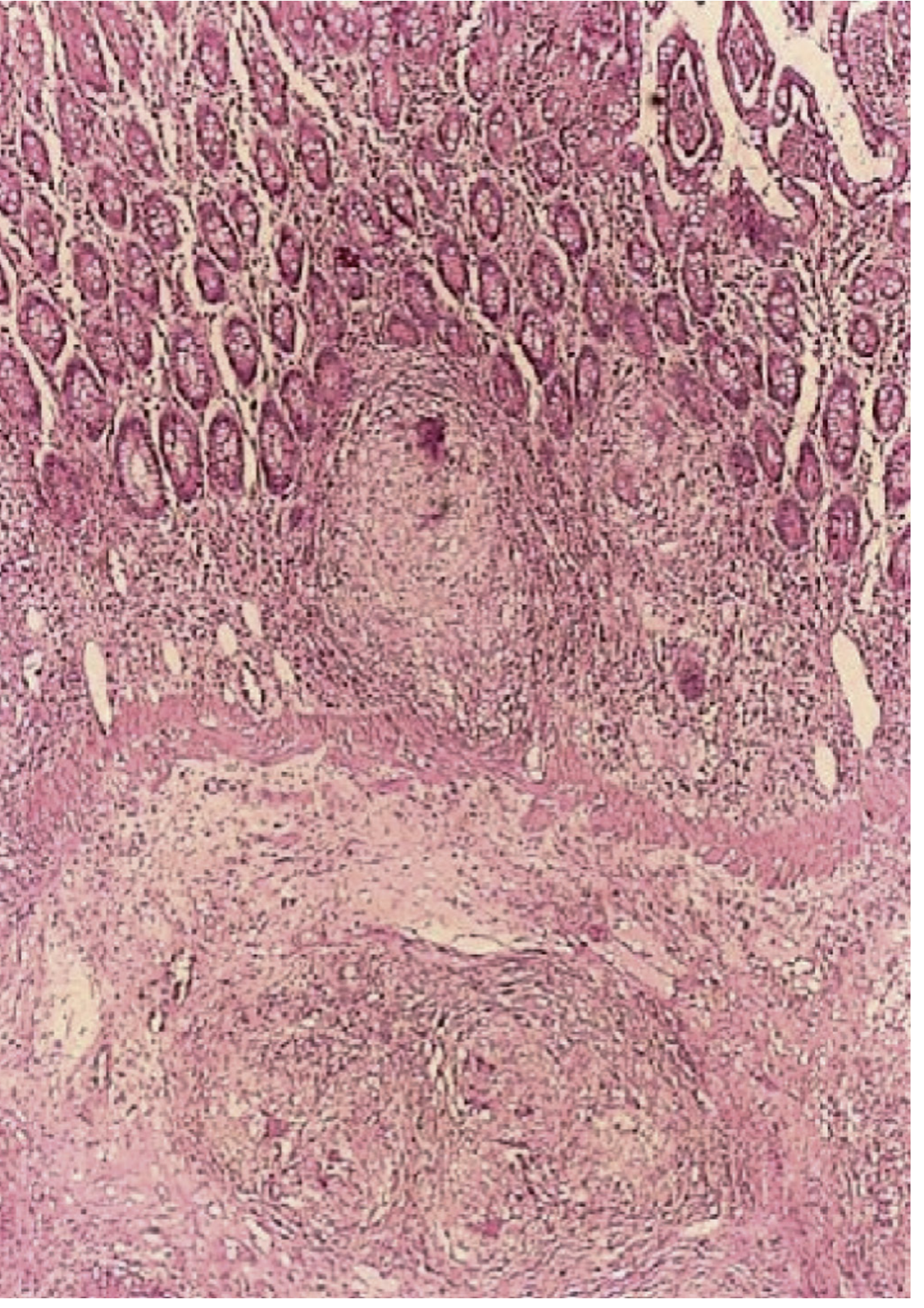
Photomicrograph of a colon biopsy showing granulomas in mucosa and submucosa in a patient with intestinal TB (H&E). - Sleisenger & Fordtran's Gastrointestinal and Liver Disease
- AFB detected on acid-fast stain in ~20% of mucosal samples
- PCR (Xpert MTB/RIF): ~65% sensitivity, faster than culture
Investigations
Laboratory
- Raised inflammatory markers (ESR, CRP), mild anaemia, normal or mildly elevated WBC
- Mantoux / IGRA (IFN-γ release assay): positive does not confirm active disease; negative does not exclude it (especially in HIV or elderly)
- QuantiFERON-Gold: poor test characteristics for active peritoneal TB, particularly in BCG-vaccinated endemic populations
Ascitic Fluid Analysis (for peritoneal TB)
- Straw-coloured exudate
- Protein >25-30 g/L; low serum-ascites albumin gradient (<1.1 g/dL)
- WBC >500/mL with lymphocytic predominance (>40%)
- Adenosine deaminase (ADA): high sensitivity and specificity (cut-off ~30 U/L); distinguishes tuberculous from carcinomatous ascites
- Smear positivity is low; culture takes 4-8 weeks
Imaging
- Chest X-ray: pulmonary infiltration (may be normal)
- Abdominal ultrasound: loculated ascites, lymphadenopathy
- CT abdomen: thickened ileocaecal valve, asymmetric bowel wall thickening, massive lymphadenopathy with central/hypodense necrosis, peritoneal/omental thickening. Contracted caecum with disease on both sides of the valve.
- Barium meal and follow-through: non-filling of terminal ileum/caecum (due to narrowing and hypermotility); Stierlin sign - conification/narrowing of the caecum and loss of haustrations; subhepatic pull-up of caecum; multiple ileal strictures.
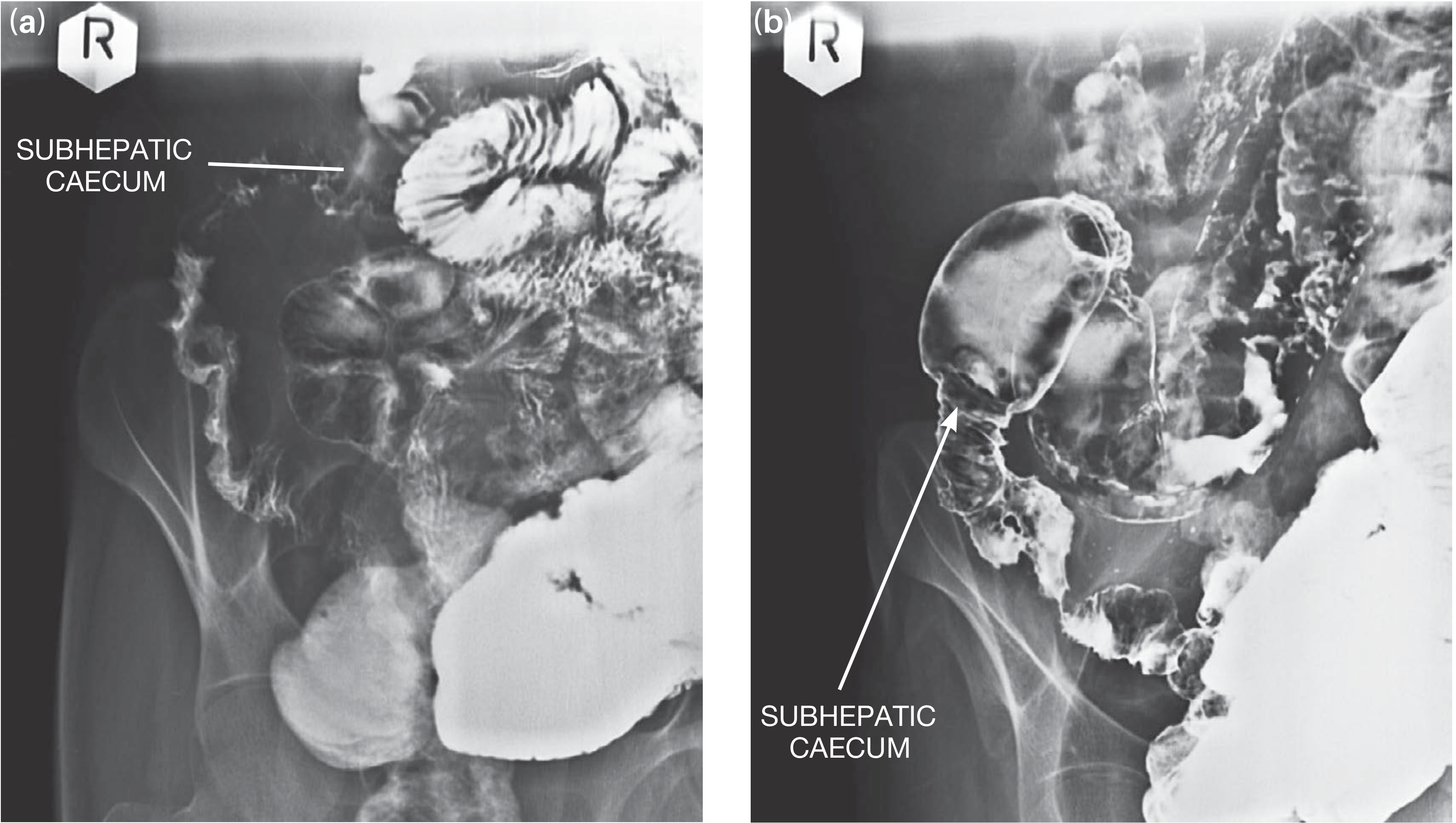
Barium series showing ileal strictures with subhepatic caecum in intestinal TB. - Bailey and Love's Short Practice of Surgery
Endoscopy
- Colonoscopy with biopsy is the most useful diagnostic procedure
- Isolation precautions (mask) are required in the endoscopy suite
- Specimens for histopathology, AFB stain/PCR, and culture with drug sensitivities
- Endoscopic appearances: transverse ulcers, patulous (gaping) ileocaecal valve, pseudopolyps, scarring - contrast with Crohn's longitudinal ulcers, cobblestoning, and aphthous ulcers
Laparoscopy
- Near 100% sensitivity for peritoneal TB (lymphocytic ascites with fever = TB until proven otherwise)
- Typical appearance: "millet seed" peritoneal tubercles; peritoneal biopsy confirms caseating granulomas
Differential Diagnosis
| Condition | Distinguishing Points |
|---|---|
| Crohn disease | Linear/longitudinal ulcers, non-caseating granulomas (<400 µm), ileocaecal valve competent, no AFB |
| Colonic carcinoma | Hypertrophic TB can mimic; biopsy differentiates |
| Appendicitis | Mesenteric TB: no Rovsing's sign, normal leucocyte count/pulse rate |
| Peritoneal carcinomatosis | TB peritonitis: lymphocytic ascites with fever; elevated ADA; peritoneal biopsy |
| Ovarian carcinoma | TB can cause pelvic mass with elevated CA-125 |
| Yersiniosis, Histoplasmosis, Actinomycosis, Amoebiasis | Microbiological/histological differentiation |
Treatment
Medical (First-Line Anti-TB Therapy)
Standard 6-month regimen (HRZE/HR):
- Phase 1 (Intensive, 2 months): Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) - 4 drugs
- Phase 2 (Continuation, 4 months): Isoniazid + Rifampicin - 2 drugs
Notes:
- Ethambutol may be stopped once susceptibility to all drugs is confirmed
- Pyridoxine (vitamin B6) supplementation is co-prescribed to prevent isoniazid-induced peripheral neuropathy
- Patients at higher risk of relapse may be treated for up to 9 months
- Global treatment success rate: ~85%
- Hepatotoxicity of first-line drugs is a concern in cirrhotic patients with TB peritonitis
- TB is a reportable disease; public health notification is mandatory
Drug-resistant TB:
- MDR-TB (resistant to H + R): ~3.4% of new cases
- XDR-TB: MDR + resistance to fluoroquinolones + injectable agents
- Second-line agents: bedaquiline, levofloxacin/moxifloxacin, clofazimine, cycloserine, delamanid, linezolid
- Treatment duration: 9-20 months depending on resistance pattern
Surgical Management
Surgery is not the primary treatment and is reserved for complications:
Elective surgery:
- Subacute intermittent obstruction not resolving on anti-TB drugs:
- Limited ileocolic resection with anastomosis (terminal ileum to ascending colon) for ileocolic hyperplastic disease
- Strictureplasty for short single ileal strictures
- Right hemicolectomy for extensive ileocolic disease
Emergency surgery (acute obstruction/perforation):
- Vigorous resuscitation first (correct dehydration, anaemia, malnutrition)
- Minimum life-saving procedure: resection of diseased segment + proximal ileostomy + distal mucus fistula (anastomosis avoided due to high leak risk in active infection and poor general condition)
- One-stage resection and anastomosis only if patient general condition permits
Post-surgery, the patient requires full multidrug anti-TB chemotherapy (6-12 months) under combined physician and surgical care, with reassessment of bowel once disease is no longer active (normal inflammatory markers, weight gain, negative culture).
Perforation: Resection of affected segment; anastomosis if condition allows.
Prognosis
- Prognosis depends primarily on immune status and promptness of therapy
- In untreated HIV-infected patients, disease progresses rapidly and is often fatal
- With appropriate early treatment, results are generally satisfactory even in immunocompromised patients
- Clinical response to anti-TB therapy often occurs within 2 weeks, though hypertrophic/mass lesions and strictures respond more slowly
- Intestinal obstruction may resolve with anti-TB treatment alone without surgery
Key Points Summary
| Feature | Detail |
|---|---|
| Commonest site | Terminal ileum + caecum (75%) |
| Gross types | Ulcerative (60%), Hypertrophic (10%), Ulcerohypertrophic (30%) |
| Diagnostic hallmark | Caseating granuloma on biopsy |
| Best diagnostic procedure | Colonoscopy with biopsy (histology + AFB stain + PCR + culture) |
| Stierlin sign | Conification of caecum on barium enema (characteristic of TB) |
| Ascitic ADA | High sensitivity/specificity for peritoneal TB |
| Treatment | 2HRZE / 4HR (6 months standard) |
| Surgery | Only for complications - obstruction, perforation, fistula, unresolved mass |
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Yamada's Textbook of Gastroenterology (7e); Bailey and Love's Short Practice of Surgery (28e); S Das Manual on Clinical Surgery (13e); Harrison's Principles of Internal Medicine (22e); Murray & Nadel's Textbook of Respiratory Medicine.
Recent evidence: A 2025 systematic review on abdominal TB in children (PMID: 40533676) highlights current advances in pediatric diagnosis and management - no major changes to the standard regimen were noted.
This is a shared conversation. Sign in to Orris to start your own chat.