What is lateral subluxation of patella? Whats it's cause and what happens in this condition?
Reading File
Finding Sources
Finding Sources
Searching the Web
lateral subluxation of patella causes pathology mechanism
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Lateral Subluxation of the Patella
Definition
Lateral subluxation of the patella is a condition in which the patella (kneecap) partially slides out of its normal position within the femoral trochlear groove toward the lateral (outer) side, without completely dislocating. It exists on a spectrum — from subtle lateral maltracking all the way to frank complete dislocation. Unlike a full dislocation, in subluxation the patella momentarily shifts laterally and may spontaneously reduce.
Normal Anatomy (What Keeps the Patella in Place)
The patella sits in the trochlear groove of the femur and is held in place by:
- Medial restraints: primarily the medial patellofemoral ligament (MPFL), which is the primary passive stabilizer (~50–60% of restraining force) against lateral displacement
- Lateral restraints: lateral retinaculum and iliotibial band
- Dynamic stabilizer: the vastus medialis oblique (VMO) muscle, which pulls the patella medially
- Bony constraint: the depth and shape of the trochlear groove
Causes (Etiology)
Lateral subluxation is multifactorial. Any condition that shifts the balance of forces laterally can cause it:
1. Increased Q Angle
The Q angle (quadriceps angle) is the angle between the line from the ASIS to the center of the patella and the line from the patella to the tibial tubercle. An increased Q angle (>15° in men, >20° in women) creates a resultant lateral pull force on the patella. This is why:
- Females have a 50–100% greater incidence than males (wider pelvis → larger Q angle)
- Genu valgum (knock knees) increases Q angle
- Femoral anteversion and pronated feet also exacerbate this
2. Trochlear Dysplasia
A shallow or abnormally shaped trochlear groove provides less bony constraint, reducing resistance to lateral patellar shift. Classified by the Dejour system (Types A–D). On lateral X-ray, a crossing sign (trochlear groove line intersecting the anterior femoral condyle) or a supratrochlear spur indicates dysplasia.
3. MPFL Injury/Insufficiency
The MPFL is the primary medial restraint. Traumatic rupture (commonly at its patellar insertion) allows unrestricted lateral movement. A history of dislocation frequently causes MPFL damage, setting up recurrent instability.
4. Patella Alta
A high-riding patella engages the trochlear groove later during knee flexion and sits above the deep constraining part of the trochlea in early flexion, making it more vulnerable to lateral subluxation.
5. VMO Weakness / Muscular Imbalance
The VMO is the only dynamic medial stabilizer. Weakness allows the relatively stronger vastus lateralis and lateral retinaculum to pull the patella laterally.
6. Tight Lateral Retinaculum
Tightness of the lateral retinaculum can cause excessive lateral patellar tilt and subluxation even in the absence of instability per se.
7. "Miserable Malalignment Syndrome"
A combination of femoral anteversion + genu valgum + pronated feet in adolescents significantly worsens symptoms and lateral pull.
8. Increased TT-TG Distance
The tibial tubercle–trochlear groove (TT-TG) distance measures the offset between the tibial tubercle and trochlear groove on CT. A distance >20 mm is strongly associated with patellar instability and lateral subluxation.
What Happens in This Condition (Pathophysiology & Consequences)
Biomechanical Changes
- The patella tracks abnormally on the lateral femoral condyle instead of centered in the groove
- The resultant force vector of the quadriceps pulls the patella laterally (especially with the knee near extension)
- The "J sign" may be observed clinically — an inverted-J trajectory of the patella as the knee moves from flexion to extension, with sudden lateral jump of the patella near terminal extension
Structural Damage
- MPFL disruption: With acute subluxation/dislocation events, the MPFL tears — most commonly at its patellar insertion
- Osteochondral injury: The medial facet of the patella impacts the lateral femoral condyle during lateral shift or during spontaneous reduction, causing:
- Bone bruise (medial patella + lateral femoral condyle)
- Osteochondral fractures — fragments can shear off the lateral femoral condyle or medial patellar facet, forming loose bodies
- Articular cartilage damage: The medial patellar facet articular surface is most commonly injured during reduction of the patella
- Hemarthrosis: A frequent result of first-time dislocation/subluxation due to tearing of the medial retinaculum and associated vasculature
Clinical Features
- Anterior knee pain and a feeling of the knee "giving way"
- Patellar apprehension test: Patient experiences pain and apprehension (sensation of impending dislocation) when the examiner pushes the patella laterally
- Lateral patellar glide: Abnormal mobility (3–4 quadrants of lateral glide)
- J sign on dynamic examination
- Swelling/effusion if there is acute injury
Long-term Consequences
- Recurrence: After a first-time dislocation, recurrence is 15–60%; higher risk with younger age, female sex, patella alta, and trochlear dysplasia
- Patellofemoral arthritis: Chronic malalignment and repeated cartilage trauma leads to premature degenerative joint disease
- Chondromalacia patellae: Softening and fibrillation of the patellar cartilage from abnormal contact stresses
Key Imaging Measurements
Sulcus and congruence angles (axial X-ray):
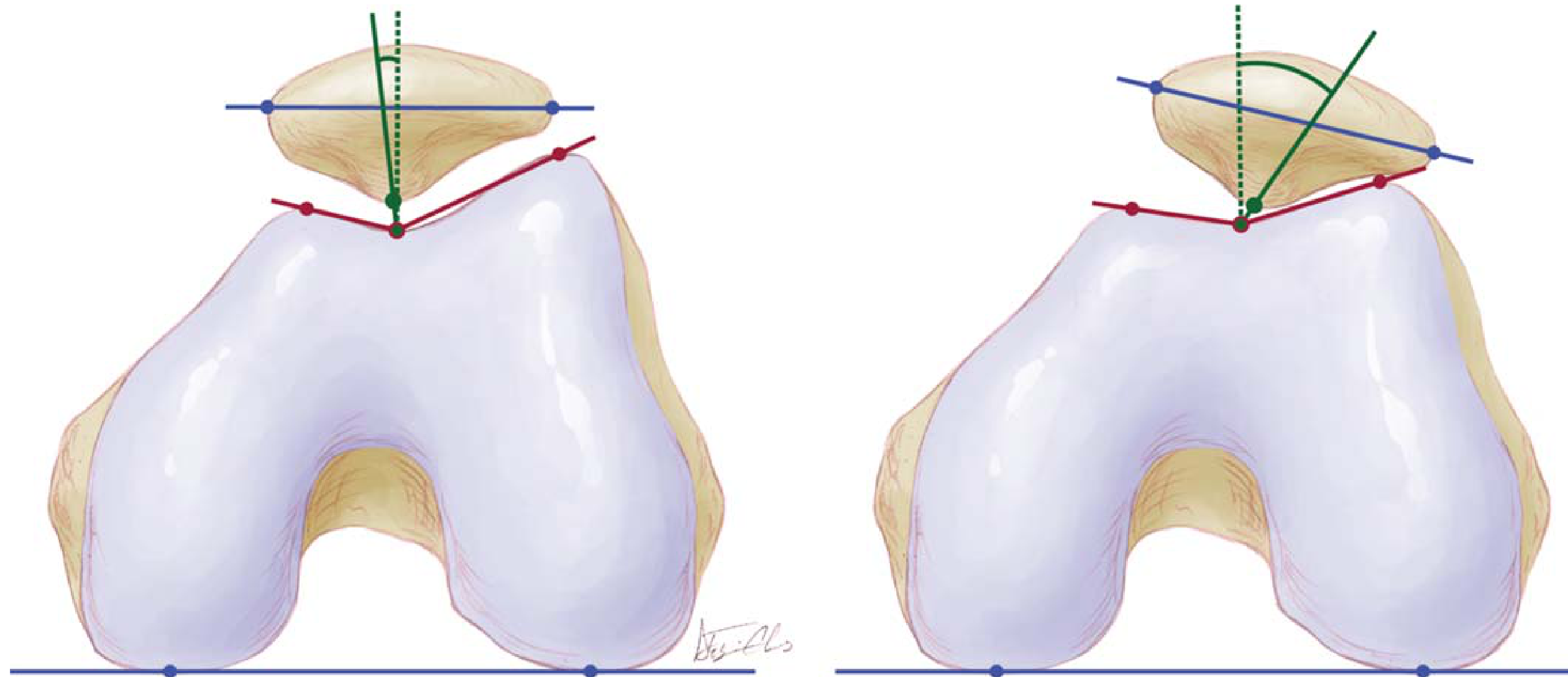
- Sulcus angle: Normally ~138°; ≥150° = abnormally shallow groove
- Congruence angle: Normally −6°; >+16° = abnormal patellofemoral articulation (lateral subluxation)
TT-TG distance (CT measurement):
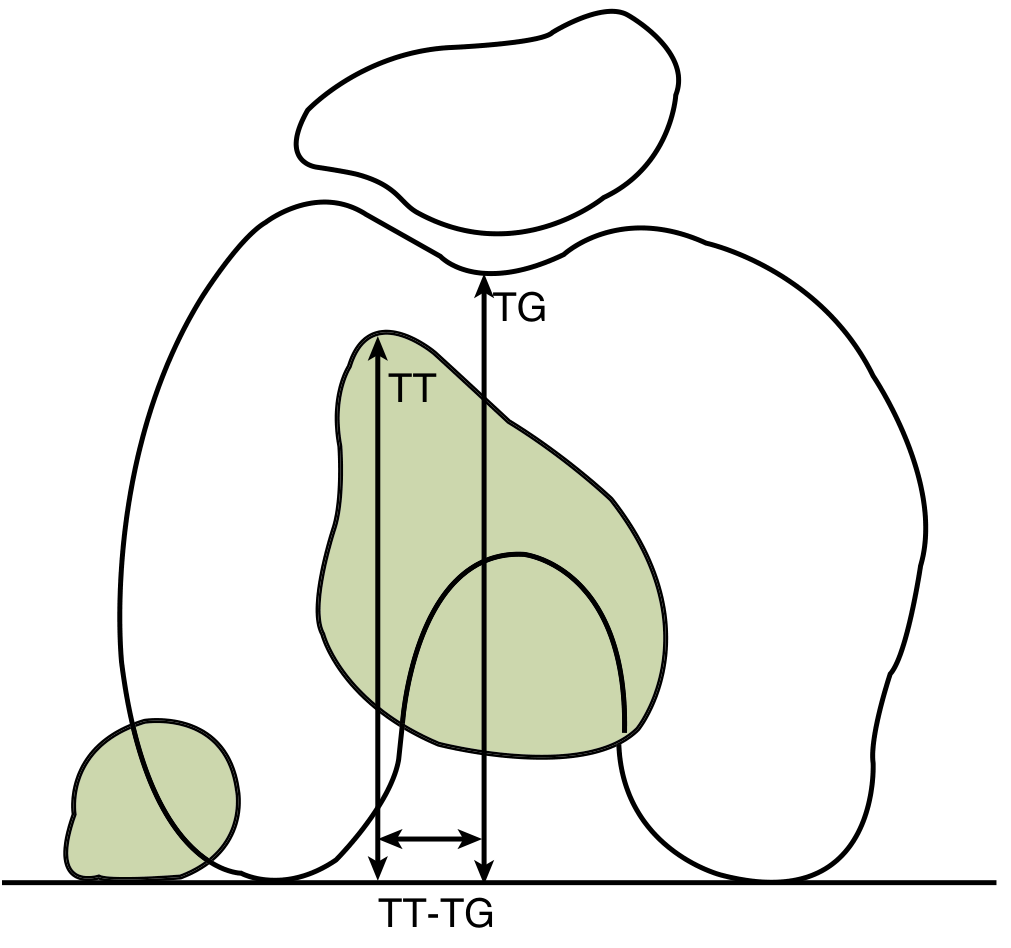
- TT-TG >20 mm is strongly correlated with patellar instability
Summary Table
| Factor | How It Causes Lateral Subluxation |
|---|---|
| Increased Q angle | Increases lateral vector on patella |
| Trochlear dysplasia | Less bony constraint to lateral shift |
| MPFL rupture/insufficiency | Loss of primary medial restraint |
| Patella alta | Late trochlear engagement, poor early stabilization |
| VMO weakness | Loss of dynamic medial pull |
| Tight lateral retinaculum | Actively pulls patella laterally |
| Increased TT-TG >20 mm | Tibial tubercle lateralized, worsens vector |
Sources: Miller's Review of Orthopaedics 9th Edition (pp. 364–367); Tintinalli's Emergency Medicine; Rockwood and Green's Fractures in Adults 10th Ed
This is a shared conversation. Sign in to Orris to start your own chat.