60 year old hypertensive male has presented with weakness and inability to move hisright upper and lower extremities since last 2 hours. After admission in nearby hospital,clinical examination revealed increased muscle tone, exaggerated tendon jerks and extensorplantar response on his right side.i) What can be the probable diagnosis?ii) Explain the reason behind the increased muscle tone and exaggerated tendon jerks in thispatient.ⅲ) Why the planter response is altered here?iv) Describe the corticospinal tract with a suitable diagram
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content and excellent diagrams. Let me compose the full answer.
Clinical Case Analysis: 60-year-old Hypertensive Male with Right-sided Weakness
i) Probable Diagnosis
Left-sided Ischemic Stroke (Middle Cerebral Artery territory infarct) - specifically, an upper motor neuron (UMN) lesion involving the left corticospinal tract, most likely at the level of the left internal capsule or left cerebral cortex/subcortical white matter.
Reasoning:
- A 60-year-old hypertensive male is at high cardiovascular risk for ischemic stroke.
- The onset is acute (2 hours), which is characteristic of a vascular event.
- Weakness of the right upper and lower extremities = right-sided hemiplegia, pointing to a lesion in the contralateral (left) hemisphere or left corticospinal tract (since fibers cross at the pyramidal decussation in the medulla).
- The triad of increased muscle tone (spasticity) + exaggerated tendon jerks (hyperreflexia) + extensor plantar response is the classic UMN syndrome.
- Hypertension is the single most important modifiable risk factor for stroke.
ii) Increased Muscle Tone and Exaggerated Tendon Jerks: Mechanism
These signs arise due to loss of the descending inhibitory influence that the corticospinal (and corticoreticulospinal) tract normally exerts on the spinal stretch reflex arc.
Normal physiology
The upper motor neurons continuously send inhibitory signals (via interneurons) that modulate the excitability of both:
- Alpha (α) motor neurons - which directly contract extrafusal muscle fibers
- Gamma (γ) motor neurons - which set the sensitivity of the muscle spindle (intrafusal fibers)
The corticospinal tract (particularly via the corticoreticulospinal pathway) also tonically inhibits the vestibulospinal and reticulospinal tracts that facilitate muscle tone.
After UMN lesion
When the corticospinal/corticoreticular fibers are damaged by the stroke:
- Loss of descending inhibition removes the braking effect on α and γ motor neurons in the spinal cord.
- γ motor neurons become hyperactive - they increase the tension of muscle spindles, making spindle afferents (Ia fibers) hypersensitive to stretch.
- Even a small stretch of the muscle now fires a volley of Ia afferent impulses that cause an exaggerated reflex contraction via the monosynaptic stretch reflex arc.
- This produces spasticity (velocity-dependent increase in muscle tone) and hyperreflexia (exaggerated tendon jerks).
As Adams and Victor's Principles of Neurology explains: "Lesions of the premotor cortex (area 6) result in weakness, spasticity, and increased stretch reflexes... the corticoreticulospinal pathways, whose fibers are arranged somatotopically and influence stretch reflexes, are particularly important in the genesis of spasticity."
Harrison's Principles of Internal Medicine further notes: "Spasticity is typical but may not be present acutely" - meaning in this patient at 2 hours, signs may be emerging as the initial spinal shock resolves.
Note: In the very acute phase (minutes to hours after a hemispheric stroke), the affected limbs may initially be flaccid due to "cerebral shock" / diaschisis. The spasticity and hyperreflexia typically develop over days to weeks as the spinal cord recovers its intrinsic excitability without cortical inhibition.
iii) Altered Plantar Response (Extensor Plantar = Babinski Sign): Mechanism
Normal plantar response
Stroking the lateral sole of the foot from heel to ball causes flexion of all toes - this is the normal adult response, mediated by cortical suppression of a primitive reflex arc.
Babinski sign (extensor plantar response)
In this patient, the response is extension of the great toe + fanning (abduction) of the other toes when the sole is stroked.
Mechanism:
- The corticospinal tract normally suppresses a spinal flexion withdrawal reflex (the "triple flexion response") that would cause dorsiflexion of the great toe, flexion at hip and knee, and fanning of toes in response to noxious stimuli on the foot.
- When the UMN is damaged by the stroke, this suppression is removed.
- The toe extension (Babinski sign) is actually a component of the disinhibited flexion-withdrawal reflex - as Adams and Victor's states: "the extension movement of the great toe is a component of a larger synergistic flexion or shortening reflex of the leg - a protective (nocifensive) response."
- These spinal flexion reflexes are present "because of disinhibition or release of motor programs of spinal origin."
As Localization in Clinical Neurology states: "The upper motor neuron syndrome is associated with the presence of pathologic reflexes, such as the extensor plantar reflex or Babinski sign, a disinhibited flexion withdrawal reflex."
The Babinski sign is normally present in infants (before myelination of the corticospinal tract is complete) and disappears as the tract matures. Its reappearance in adults is a reliable indicator of corticospinal tract damage at any level.
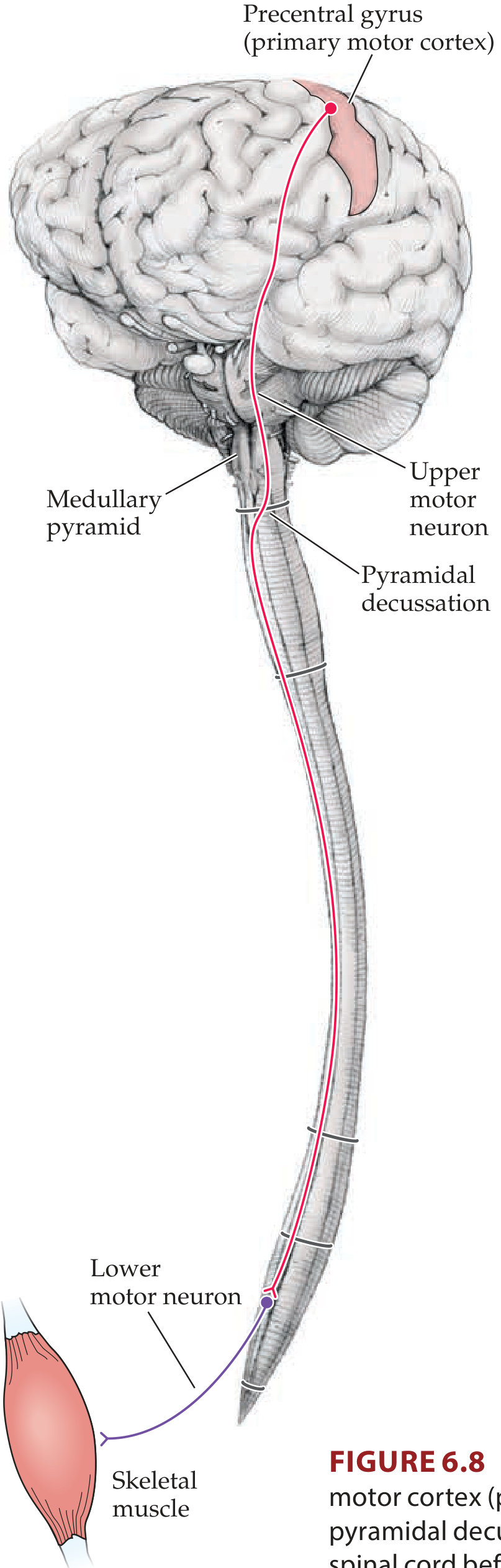
iv) The Corticospinal Tract
The corticospinal tract is the most clinically important descending motor pathway in the nervous system. It controls voluntary movement of the extremities.
Origin (Upper Motor Neuron)
- >50% of fibers originate in the primary motor cortex (Brodmann area 4) of the precentral gyrus
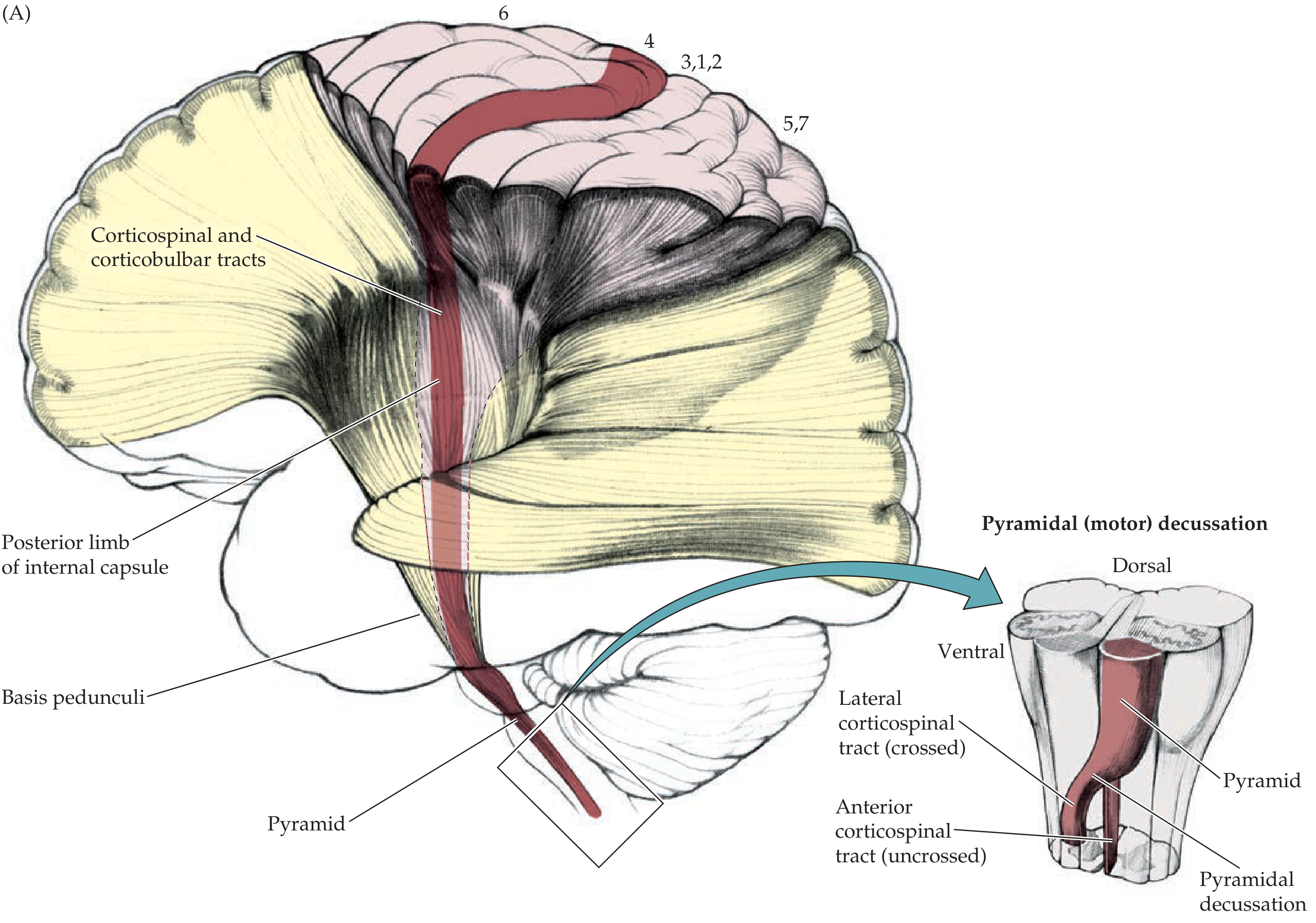
- Remaining fibers arise from the premotor and supplementary motor areas (area 6) and parietal lobe (areas 3, 1, 2, 5, 7)
- Cell bodies reside in cortical layer V; the largest are the Betz cells (giant pyramidal cells, ~3% of corticospinal neurons)
- Topographically organized: face and mouth laterally near the Sylvian fissure; arm and hand in the midportion; trunk near the apex; leg and foot dipping into the longitudinal fissure (motor homunculus)
Course
| Segment | Location | Key Feature |
|---|---|---|
| Cerebral cortex | Layer V of precentral gyrus | Origin of UMN |
| Corona radiata | Subcortical white matter | Fibers fan out |
| Internal capsule | Posterior limb (genu and posterior limb) | Compact, highly vulnerable |
| Cerebral peduncle | Basis pedunculi (middle 3/5) | Midbrain level |
| Pons | Dispersed through pontine nuclei | Crossed by pontine fibers |
| Medullary pyramid | Ventral medulla | Gives the tract its name "pyramidal tract" |
| Pyramidal decussation | Junction of medulla and spinal cord | ~85% of fibers cross here |
| Lateral corticospinal tract | Lateral funiculus of contralateral spinal cord | Main tract; descends to all levels |
| Anterior corticospinal tract | Anterior funiculus of ipsilateral spinal cord | ~15% uncrossed; axial muscles |
Termination (Lower Motor Neuron)
- Fibers synapse on alpha motor neurons and interneurons in the anterior horn of the spinal cord
- From here, lower motor neurons exit via ventral roots to innervate skeletal muscles
Diagram from Neuroanatomy through Clinical Cases:
Clinical Correlation in This Patient
The lesion is in the left internal capsule (or left hemisphere corona radiata/cortex). The internal capsule is a very compact area where all corticospinal fibers are tightly bundled - a small hypertensive lacunar infarct here (from occlusion of lenticulostriate arteries, which are end-arteries particularly prone to hypertensive damage) can cause a dense contralateral hemiplegia affecting both the right arm and right leg equally. Because the fibers decussate at the level of the medulla (already below the lesion), the patient manifests right-sided weakness despite a left-sided brain lesion.
Sources: Neuroanatomy through Clinical Cases, 3rd Ed. - p. 256-260 | Adams and Victor's Principles of Neurology, 12th Ed. - p. 72-74 | Harrison's Principles of Internal Medicine, 22nd Ed. | Guyton and Hall Textbook of Medical Physiology - p. 687
Take reference from guyton
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.