subtalar joint
Reading File
Finding Sources
Searching the Web
subtalar joint anatomy biomechanics clinical
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Excellent. Now I have all the information needed for a comprehensive answer. Let me compile it.
Subtalar Joint
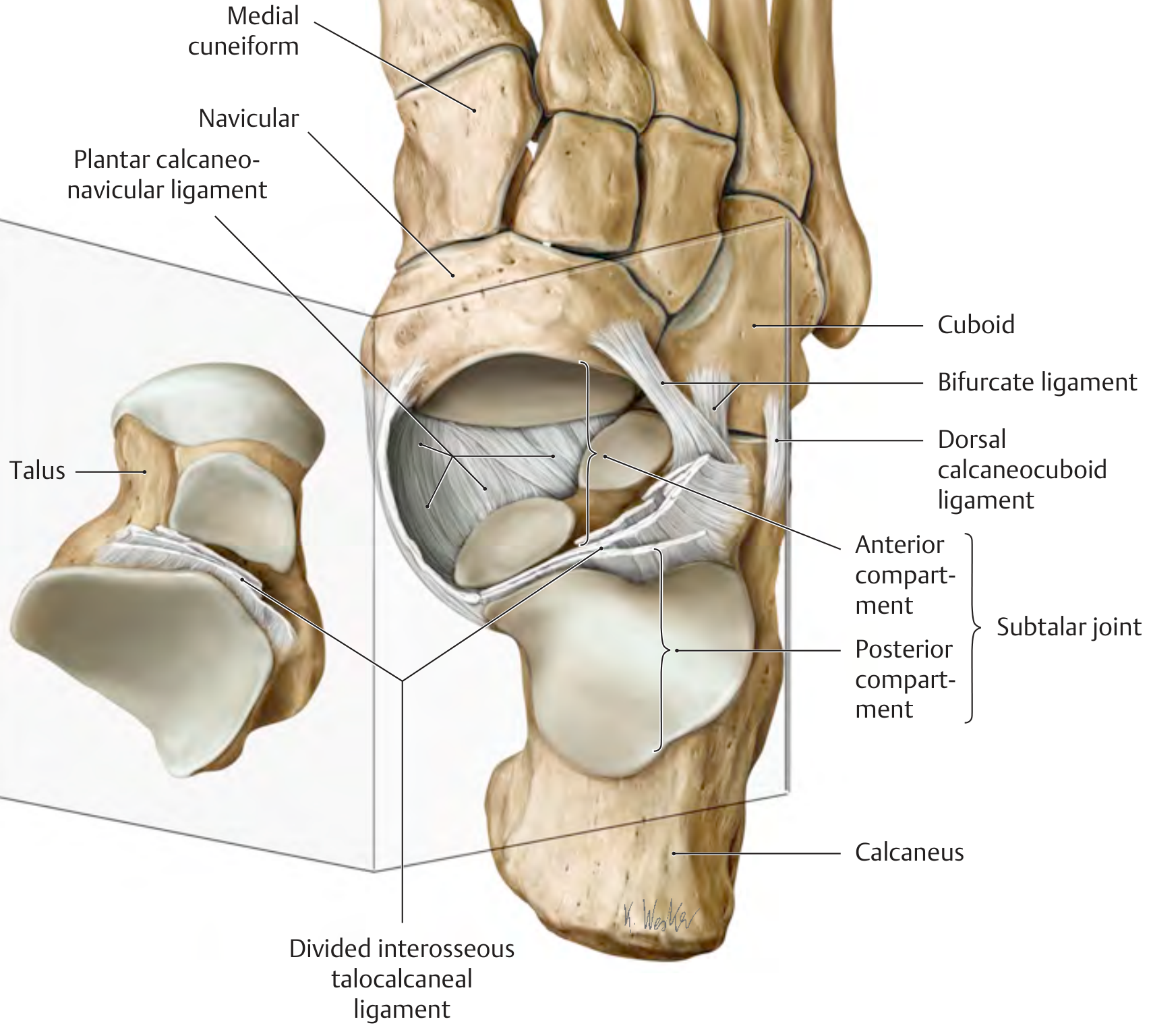
Opened subtalar joint showing the anterior and posterior compartments, divided interosseous talocalcaneal ligament, and surrounding structures. - THIEME Atlas of General Anatomy and Musculoskeletal System
Definition and Overview
The subtalar joint (also called the talocalcaneal joint) is the articulation between the talus and the calcaneus, located just below the ankle joint. It is a complex synovial joint that plays a central role in human locomotion, shock absorption, and adaptation to uneven terrain.
Compartments
The subtalar joint actually consists of two completely separate articulations divided by the interosseous talocalcaneal ligament:
| Compartment | Joint | Key Feature |
|---|---|---|
| Posterior | Talocalcaneal joint (posterior facets) | The larger, weight-bearing compartment; plane-type synovial joint |
| Anterior | Talocalcaneonavicular joint | Talus articulates with calcaneus (anterior + middle facets) AND the navicular head |
The boundary between the two compartments is the tarsal canal (formed by the sulcus tali and sulcus calcanei), whose lateral opening is the tarsal sinus (sinus tarsi).
In about 20% of the general population, there is communication between the subtalar and the talocrural (ankle) joints.
- Imaging Anatomy, Bones, Joints, Vessels and Nerves, p. 482
Articular Surfaces
- Talus (inferior surface): Three facets - posterior, middle, and anterior
- Calcaneus (superior surface): Corresponding posterior, middle (on the sustentaculum tali), and anterior facets
- The plantar calcaneonavicular (spring) ligament contributes to the articular socket of the talocalcaneonavicular joint, providing a cartilage-lined floor for the talar head
Ligamentous Stabilization
| Ligament | Location/Role |
|---|---|
| Interosseous talocalcaneal ligament | Within the tarsal canal; primary stabilizer; divides the two compartments; limits inversion |
| Cervical ligament | Within the sinus tarsi; limits inversion |
| Lateral talocalcaneal ligament | Lateral talar process to lateral calcaneus, anterior to calcaneofibular ligament insertion |
| Medial talocalcaneal ligament | Medial talar tubercle to posterior sustentaculum tali |
| Plantar calcaneonavicular (spring) ligament | Sustentaculum tali to navicular; supports the longitudinal arch; overstretching leads to flat foot |
| Collateral ligaments of the ankle | Also provide indirect support to the subtalar joint |
The medial and lateral collateral ligaments stabilize and guide the subtalar joint because portions remain taut in every joint position. - THIEME Atlas of General Anatomy and Musculoskeletal System
Biomechanics and Range of Motion
The subtalar joint's oblique axis (described by Inman as approximately 42° inclination in the sagittal plane and 23° medial deviation in the axial plane relative to the long axis of the foot) allows it to function as a torque converter between the leg and the foot.
Primary movements are inversion and eversion of the calcaneus (hindfoot):
- Inversion: ~20° (medial rotation of calcaneus)
- Eversion: ~10°
- Combined (clinical test): Normal range is about 5° varus and 5° valgus from neutral
The subtalar joint functions as a bridge between the foot and ankle, transferring loads bidirectionally and acting as a universal joint when combined with the ankle. This is essential for walking on uneven surfaces.
Clinical assessment (Bailey & Love): Hold the talar neck, apply varus/valgus stress to the heel while feeling for heel motion - this isolates the subtalar from talocrural motion.
Clinical Relevance
1. Sinus Tarsi Syndrome
Pain and tenderness over the lateral sinus tarsi, often post-ankle sprain. The sinus tarsi provides an anterolateral approach for injection if ultrasound is unavailable (it communicates into the joint and avoids neurovascular structures).
2. Subtalar Joint Injection
- Approach: anterolateral via sinus tarsi, or posterolateral
- Ultrasound guidance recommended (joint is narrow, covered by thick capsule, and the intrajoint talocalcaneal ligament may resist the needle)
- Materials: 23-gauge needle; 10-40 mg triamcinolone acetonide/hexacetonide or methylprednisolone ± 2 mL 1% lidocaine
- Patient positioned supine, ankle in inversion
- Firestein & Kelley's Textbook of Rheumatology
3. Posttraumatic Subtalar Arthritis
The most common cause is intra-articular calcaneal fractures (Sanders III/IV). Approximately 30% of intra-articular calcaneal fractures develop symptomatic posttraumatic subtalar arthritis. Treatment is subtalar arthrodesis (fusion), performed through a sinus tarsi approach with screw fixation. - Rockwood & Green's Fractures in Adults, 10th ed. 2025
4. Rheumatoid Arthritis / Pantalar Disease
In rheumatoid arthritis or deformity with multi-joint involvement, isolated subtalar arthrodesis or pantalar fusion (ankle + subtalar + midtarsal) may be required, though pantalar fusion is quite disabling.
5. Flat Foot (Pes Planus)
Overstretching of the plantar calcaneonavicular (spring) ligament due to collapse of the longitudinal arch destabilizes the subtalar joint and contributes to progressive flat foot deformity.
6. Adjacent Joint Arthritis after Total Ankle Replacement
Development of subtalar arthritis is a recognized complication post-total ankle arthroplasty; when symptomatic, it may require subtalar arthrodesis concurrent with or staged after the replacement. - Campbell's Operative Orthopaedics, 15th ed. 2026
Summary Table
| Feature | Detail |
|---|---|
| Type | Complex synovial joint (plane-type posterior; ball-and-socket-like anterior) |
| Bones | Talus + calcaneus (+ navicular anteriorly) |
| Key ligaments | Interosseous talocalcaneal, cervical, spring, talocalcaneal medial/lateral |
| Main motion | Inversion/eversion (hindfoot) |
| ROM | Inversion ~20°, eversion ~10° |
| Clinical access | Via sinus tarsi |
| Common pathology | Posttraumatic arthritis, sinus tarsi syndrome, flat foot, RA |
| Definitive treatment for arthritis | Subtalar arthrodesis |
perfect images for its ligaments
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Here are the complete ligament images from the THIEME Atlas of General Anatomy and Musculoskeletal System, covering every view:
Subtalar Joint - Ligaments (All Views)
1. Medial View - Right Foot
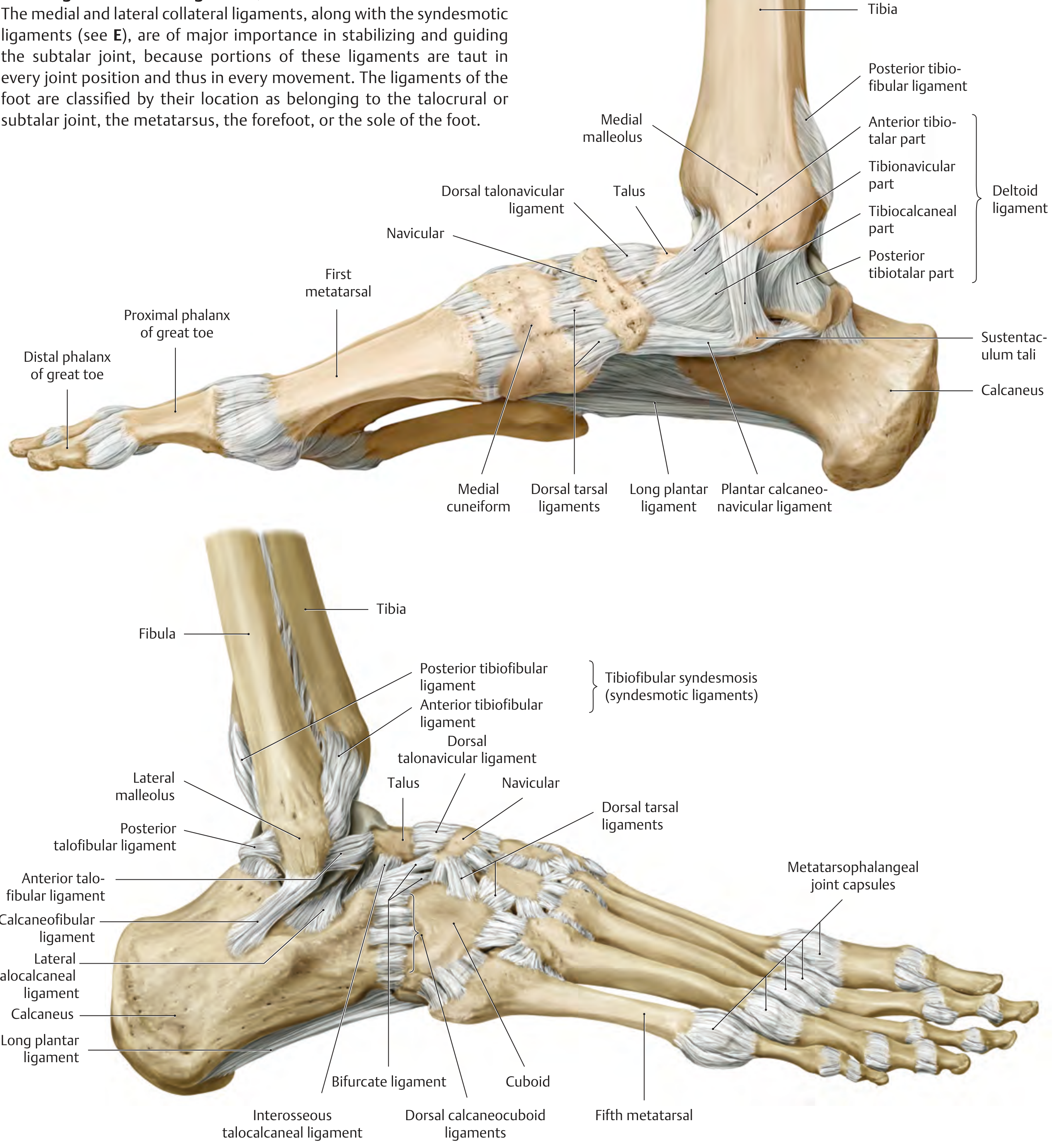
Key structures visible (medial):
- Deltoid ligament (4 parts): anterior tibiotalar, posterior tibiotalar, tibionavicular, tibiocalcaneal parts
- Plantar calcaneonavicular (spring) ligament - from sustentaculum tali to navicular; supports the longitudinal arch and acts as a cartilaginous floor for the talar head
- Long plantar ligament - arch support
- Dorsal talonavicular ligament
- Sustentaculum tali clearly visible as the shelf of the calcaneus supporting the talus medially
2. Lateral View - Right Foot
(Top panel = medial + lateral composite; bottom panel = anterior/dorsal view)
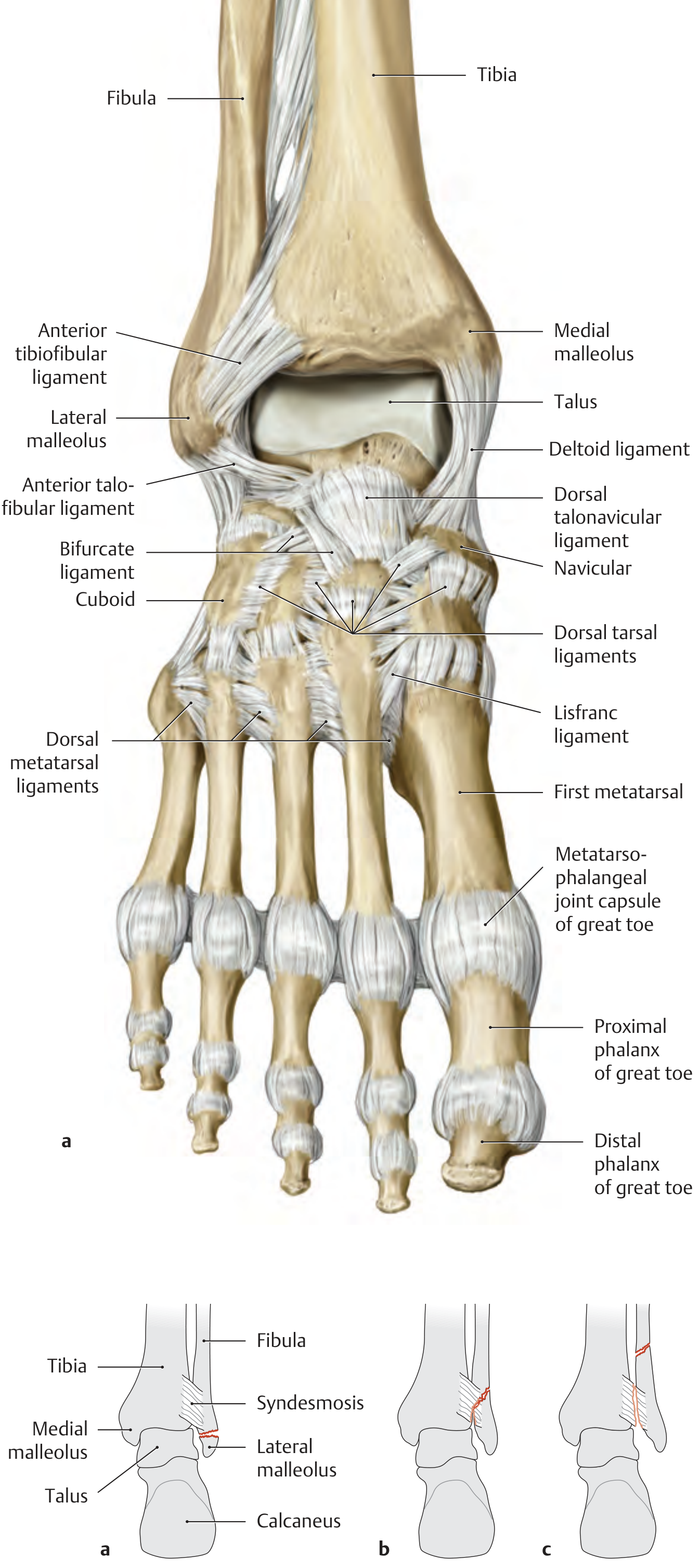
Key structures visible (lateral):
- Anterior talofibular ligament (ATFL) - most commonly torn in ankle sprains
- Calcaneofibular ligament (CFL) - bridges fibula to calcaneus, crosses both ankle and subtalar joints
- Posterior talofibular ligament (PTFL)
- Lateral talocalcaneal ligament - lateral talar process to lateral calcaneus
- Interosseous talocalcaneal ligament - deep within the tarsal canal; primary stabilizer of the subtalar joint
- Bifurcate ligament - Y-shaped ligament from calcaneus to cuboid and navicular
- Tibiofibular syndesmosis (anterior + posterior tibiofibular ligaments)
3. Plantar (Inferior) View - Spring Ligament Complex

Key structures visible (plantar):
- Plantar calcaneonavicular (spring) ligament - runs from sustentaculum tali to navicular, completes the socket for the talar head from the plantar side
- Sustentaculum tali clearly labeled
- Relationship of calcaneus, talus, navicular, and cuboid
4. Overview - Opened Subtalar Joint (from previous response)
Ligament Summary for the Subtalar Joint
| Ligament | Attachment | Function |
|---|---|---|
| Interosseous talocalcaneal | Sulcus tali → sulcus calcanei (inside tarsal canal) | Primary stabilizer; divides anterior/posterior compartments; limits inversion |
| Cervical ligament | Dorsal calcaneus → talar neck (in sinus tarsi) | Limits inversion; taut in eversion |
| Lateral talocalcaneal | Lateral talar process → lateral calcaneus | Lateral stability |
| Medial talocalcaneal | Medial talar tubercle → sustentaculum tali | Medial stability |
| Calcaneofibular | Fibula → calcaneus | Crosses both ankle & subtalar joints; limits inversion |
| Spring (plantar calcaneonavicular) | Sustentaculum tali → navicular | Supports talar head; maintains longitudinal arch |
| Deltoid (tibiocalcaneal part) | Medial malleolus → calcaneus | Indirect medial subtalar support |
| Bifurcate | Calcaneus → navicular + cuboid | Stabilizes midtarsal joints; dorsolateral foot |
All images: THIEME Atlas of General Anatomy and Musculoskeletal System
This is a shared conversation. Sign in to Orris to start your own chat.