STEPS IN BP TAKING I AM MBBS STUDENT DOING INTERNSHIP
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed to give a thorough, well-illustrated answer. Here is a complete guide to BP measurement for your internship:
Blood Pressure Measurement - Complete Guide for MBBS Interns
Equipment Required
- Sphygmomanometer - cuff with inflatable bladder, inflating bulb, controlled exhaust valve, and manometer (mercury, aneroid, or digital)
- Stethoscope (bell end preferred)
- Properly sized cuff
Cuff sizing rule (AHA):
- Bladder width = at least 40-50% of arm circumference at midpoint
- Bladder length = 80% of midarm circumference (or twice the width)
- Using too small a cuff gives falsely HIGH readings; too large gives falsely LOW readings
STEP-BY-STEP PROCEDURE
STEP 1 - Patient Preparation (30 minutes before)
- Ask patient to avoid caffeine, smoking, alcohol, and exercise for 30 min
- Ensure the patient has an empty bladder (full bladder raises BP by ~10-15 mmHg)
- Bring the patient into a quiet room with comfortable ambient temperature
- Let the patient rest for 3-5 minutes before the first reading
- No talking or cell phone use during the rest period or measurements
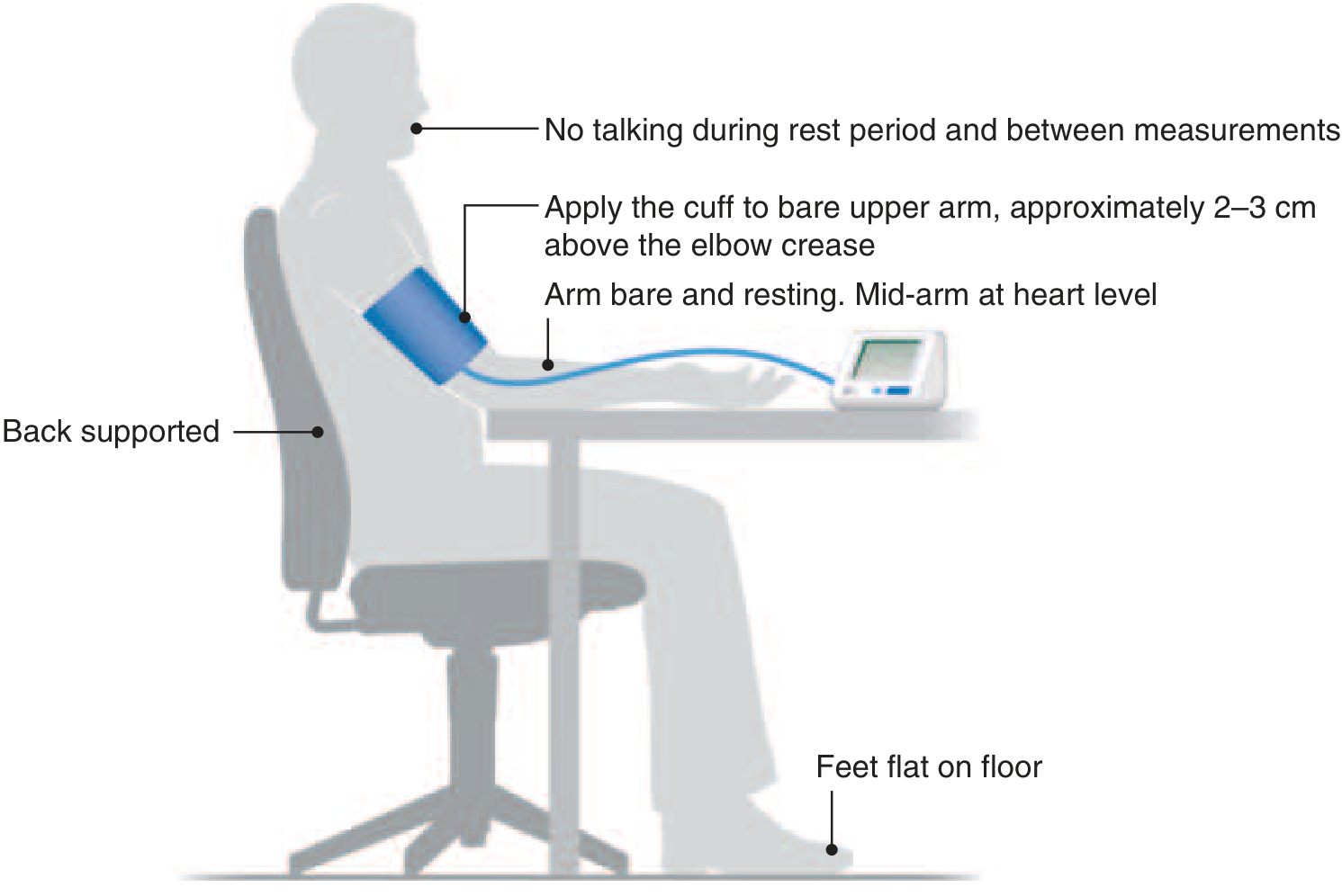
STEP 2 - Positioning the Patient
- Patient seated in a chair with upright back support
- Feet flat on the floor (crossing legs raises BP)
- The measurement arm bare and comfortably supported on a surface
- Mid-arm (cuff) must be at the level of the heart (right atrium)
- If the arm hangs freely parallel to the body, readings will be 9-14 mmHg higher than true value
STEP 3 - Applying the Cuff
- Expose the bare upper arm (no clothing bunched underneath)
- Place the cuff 2-3 cm (approximately 2.5 cm) above the antecubital fossa (elbow crease)
- The center of the inflatable bladder should be placed directly over the brachial artery
- The artery marker on the cuff (if present) should align with the brachial artery
- Wrap the cuff snugly - you should be able to fit 2 fingers underneath, not more
STEP 4 - Estimate Systolic BP by Palpation First (Riva-Rocci technique)
This step helps you avoid missing an auscultatory gap (silent interval between Korotkoff phase I and II, seen in hypertension/arteriosclerosis).
- Palpate the radial pulse with 2 fingers
- Inflate the cuff while palpating the radial artery
- Note the pressure at which the radial pulse disappears - this is the estimated systolic BP
- Inflate 30 mmHg above this level for the auscultatory measurement
- Deflate fully and wait 30-60 seconds before re-inflating for auscultation
STEP 5 - Auscultatory Measurement (Standard Method)
- Place the bell of the stethoscope (or diaphragm) lightly over the brachial artery in the cubital fossa - do NOT tuck it under the cuff
- Reinflate the cuff to 30 mmHg above the estimated systolic (from Step 4)
- Open the deflation valve and deflate slowly at 2-3 mmHg per second (or per beat)
- Listen carefully for Korotkoff sounds
Korotkoff Sounds - What to Listen For
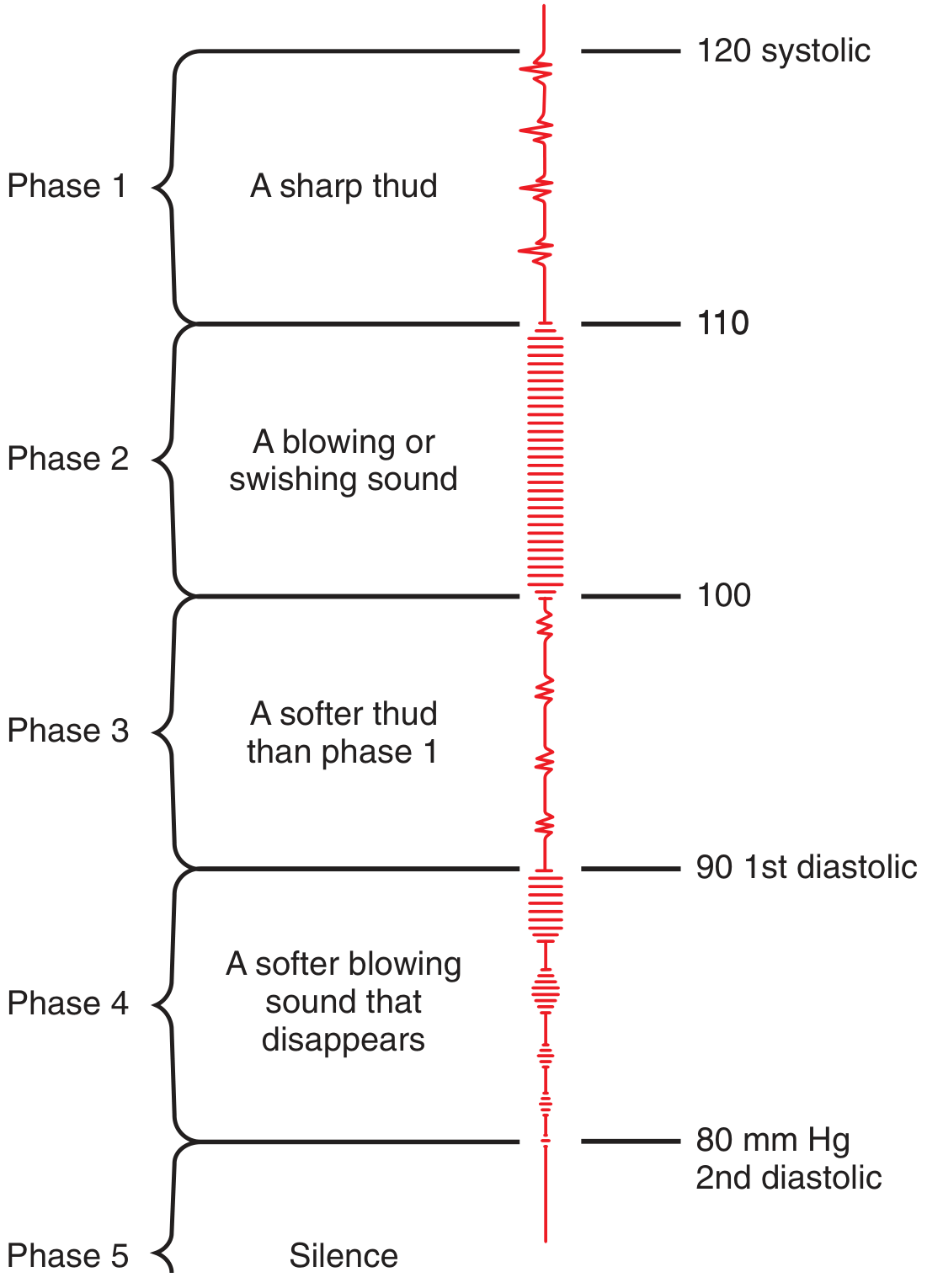
| Phase | Sound | Clinical Significance |
|---|---|---|
| Phase I | First faint, clear, sharp tapping sound | = Systolic BP |
| Phase II | Blowing or swishing sound (softer) | (may disappear = auscultatory gap) |
| Phase III | Softer thud, crisper than Phase II | |
| Phase IV | Distinct muffling - soft, blowing quality | = Diastolic BP in children |
| Phase V | Complete disappearance of sounds | = Diastolic BP in adults |
In adults: Record Korotkoff Phase I as systolic, Phase V as diastolic. In children and pregnant women: Use Phase IV as diastolic.
STEP 6 - Recording and Reporting
- Record the exact mmHg readings - do not round up or down excessively
- Report as systolic/diastolic (e.g., 120/80 mmHg)
- Note which arm was used, patient position (sitting/lying/standing), and time
- Inform the patient of the result
STEP 7 - Repeat Measurements
- Take at least 2 readings separated by at least 1-2 minutes in the same sitting
- Use the average of the two readings
- If readings differ by >5 mmHg, take a third and average all three
- On the first visit, measure BP in both arms - use the arm with the higher reading subsequently
- An inter-arm difference of >15 mmHg systolic is clinically significant (consider subclavian stenosis)
BP Classification (ACC/AHA 2017)
| Category | Systolic (mmHg) | Diastolic (mmHg) | |
|---|---|---|---|
| Normal | <120 | and | <80 |
| Elevated | 120-129 | and | <80 |
| Stage 1 Hypertension | 130-139 | or | 80-89 |
| Stage 2 Hypertension | ≥140 | or | ≥90 |
Source: Harrison's Principles of Internal Medicine 22E (2025)
Common Errors to Avoid
| Error | Effect on Reading |
|---|---|
| Cuff too small | Falsely HIGH |
| Cuff too large | Falsely LOW |
| Arm below heart level | Falsely HIGH |
| Arm above heart level | Falsely LOW |
| Not waiting after exercise/smoking | Falsely HIGH |
| Deflating too fast (>3 mmHg/sec) | Underestimates systolic, overestimates diastolic |
| Stethoscope under the cuff | Falsely LOW |
| Not palpating first | Misses auscultatory gap, underestimates systolic |
| Patient talking during measurement | Raises BP ~10 mmHg |
| Full bladder | Raises BP ~10-15 mmHg |
| Crossed legs | Raises systolic ~2-8 mmHg |
Special Situations You May Encounter in Internship
Auscultatory Gap: A period of silence between Phase I and Phase II, common in hypertension and arteriosclerosis. If you miss Phase I, you record a falsely low systolic BP. Always palpate first to avoid this.
Orthostatic (Postural) BP: Measure lying down, then after 1 minute standing. A drop of ≥20 mmHg systolic or ≥10 mmHg diastolic = orthostatic hypotension. Common in elderly, dehydration, autonomic neuropathy, antihypertensives.
Pulsus Paradoxus: Measure the difference in systolic BP between expiration and inspiration. >10 mmHg difference is abnormal - seen in cardiac tamponade, severe asthma, COPD.
Lower Limb BP: Popliteal artery used with a thigh cuff - normally 20-30 mmHg higher than upper limb. A low thigh BP compared to arm BP suggests coarctation of the aorta.
Sources: Harrison's Principles of Internal Medicine 22E (2025); Roberts and Hedges' Clinical Procedures in Emergency Medicine; Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.