I now have all the content needed for a thorough, well-illustrated answer. Let me compose it.
Monteggia Fracture-Dislocation: A Complete Guide
What Is It?
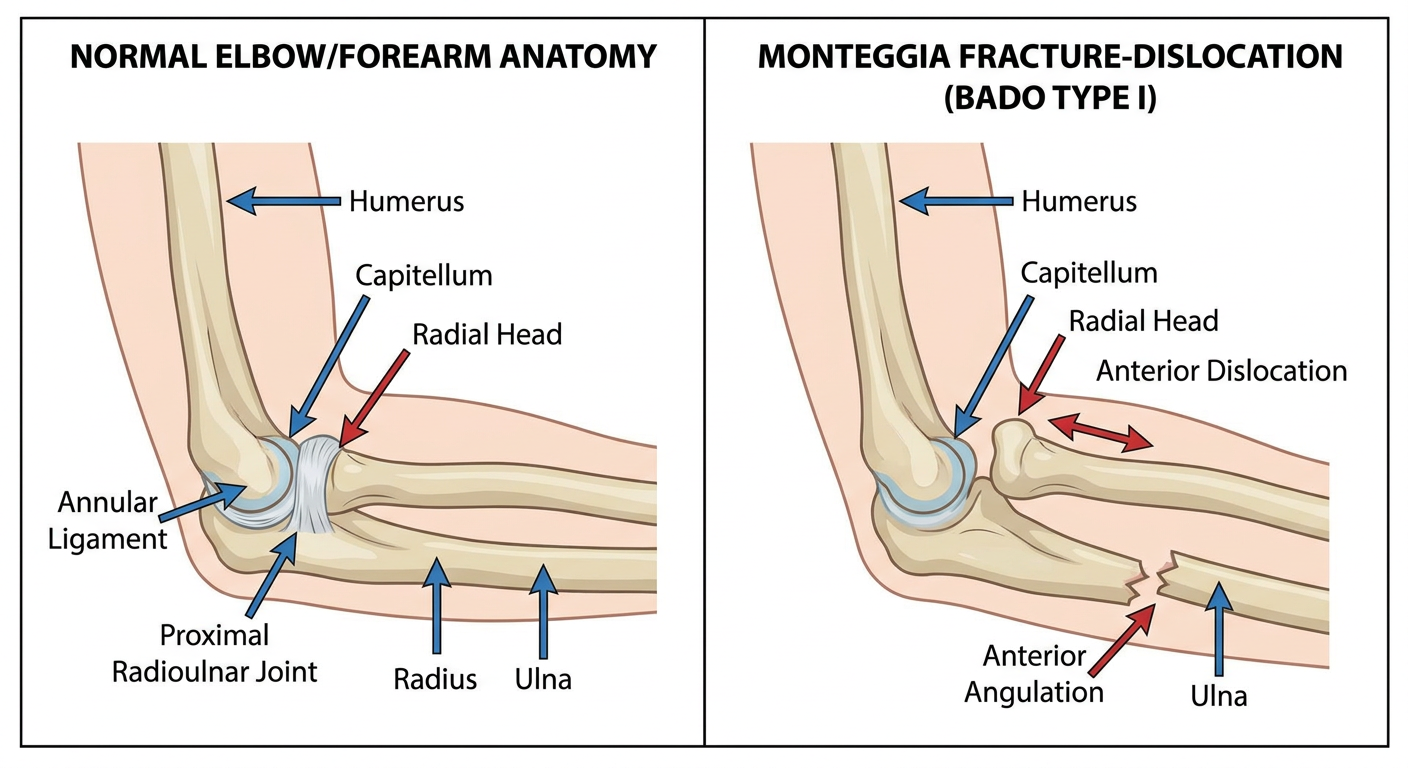
A Monteggia fracture is a fracture of the proximal or middle third of the ulna combined with a dislocation of the radial head at the proximal radioulnar joint (PRUJ). It is named after Giovanni Battista Monteggia, an Italian surgeon who first described the injury in 1814.
The key concept: the ulna breaks and the radial head dislocates - these two injuries always occur together, and failure to recognize the radial head dislocation is a classic diagnostic pitfall that can lead to chronic pain, loss of motion, and need for salvage surgery.
"The associated radial head dislocation may be easily missed. Missing the radial head dislocation can lead to chronic pain, limited range of motion, and possibly radial head excision as treatment." - Tintinalli's Emergency Medicine
Anatomy Relevant to the Injury
The forearm contains two parallel bones - the radius and ulna - connected by:
- The proximal radioulnar joint (PRUJ): radial head articulates in the radial notch of the ulna, held by the annular ligament
- The interosseous membrane (IOM): binds radius and ulna along their shafts
- The radiocapitellar joint: radial head articulates with the capitellum of the humerus
When the ulna fractures, the intact IOM and annular ligament transmit force to the radial head, causing it to dislocate. The direction of dislocation corresponds directly to the direction of the apex of the ulnar fracture.
Epidemiology
| Feature | Details |
|---|
| Incidence | Rare - ~1-2% of all forearm fractures |
| Pediatric peak | Ages 4-10 years |
| Adult predominance | Type II (posterior) - up to 70-80% of adult cases |
| Pediatric predominance | Type I (anterior) - most common in children |
Causes and Mechanism of Injury
Monteggia fractures occur from two main mechanisms:
1. Fall on Outstretched Hand (FOOSH) - Type I most common
- The patient falls with the forearm in forced pronation
- The hand hits the ground, transmitting force up the forearm
- The ulna fractures with anterior angulation
- The force drives the radial head anteriorly out of its articulation
- Common in children and young adults
2. Direct Blow to the Posterior Forearm - Type II
- A direct blow strikes the dorsal (posterior) surface of the proximal forearm
- The ulna fractures with posterior angulation
- The radial head dislocates posteriorly
- The annular ligament is disrupted
- More common in adults, especially with high-energy mechanisms
3. Hyperpronation Mechanism - Type III
- Violent varus force applied to a partially flexed elbow
- Ulnar metaphysis fractures
- Radial head displaces laterally
- Predominantly a pediatric injury
4. High-Energy Trauma - Type IV
- Combined forearm fracture (both ulna and radius) with radial head dislocation
- Seen in high-velocity injuries (motor vehicle accidents, machinery)
Classification
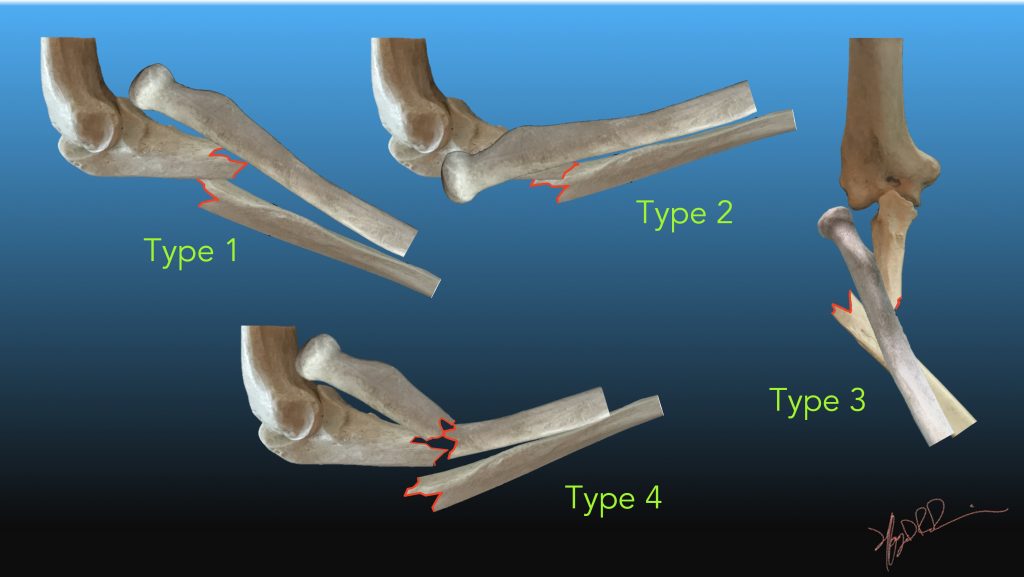
Bado Classification (Primary - based on direction of radial head dislocation)
| Type | Radial Head Dislocation | Ulnar Fracture | Frequency |
|---|
| I | Anterior | Diaphysis, apex anterior angulation | ~60% (most common overall, #1 in children) |
| II | Posterior or posterolateral | Diaphysis, apex posterior angulation | ~15% (70-80% of adult cases) |
| III | Lateral or anterolateral | Metaphysis (distal to coronoid) | ~20% (almost exclusively pediatric) |
| IV | Anterior | Same level as radial fracture + proximal 1/3 radius fracture | ~5% (rare, adults only) |
"Understanding the deformity of the ulna and the direction of dislocation of the radial head is important for fracture reduction. In most instances, reduction of the ulnar fracture leads to reduction of the radial head." - Rockwood and Green's Fractures in Adults
Jupiter Modification of Bado Type II (most clinically significant subclassification)
Type II Monteggia fractures in adults frequently involve radial head or coronoid fractures, making them complex elbow instability patterns. Jupiter divided them by ulnar fracture location:
| Subtype | Ulnar Fracture Location |
|---|
| IIA | Very proximal - through the coronoid and olecranon |
| IIB | Junction of proximal metaphysis and diaphysis (not involving coronoid) |
| IIC | Diaphyseal fracture |
| IID | Complex - involves ulna from olecranon into diaphysis |
Monteggia Equivalents
When a radial head fracture occurs instead of a true dislocation alongside an ulnar fracture, this is termed a "Monteggia equivalent." The interosseous membrane evaluation is important in these injuries.
Signs and Symptoms
History
- Mechanism as above (FOOSH, direct blow, sports injury, MVA)
- Immediate pain at the forearm and elbow
- Inability to move the elbow or forearm
Physical Examination
| Finding | Description |
|---|
| Pain and swelling | Significant pain and swelling at the elbow and proximal forearm |
| Elbow deformity | Visible deformity of the elbow joint |
| Forearm shortening/angulation | The forearm may appear shortened and angulated |
| Palpable radial head | Radial head may be palpable in an anterolateral (Type I) or posterolateral (Type II) location |
| Restricted ROM | Limited forearm rotation (pronation/supination) and elbow flexion/extension |
| Tenderness | Point tenderness along proximal ulna at fracture site; tenderness over radial head |
| Neurovascular exam | PIN (posterior interosseous nerve) deficit - weakness of finger/wrist extension; must be documented pre-operatively |
Neurovascular Complications at Presentation
- Posterior Interosseous Nerve (PIN) palsy - occurs in ~10% of cases; presents as weakness of finger extension and wrist drop
- Radial nerve injury (less common)
- Vascular injury (rare but must be excluded in high-energy trauma)
Investigations
Plain Radiographs (First-Line)
The cornerstone of diagnosis. Two key rules:
Rule 1: Always include the elbow joint on forearm X-rays and always include forearm views with elbow X-rays.
"All forearm fracture radiographs should be accompanied by elbow radiographs to evaluate for radial head dislocation." - Miller's Review of Orthopaedics
Rule 2 - Radiocapitellar Line: On any X-ray, a line drawn through the center of the radial head should pass through the center of the capitellum. If it does not, the radial head is dislocated.
Views needed:
- AP and lateral of the forearm
- AP and lateral of the elbow
AP view: Note proximal ulnar fracture and displaced radial head at the elbow
Lateral view: The apex of the ulnar fracture angulation points in the direction of radial head dislocation - this is a key radiographic clue
Key radiographic sign: The apex of the ulnar fracture always points in the same direction as the radial head dislocation.
Pediatric note: In children, a plastic deformation (bow) of the ulna without a visible fracture line can cause radial head dislocation - this is easily missed.
CT Scan
- Indicated when plain films are equivocal
- Better delineates coronoid fractures (critical for Jupiter classification of Type II)
- Helps assess radial head comminution and fracture pattern
- Pre-operative planning tool
MRI
- Rarely needed acutely
- Useful to assess annular ligament and lateral collateral ligament (LCL) integrity in chronic cases
- Guides reconstructive planning in chronic Monteggia injuries
Associated Injuries
| Associated Injury | Significance |
|---|
| Radial head fracture (Monteggia equivalent) | Present in many Type II injuries; may need ORIF or arthroplasty |
| Coronoid fracture | Critical - affects elbow stability; must be fixed if present |
| Lateral collateral ligament (LCL) injury | Causes elbow instability; repair may be required |
| Annular ligament rupture | Especially in Type II; may prevent radial head reduction |
| PIN (posterior interosseous nerve) palsy | ~10% incidence; usually neuropraxia - resolves in 3 months |
| Olecranon fracture | With proximal ulnar injury patterns |
| Elbow dislocation | Transolecranon fracture-dislocation variants |
| Open fractures | In high-energy mechanisms |
| Compartment syndrome | Must monitor post-injury and post-operatively |
Treatment
Emergency Stabilization
- Neurovascular assessment (document PIN function)
- Closed reduction attempt (especially in children)
- Splint/backslab in position of reduction
- Urgent orthopedic referral
Pediatric Treatment (Age < 10 years)
Most pediatric Monteggia fractures can be managed non-operatively:
Closed Reduction:
- Performed under sedation/anesthesia
- Technique: Longitudinal traction on forearm + correction of ulnar angulation + pressure on radial head in opposite direction to dislocation
- For Type I: Flex elbow to 90-110° (tightens anterior structures, maintains reduction)
- For Type II: Position in extension
- After reduction: Above-elbow cast for 6-8 weeks
Operative Indications in Children:
- Failed or irreducible closed reduction
- Unstable reduction
- Chronic/missed injuries
- Soft tissue interposition blocking reduction (often annular ligament)
Intramedullary (IM) fixation of the ulna is the preferred operative technique in children when surgery is needed.
Adult Treatment
"These injuries usually require operative intervention in adults... and should only be treated nonoperatively in a patient who is too frail or has too much medical comorbidity to tolerate a surgical procedure." - Rockwood and Green's Fractures in Adults
Open Reduction and Internal Fixation (ORIF) is the standard of care in adults.
Surgical Approach
- Position: Lateral decubitus on a radiolucent table
- Incision: Posterior midline incision; full-thickness skin flaps created
- Interval: Between ECU (extensor carpi ulnaris) and FCU (flexor carpi ulnaris)
Step-by-Step Surgical Protocol (Rockwood and Green / Campbell's)
| Step | Action |
|---|
| 1 | Posterior approach with thick subcutaneous flaps |
| 2 | Develop interval between ECU and FCU |
| 3 | Assess and address radial head fracture if present (repair or replace) |
| 4 | Anatomic reduction of ulnar shaft with provisional mini-fragment plate fixation |
| 5 | Fix coronoid fracture if present (mini-fragment plates, screws, or sutures) |
| 6 | Definitive plate fixation of proximal ulna (precontoured locking plate preferred) |
| 7 | Assess PRUJ and radiocapitellar joint reduction under fluoroscopy |
| 8 | Evaluate and repair LCL with suture anchors if avulsed |
Key principle: Anatomic reduction of the ulna almost always leads to spontaneous reduction of the radial head. If the radial head remains subluxed after anatomic ulnar fixation, check for:
- Malreduction of the ulna (most common cause)
- Interposed annular ligament
- Associated radial head fracture requiring fixation/replacement
Implants Used
- Precontoured proximal ulna locking plates (preferred)
- LCDC (Limited Contact Dynamic Compression) plates
- Mini-fragment plates and T-plates for coronoid fragments
- Radial head arthroplasty (if radial head is not salvageable)
- Suture anchors (for LCL repair)
Chronic Monteggia Fracture (Missed/Neglected)
Controversial when "acute" becomes "chronic," but generally >4 weeks is considered chronic.
Clinical features: Pain, decreased ROM, cubitus valgus deformity, PIN palsy.
Treatment:
- Symptomatic patients with no radial head deformity (especially younger patients): operative reconstruction
- Key principle: Ulnar osteotomy to restore ulnar length + annular ligament reconstruction
- Annular ligament reconstruction options: Native ligament repair, triceps tendon strip (Bell-Tawse technique), or fascia graft
- Avoid radial head resection in young patients - risk of late deformity; reserve as salvage only
- Complications are high: compartment syndrome, residual subluxation, ulnar nerve palsy, nonunion
Complications
| Complication | Notes |
|---|
| PIN palsy | Most common nerve injury (~10%); usually neuropraxia; observe 3 months before exploring |
| Recurrent radial head dislocation | Often due to inadequate ulnar reduction |
| Radioulnar synostosis | Bridging bone between radius and ulna; restricts rotation |
| Loss of motion | Especially pronation/supination |
| Nonunion of ulna | Usually a technical error |
| Compartment syndrome | Must monitor post-operatively |
| Infection | Post-surgical |
| Radial head arthrosis | Late complication after chronic dislocation |
Key Mnemonic - "RADS"
R - Radial head always dislocates in Monteggia (not the wrist - that's Galeazzi)
A - Apex of ulnar fracture points toward radial head dislocation
D - Direction of dislocation = Bado type (Anterior I, Posterior II, Lateral III)
S - Suspect PIN injury (spontaneous recovery expected)
Monteggia vs. Galeazzi - Quick Comparison
| Feature | Monteggia | Galeazzi |
|---|
| Fracture | Proximal/middle ulna | Distal radius |
| Dislocation | Radial head (PRUJ) | DRUJ (distal radioulnar joint) |
| Common age | Children (Type I) / Adults (Type II) | Adults > children |
| Nerve at risk | PIN (posterior interosseous) | None typically |
| Mnemonic | "Monteggia = ulna + radial head up" | "Galeazzi = radius + wrist joint" |
Sources
- Rockwood and Green's Fractures in Adults, 10th Edition (2025) - Classification, mechanism, treatment
- Campbell's Operative Orthopaedics, 15th Edition (2026) - Surgical technique, chronic Monteggia
- Miller's Review of Orthopaedics, 9th Edition - Classification and complications
- Tintinalli's Emergency Medicine - Emergency assessment and management
- Bado JL. The Monteggia Lesion. Clin Orthop Relat Res. 1967;50:71
- Jupiter et al. - Jupiter modification of Type II classification