Now I have everything needed. Here is the full, image-rich, flowchart-structured revision notes:
🦾🦵 UPPER LIMB & LOWER LIMB ANATOMY
NEET PG & INICET Master Revision Notes
Source: Gray's Anatomy for Students | THIEME Atlas | Harriet Lane | Miller's Orthopaedics
═══════════════════════════════
PART 1 — UPPER LIMB
═══════════════════════════════
🔴 TOPIC 1: BRACHIAL PLEXUS ⭐⭐⭐ (Most Repeated)
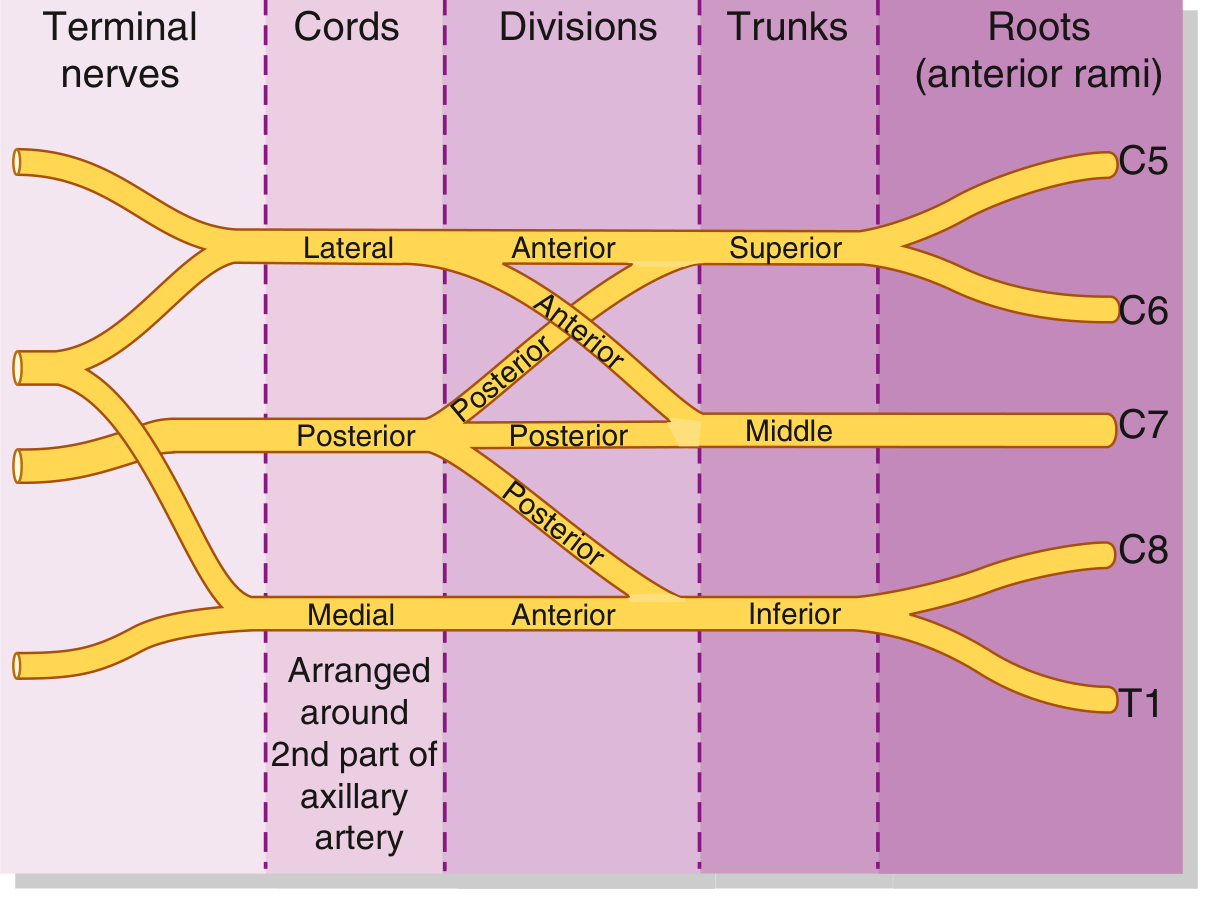
Textbook Diagram (Gray's Anatomy for Students)
Brachial Plexus — Roots, Trunks, Divisions, Cords (Gray's Anatomy for Students)
Brachial Plexus Schematic — cords arranged around 2nd part of axillary artery
FLOWCHART: Brachial Plexus Formation
ROOTS (Ant. rami) TRUNKS DIVISIONS CORDS
┌──────────────┐
C5 ──────────────────►│ │──Ant──►┐
│ SUPERIOR │ │ LATERAL CORD
C6 ──────────────────►│ │──Post─►┤ (C5,C6,C7)
└──────────────┘ ▼
┌──────────────┐ Posterior ───► POSTERIOR CORD
C7 ──────────────────►│ MIDDLE │──Post─►┤ (C5–T1)
└──────────────┘ │
┌──────────────┐ │
C8 ──────────────────►│ │──Post─►┘
│ INFERIOR │──Ant──► MEDIAL CORD
T1 ──────────────────►│ │ (C8, T1)
└──────────────┘
FLOWCHART: Branches from Each Level
ROOTS ──────────► Dorsal Scapular (C5) → Rhomboids
└───► Long Thoracic (C5,C6,C7) → Serratus Anterior
UPPER TRUNK ────► Suprascapular → Supraspinatus + Infraspinatus
└───► Nerve to Subclavius
LATERAL CORD ──► Lateral Pectoral → Pec Major (clavicular)
├──► Musculocutaneous → Coracobrachialis, Biceps, Brachialis
└──► Lateral root of MEDIAN nerve
MEDIAL CORD ───► Medial Pectoral → Pec Major + Minor
├──► Medial cutaneous nerve of arm + forearm
├──► ULNAR nerve
└──► Medial root of MEDIAN nerve
POSTERIOR CORD ► Upper subscapular → Subscapularis (upper)
├──► Thoracodorsal → Latissimus Dorsi
├──► Lower subscapular → Subscapularis (lower) + Teres Major
├──► AXILLARY nerve → Deltoid + Teres Minor
└──► RADIAL nerve
BRACHIAL PLEXUS INJURY TABLE
| Injury | Root | Deformity | Key Features | PYQ |
|---|
| Erb-Duchenne | C5, C6 | "Waiter's tip" — adduction + internal rotation, pronated forearm, flexed wrist | Most common (90%); C4 → diaphragm palsy; Biceps function = prognostic indicator | ⭐ INICET 2021, 2022 |
| Total plexus palsy | C5–T1 | Entire limb involved; Horner if T1 | 8–9% | — |
| Klumpke | C8, T1 | Claw hand, flaccid hand | <2%; Horner syndrome (ptosis, anhidrosis, miosis) | ⭐ INICET 2021 |
🔴 PYQs — Brachial Plexus
Q (INICET 2022): Which cord of brachial plexus gives the ulnar nerve?
A: Medial cord ✅
Q (INICET 2023): Which nerve is injured in winged scapula?
A: Long thoracic nerve (C5–C7) — loss of serratus anterior ✅
Q (NEET PG 2025): Long head of triceps brachii originates from?
A: Infraglenoid tubercle ✅ (Long head of biceps = supraglenoid tubercle)
🔴 TOPIC 2: THREE POSTERIOR AXILLARY SPACES ⭐⭐⭐
FLOWCHART: Spaces of Posterior Axillary Wall
Long head of Triceps divides the space into:
TRIANGULAR SPACE (medial) QUADRANGULAR SPACE (lateral)
Borders: Borders:
- Superior: Teres minor/subscap - Superior: Teres minor/subscap
- Inferior: Teres major - Inferior: Teres major
- Lateral: Long head of Triceps - Medial: Long head of Triceps
- Lateral: Surgical neck of humerus
Contents: Contents:
⬛ Circumflex scapular artery ⬛ AXILLARY NERVE
⬛ Posterior circumflex humeral A+V
TRIANGULAR INTERVAL (below)
Borders:
- Superior: Teres major
- Medial: Long head of triceps
- Lateral: Shaft of humerus
Contents:
⬛ RADIAL NERVE
⬛ Profunda brachii (deep brachial) artery
Memory trick: "ACE" → Axillary-Circumflex-Extensor(radial)
- Quadrangular → Axillary
- Triangular (space) → Circumflex scapular
- Triangular interval → Radial + Profunda brachii
🔴 PYQs — Spaces
Q (INICET 2022): What passes through the quadrangular space?
A: Axillary nerve + Posterior circumflex humeral artery ✅
Q: Radial nerve enters the posterior compartment of arm via?
A: Triangular interval ✅
🔴 TOPIC 3: INDIVIDUAL NERVE INJURIES ⭐⭐⭐
FLOWCHART: Radial Nerve Injury at Different Levels
RADIAL NERVE (C5–C8, T1) — from Posterior Cord
At AXILLA (crutch palsy):
→ Wrist drop + finger drop
→ Triceps ALSO paralysed
→ Loss of elbow extension
At RADIAL GROOVE / MID-SHAFT HUMERUS FRACTURE: ★ Most Common
→ WRIST DROP (extensors lost)
→ Triceps SPARED (branches given before groove)
→ Sensory loss dorsum of hand
At ELBOW (lateral epicondyle/radial head fracture):
Bifurcates into:
├── SUPERFICIAL branch (purely sensory) → dorsolateral hand skin
└── DEEP branch = Posterior Interosseous Nerve (PIN)
→ Supplies all posterior forearm extensors
→ Injury → FINGER DROP (no wrist drop — ECRL/ECRB spared)
FLOWCHART: Median Nerve Injury at Different Levels
MEDIAN NERVE (C6–C8, T1) — Lateral + Medial cords
No branches in ARM
At FOREARM — AIN (Anterior Interosseous Nerve):
→ Supplies FPL + lateral FDP + pronator quadratus
→ Injury → Cannot make "OK sign"
→ No sensory loss
At WRIST (Carpal Tunnel Syndrome): ★ Most Common
→ APE HAND (thenar wasting, thumb cannot oppose)
→ Loss of sensation lateral 3½ digits
→ PALMAR BRANCH SPARED (passes superficial to retinaculum)
→ Thenar skin sensation INTACT
In HAND:
├── Recurrent (thenar) branch → 3 thenar muscles
└── Lateral 2 lumbricals (index, middle)
FLOWCHART: Ulnar Nerve Injury at Different Levels
ULNAR NERVE (C7, C8, T1) — Medial cord
No branches in ARM
Passes POSTERIOR to medial epicondyle ← Injury site #1
At ELBOW:
→ FCU + medial FDP LOST
→ CLAW less severe (paradox!) — some lumbrical function lost
→ Sensory loss medial 1½ digits
At WRIST (Guyon's canal, lateral to pisiform): ← Injury site #2
→ FCU + medial FDP SPARED
→ CLAW more severe (ring + little worse)
→ All interossei + adductor pollicis LOST
→ FROMENT SIGN (+) — loses adductor pollicis, compensates with FPL
→ WARTENBERG SIGN (+) — little finger abducts (EDM unopposed)
In HAND — deep branch:
├── All interossei (DAB/PAD)
├── Adductor pollicis
├── Hypothenar muscles (3)
└── Medial 2 lumbricals (ring, little)
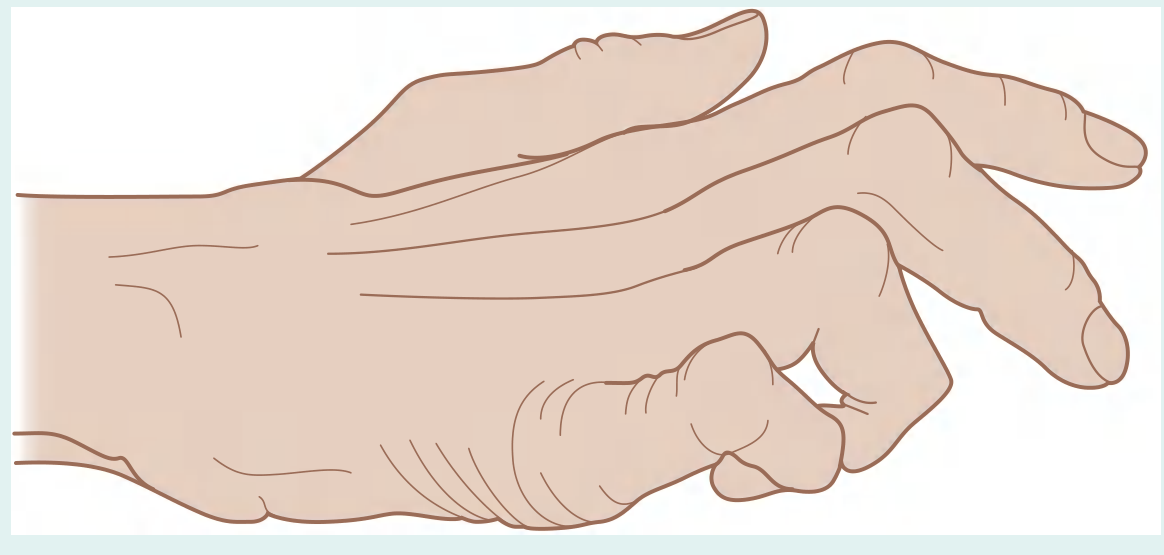
Clawed Hand Image (Gray's Anatomy)
"Clawed Hand" — Ulnar nerve lesion. MCP hyperextended + IPJ flexed in ring and little fingers.
NERVE INJURY SUMMARY TABLE (Upper Limb)
| Nerve | Level of Injury | Deformity | Test | Spared |
|---|
| Radial | Radial groove | Wrist drop | Weakness of wrist extension | Triceps (branches given above) |
| Radial (PIN) | Lateral epicondyle | Finger drop, NO wrist drop | Weakness extending fingers | ECRL, ECRB (wrist extension intact) |
| Median | Carpal tunnel | Ape hand | Cannot oppose thumb | Palmar branch (skin over thenar eminence) |
| Median (AIN) | Forearm | Cannot make OK sign | FPL, FDP(index) weak | No sensory loss |
| Ulnar | Elbow | Claw (less severe) | FCU, FDP lost | — |
| Ulnar | Wrist | Claw (more severe) | Froment sign; Wartenberg sign | FCU, medial FDP |
| Axillary | Surgical neck humerus/shoulder dislocation | Loss of shoulder abduction >15°; deltoid wasting | Regimental badge area numbness | — |
| Musculocutaneous | Coracobrachialis | Weak elbow flexion | — | Lateral cutaneous nerve forearm |
🔴 PYQs — Nerve Injuries
Q (INICET 2022): Injury at wrist gives more severe claw than elbow for ulnar nerve — why?
A: At elbow, FCU and FDP to medial fingers are also lost — partial compensation. At wrist, lumbricals to ring and little fingers also lost → more severe clawing (Ulnar paradox) ✅
Q: Froment's sign tests which nerve?
A: Ulnar nerve (adductor pollicis paralysis) ✅
Q (INICET 2023): Rotator cuff muscles — mnemonic?
A: SITS — Supraspinatus, Infraspinatus, Teres minor, Subscapularis ✅
🔴 TOPIC 4: CUBITAL FOSSA ⭐⭐
FLOWCHART: Cubital Fossa
LATERAL EPICONDYLE ←———→ MEDIAL EPICONDYLE
Brachioradialis Pronator Teres
(lateral wall) (medial wall)
CONTENTS (Lat → Med): "BiTAMeN"
┌──────────────────────────────────────────────────────┐
│ Biceps tendon │
│ (covered by bicipital aponeurosis) │
│ brachial Artery ← bifurcates into Radial + Ulnar │
│ Median Nerve │
│ [Radial nerve — under lip of brachioradialis] │
└──────────────────────────────────────────────────────┘
ROOF: Skin + fascia + Median cubital vein (used for venipuncture)
Bicipital aponeurosis → protects brachial A + median N
FLOOR: Brachialis + Supinator
KEY: Ulnar nerve does NOT pass through cubital fossa
(passes POSTERIOR to medial epicondyle)
🔴 TOPIC 5: CARPAL TUNNEL ⭐⭐⭐
CARPAL TUNNEL CONTENTS (9 tendons + 1 nerve):
┌────────────────────────────────────────┐
│ 4 × FDS tendons │
│ 4 × FDP tendons │
│ 1 × FPL tendon │
│ MEDIAN NERVE │
│ │
│ Note: Ulnar nerve + artery = OUTSIDE │
│ (pass in Guyon's canal, superficial │
│ to flexor retinaculum) │
└────────────────────────────────────────┘
Roof: Flexor retinaculum
Floor/walls: 8 carpal bones
PALMAR BRANCH of median nerve → passes SUPERFICIAL to retinaculum
→ Spared in CTS → Thenar skin sensation preserved
🔴 TOPIC 6: MUSCLES OF HAND — INNERVATION ⭐⭐⭐
MEDIAN nerve (recurrent branch) innervates:
THENAR muscles (3):
├── Abductor Pollicis Brevis
├── Opponens Pollicis ★
└── Flexor Pollicis Brevis (superficial head)
+ Lateral 2 LUMBRICALS (index + middle)
ULNAR nerve (deep branch) innervates:
HYPOTHENAR muscles (3):
├── Abductor Digiti Minimi
├── Opponens Digiti Minimi
└── Flexor Digiti Minimi Brevis
+ All INTEROSSEI (7)
+ Adductor Pollicis ★★
+ Medial 2 LUMBRICALS (ring + little)
RADIAL nerve:
→ ONLY skin on dorsolateral hand (no intrinsic muscles)
INTEROSSEI mnemonic:
DAB = Dorsal ABduct (4 muscles)
PAD = Palmar ADduct (3 muscles)
All = ULNAR nerve
═══════════════════════════════
PART 2 — LOWER LIMB
═══════════════════════════════
🔵 TOPIC 7: LUMBOSACRAL PLEXUS — OVERVIEW ⭐⭐⭐
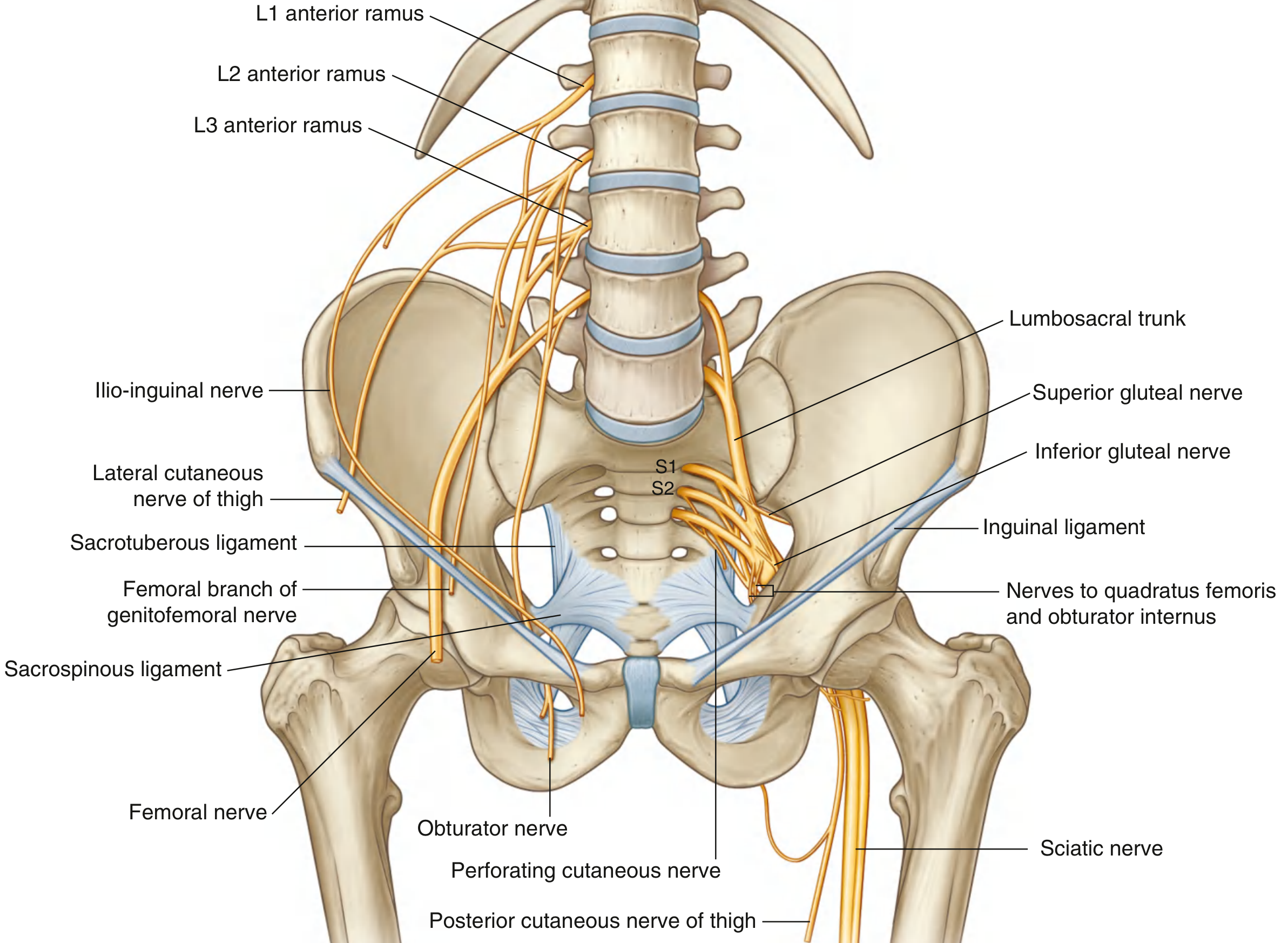
Branches of the Lumbosacral Plexus (Gray's Anatomy for Students)
FLOWCHART: Lower Limb Nerves — Origin and Distribution
LUMBAR PLEXUS (L1–L4):
├── Iliohypogastric (L1)
├── Ilio-inguinal (L1) → medial upper thigh + perineum skin
├── Genitofemoral (L1,L2) → femoral branch → upper central thigh skin
├── Lateral cutaneous nerve of thigh (L2,L3) → lateral thigh
├── FEMORAL nerve (L2–L4) ——→ anterior compartment thigh
│ (passes lateral to femoral artery, OUTSIDE femoral sheath)
└── OBTURATOR nerve (L2–L4) ——→ medial compartment thigh
LUMBOSACRAL TRUNK (L4,L5) + SACRAL PLEXUS (S1–S4):
├── SCIATIC nerve (L4–S3) → posterior thigh + ALL leg + foot
│ ├── Tibial division (ant. rami L4–S3)
│ └── Common fibular division (post. rami L4–S2)
├── Superior gluteal (L4–S1) → above piriformis → Glut med, min, TFL
├── Inferior gluteal (L5–S2) → below piriformis → Gluteus maximus
└── Pudendal (S2–S4) → perineum
🔵 TOPIC 8: GREATER SCIATIC FORAMEN — PIRIFORMIS RULE ⭐⭐⭐
FLOWCHART: What passes through Greater Sciatic Foramen
GREATER SCIATIC FORAMEN
│
PIRIFORMIS muscle divides it:
│
├── ABOVE PIRIFORMIS:
│ • Superior gluteal nerve + artery + vein
│
└── BELOW PIRIFORMIS: (SIP-OQ-P)
• SCIATIC nerve ★
• Inferior gluteal nerve + vessels
• Posterior cutaneous nerve of thigh
• Pudendal nerve → then exits via LESSER sciatic foramen
• Nerve to Obturator internus + gemellus superior
• Nerve to Quadratus femoris + gemellus inferior
• Internal pudendal vessels
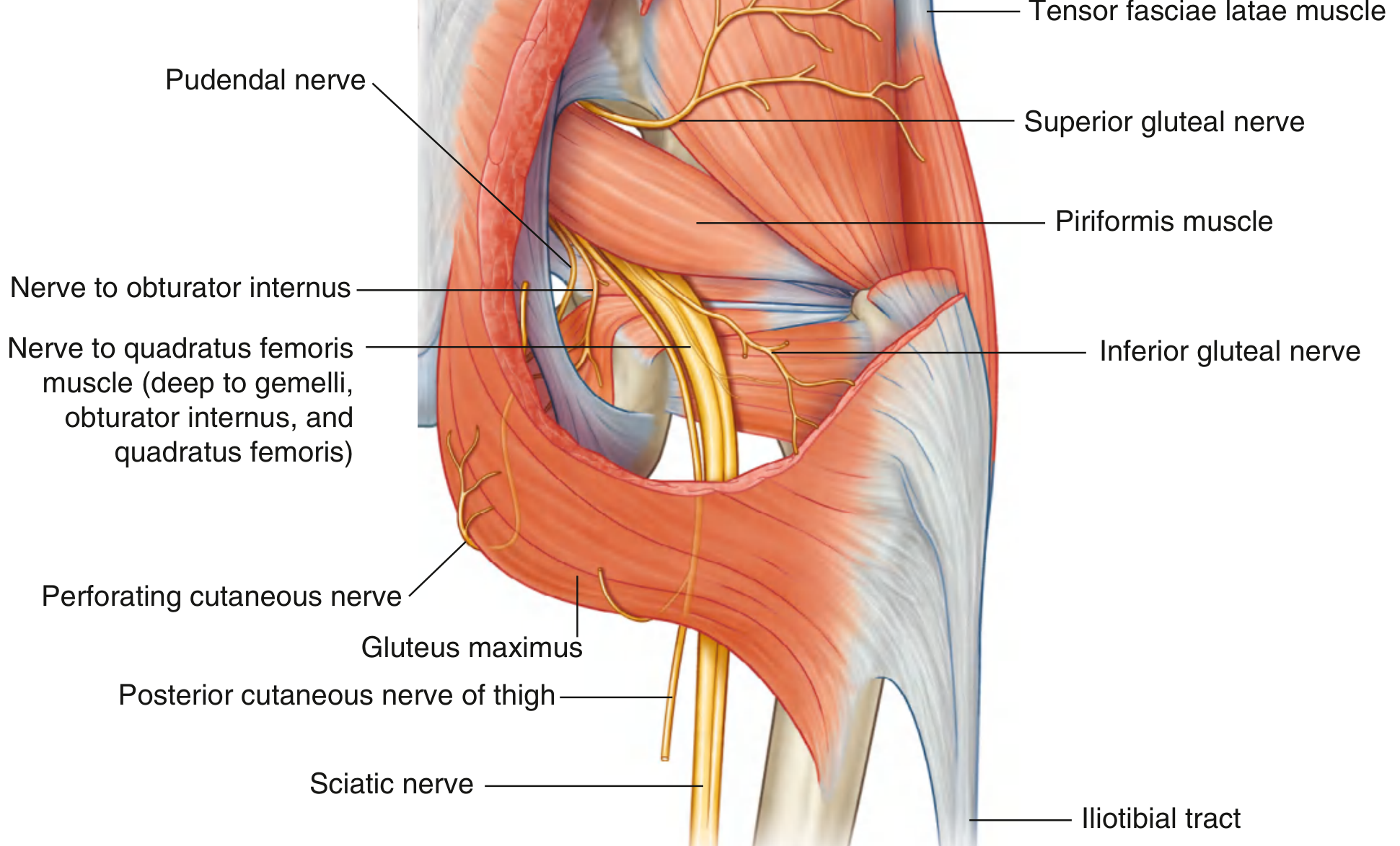
Gluteal Region Nerves (Gray's Anatomy Image)
Nerves of the Gluteal Region — Superior gluteal nerve (above piriformis), Sciatic + all others (below piriformis)
🔴 PYQs — Gluteal Region
Q (INICET 2021): Which nerve is tested in Trendelenburg sign?
A: Superior gluteal nerve (L4–S1) — supplies gluteus medius + minimus ✅
Q: Trendelenburg sign is positive when?
A: When patient stands on affected limb, pelvis drops on the opposite (swing) side — weak hip abductors (gluteus medius/minimus) ✅
Q (INICET 2022): Safest quadrant for intramuscular injection in gluteal region?
A: Anterior corner of the upper outer quadrant (avoids sciatic nerve and superior gluteal neurovascular bundle) ✅
Q: Which nerve exits above piriformis?
A: Superior gluteal nerve ✅ (All others exit below)
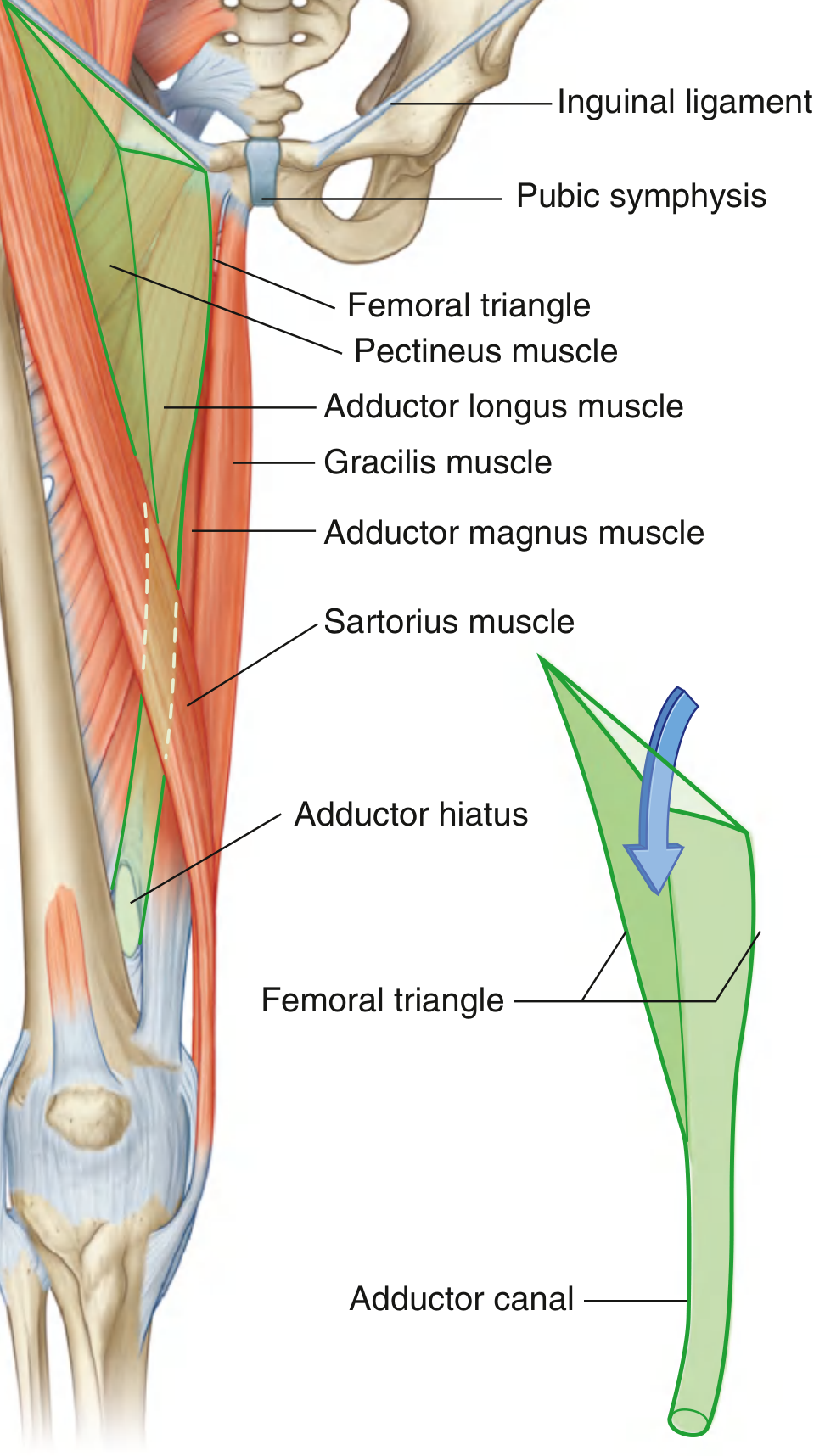
🔵 TOPIC 9: FEMORAL TRIANGLE & ADDUCTOR CANAL ⭐⭐⭐
Femoral Triangle boundaries and continuation into Adductor Canal (Hunter's canal)
FLOWCHART: Femoral Triangle
FEMORAL TRIANGLE — Anteromedial thigh
┌─────────────────────────────────────┐
│ BASE (superior): Inguinal ligament│
│ MEDIAL border: Adductor longus │
│ LATERAL border: Sartorius │
│ FLOOR: Iliopsoas (lat) + │
│ Pectineus (med) │
│ ROOF: Fascia lata + skin │
└─────────────────────────────────────┘
CONTENTS (Lateral → Medial): NAVY
N – Femoral NERVE (lateral, OUTSIDE femoral sheath)
A – Femoral ARTERY (midpoint between ASIS + pubic symphysis)
V – Femoral VEIN
Y – Lymphatics (femoral canal = most medial compartment of sheath)
FEMORAL SHEATH contains: Artery + Vein + Lymphatics
(NOT the femoral nerve)
FEMORAL CANAL: most medial compartment → site of femoral hernia
FLOWCHART: Adductor Canal (Hunter's Canal)
ADDUCTOR CANAL (middle third of thigh):
Roof: Sartorius muscle
Medial: Adductor longus + Adductor magnus
Lateral: Vastus medialis
CONTENTS:
├── Femoral artery (→ becomes popliteal at adductor hiatus)
├── Femoral vein
├── Saphenous nerve (sensory branch of femoral)
└── Nerve to vastus medialis
Ends at: ADDUCTOR HIATUS in adductor magnus
→ femoral vessels become popliteal vessels
🔴 PYQs — Femoral Triangle
Q: Femoral nerve relation to femoral artery in femoral triangle?
A: Femoral nerve is LATERAL to artery and is OUTSIDE the femoral sheath ✅
Q: Which structure is most medial in the femoral triangle?
A: Femoral canal (containing lymphatics) ✅ — site of femoral hernia
Q: Femoral artery pulse is felt at?
A: Midpoint of inguinal ligament (mid-inguinal point) — halfway between ASIS and pubic symphysis ✅
🔵 TOPIC 10: SCIATIC NERVE ⭐⭐⭐
FLOWCHART: Sciatic Nerve Course and Branches
SCIATIC NERVE (L4–S3) — Largest nerve in body
│
├── Exits pelvis through GREATER SCIATIC FORAMEN below piriformis
├── Lies at midpoint between ischial tuberosity and greater trochanter
├── Passes through posterior thigh
│
Divides into (usually at apex of popliteal fossa):
│
├── TIBIAL NERVE (ant. divisions L4–S3)
│ • Motor: All posterior thigh muscles (hamstrings)
│ ALL leg + foot muscles
│ • Sensory: Sole of foot + lateral foot
│ • Injury → CALCANEOVALGUS FOOT (loss of plantarflexion)
│ Loss of sensation sole
│
└── COMMON FIBULAR (PERONEAL) NERVE (post. divisions L4–S2)
• Winds around NECK OF FIBULA ← most vulnerable site
• Divides into:
├── Superficial fibular → fibularis longus + brevis (eversion)
│ Sensory: lateral leg + dorsum of foot
└── Deep fibular → anterior compartment (dorsiflexion)
Sensory: 1st web space
• Injury at fibula neck → FOOT DROP (cannot dorsiflex)
→ Sensory loss dorsum foot
→ Steppage gait
🔴 PYQs — Sciatic/Common Peroneal Nerve
Q (NEET PG, multiple years): Most common nerve injured at proximal fibula?
A: Common peroneal (fibular) nerve ✅
Q: Common peroneal nerve injury causes?
A: Foot drop + sensory loss dorsum of foot + steppage gait ✅
Q: Tibial nerve injury causes?
A: Calcaneovalgus foot — cannot plantarflex; loss of sensation over sole ✅
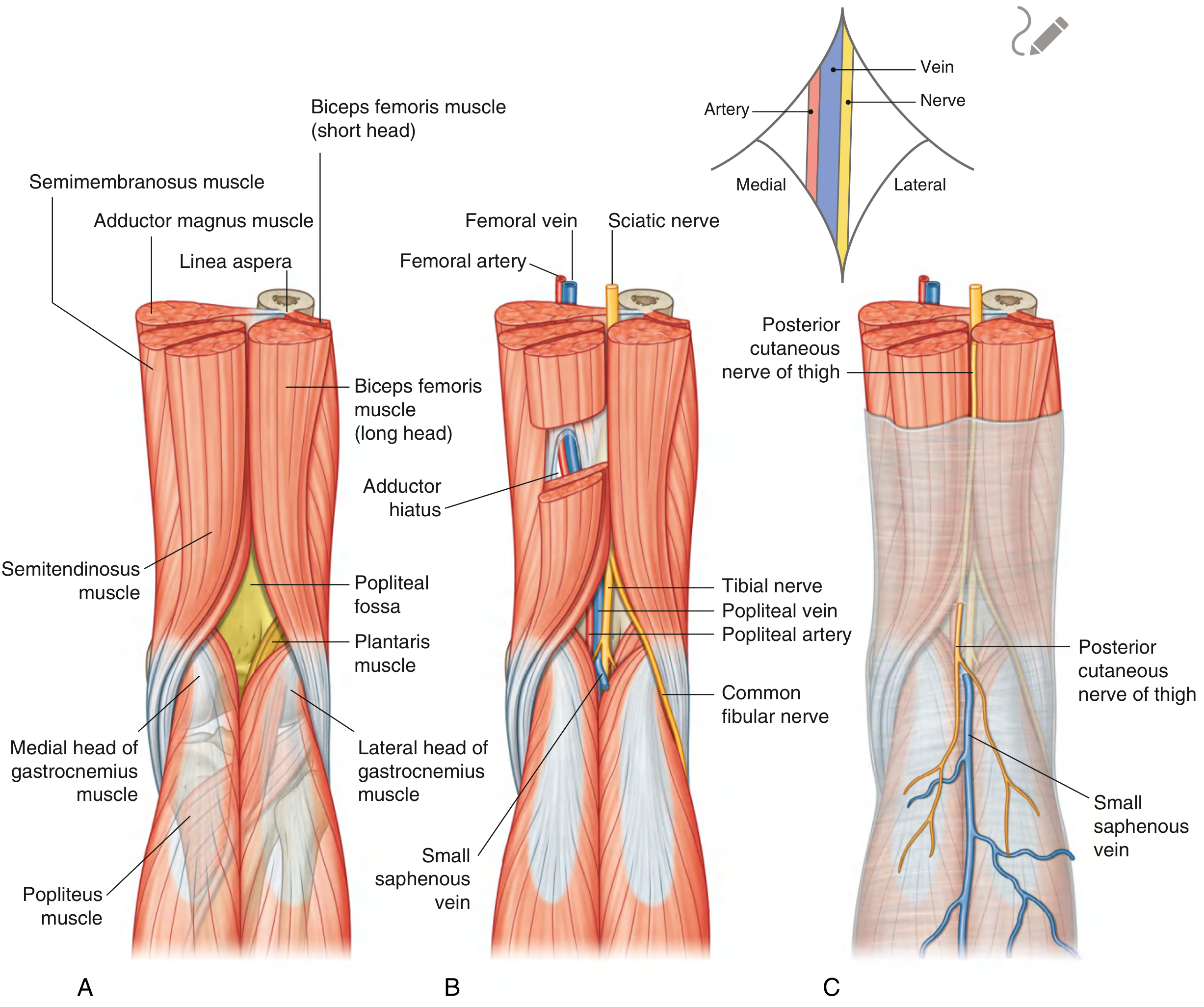
🔵 TOPIC 11: POPLITEAL FOSSA ⭐⭐
Popliteal Fossa: (A) Boundaries (B) Neurovascular contents — Tibial nerve, Popliteal artery, Common fibular nerve
FLOWCHART: Popliteal Fossa
POPLITEAL FOSSA — Diamond-shaped space behind knee
┌────────────────────────────────────────────┐
│ UPPER MEDIAL border: Semitendinosus + │
│ Semimembranosus │
│ UPPER LATERAL border: Biceps femoris │
│ LOWER MEDIAL border: Medial head gastrocnem│
│ LOWER LATERAL: Lateral gastrocnemius + │
│ Plantaris │
│ FLOOR: Femur (popliteal surface) + capsule │
│ of knee joint + Popliteus │
│ ROOF: Deep fascia (fascia lata cont.) │
└────────────────────────────────────────────┘
CONTENTS (Superficial → Deep):
1. TIBIAL NERVE (most superficial/posterior)
2. Popliteal VEIN (middle)
3. Popliteal ARTERY (deepest — most anterior)
[Mnemonic: TAN = Tibial-Artery-Nerve, deep to superficial]
4. Common FIBULAR nerve (leaves laterally, follows biceps femoris tendon)
5. Small saphenous vein (enters fossa piercing deep fascia)
Popliteal artery = continuation of femoral artery through adductor hiatus
Bifurcates → Anterior + Posterior tibial arteries
Key clinical: Popliteal artery aneurysm/injury in posterior knee dislocation → most common peripheral arterial aneurysm
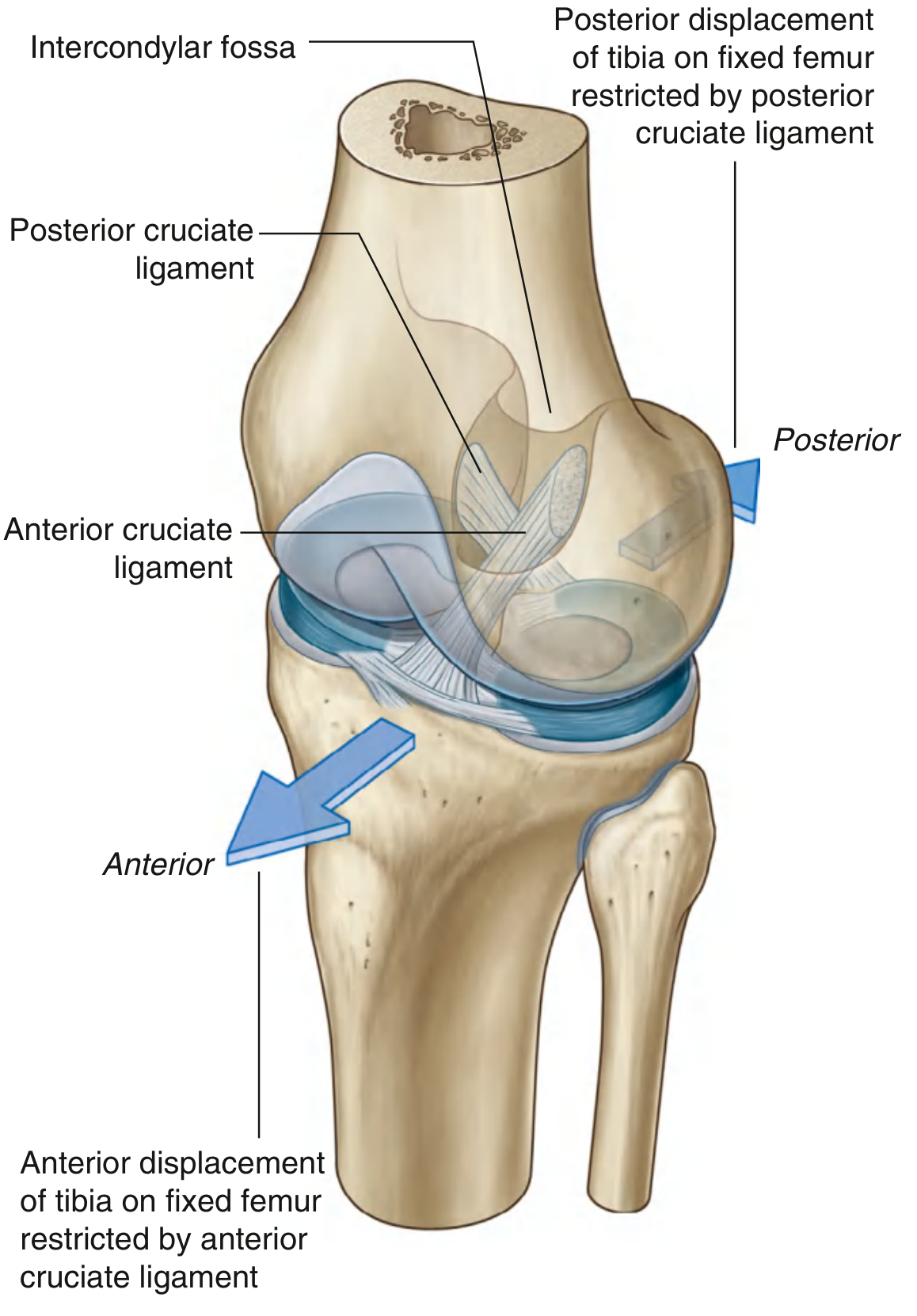
🔵 TOPIC 12: KNEE JOINT ⭐⭐⭐
Cruciate Ligaments — ACL prevents anterior tibial displacement; PCL prevents posterior displacement
FLOWCHART: Knee Joint Ligaments
KNEE JOINT (largest joint; compound synovial — hinge + pivot)
CRUCIATE LIGAMENTS (inside joint, extrasynovial):
ACL: Tibia (anterior) → Femur (lateral wall, intercondylar fossa)
Function: PREVENTS ANTERIOR displacement of tibia
Test: Anterior Drawer test, Lachman test
Blood supply: Middle genicular artery
PCL: Tibia (posterior) → Femur (medial wall, intercondylar fossa)
Function: PREVENTS POSTERIOR displacement of tibia
Test: Posterior Drawer test
Stronger than ACL
COLLATERAL LIGAMENTS:
MCL (Medial): Femur → Tibia
Attached to medial meniscus → MCL tear often tears medial meniscus
Test: Valgus stress test
LCL (Lateral): Femur → Fibula head
NOT attached to lateral meniscus
Test: Varus stress test
"UNHAPPY TRIAD" (O'Donoghue): ACL + MCL + Medial meniscus
(caused by lateral blow to extended knee)
LOCKING MECHANISM:
Knee extends → femoral surfaces become broader → stability ↑
Final extension → medial rotation of femur (screws home)
UNLOCKING: Popliteus muscle → lateral rotation of femur
🔴 PYQs — Knee
Q (INICET 2023): Unhappy triad of O'Donoghue involves?
A: ACL + MCL + Medial meniscus ✅
Q: Which ligament prevents anterior displacement of tibia?
A: ACL (Anterior Cruciate Ligament) ✅
Q: Which muscle unlocks the knee?
A: Popliteus — initiates lateral rotation of femur ✅
Q (INICET 2022): Ligament injury in valgus stress?
A: MCL (Medial Collateral Ligament) ✅
🔵 TOPIC 13: HIP JOINT & FEMORAL NECK FRACTURE ⭐⭐
FLOWCHART: Blood Supply of Femoral Head
BLOOD SUPPLY OF FEMORAL HEAD (3 sources):
1. Vessels in RETINACULA of fibrous capsule (most important in adults)
← Come from medial + lateral circumflex femoral arteries
← TRANSECTED in fracture of femoral neck → AVN
2. Artery in LIGAMENT OF HEAD of femur (ligamentum teres)
← From obturator artery
← Attenuates with age (often non-functional in elderly)
3. Vessels in MEDULLARY CAVITY
← Attenuate with fatty replacement in elderly
FRACTURE OF NECK OF FEMUR:
├── Intracapsular fracture → Retinacular vessels CUT → HIGH risk of AVN
└── Intertrochanteric fracture → Retinacular vessels INTACT → Lower AVN risk
→ Can be fixed (not need hemiarthroplasty)
Lower Limb Nerve Injury Summary Table
| Nerve | Root | Injury Site | Deformity/Sign | Sensory Loss |
|---|
| Femoral | L2–L4 | Inguinal region/pelvic fracture | Loss of knee extension; weak hip flexion | Anterior thigh, medial leg |
| Obturator | L2–L4 | Obturator canal/pelvic fracture | Weak thigh adduction | Upper medial thigh |
| Sciatic | L4–S3 | Gluteal region/posterior hip dislocation | Combined tibial + peroneal loss | Posterior thigh + all of leg/foot |
| Common Fibular | L4–S2 | Neck of fibula (most common) | Foot drop, steppage gait | Dorsum of foot, lateral leg |
| Tibial | L4–S3 | Popliteal fossa | Calcaneovalgus foot; loss of plantarflexion | Sole of foot |
| Superior gluteal | L4–S1 | Greater sciatic foramen (above piriformis) | Trendelenburg sign (+) | None |
| Inferior gluteal | L5–S2 | Greater sciatic foramen (below piriformis) | Weak hip extension; gluteus maximus wasting | None |
| Lateral femoral cutaneous | L2,L3 | Under/through inguinal ligament near ASIS | No motor loss; Meralgia paresthetica | Lateral thigh |
═══════════════════════════════
PART 3 — INTEGRATED PYQ BANK
NEET PG & INICET 2021–2025
═══════════════════════════════
✅ Quick-Fire Q&A (All Previously Asked)
| Q | A | Year |
|---|
| Long head triceps — origin? | Infraglenoid tubercle | NEET PG 2025 |
| Which nerve passes through quadrangular space? | Axillary nerve | INICET 2022 |
| Winged scapula — nerve? | Long thoracic (C5–C7) | INICET 2023 |
| Erb palsy deformity? | Waiter's tip (C5, C6) | INICET 2021 |
| Klumpke associated with? | Horner syndrome (T1) | INICET 2021 |
| Ulnar nerve injury at wrist — worse claw? | Yes — ulnar paradox | INICET 2022 |
| Froment sign tests? | Ulnar nerve (adductor pollicis) | INICET 2022 |
| Carpal tunnel contents? | 4 FDS + 4 FDP + FPL + Median nerve | INICET 2023 |
| Spared in carpal tunnel syndrome? | Palmar branch of median nerve | INICET 2023 |
| Thenar muscles nerve? | Recurrent branch of median nerve | INICET 2020 |
| All intrinsic muscles except thenar + 2 lumbricals? | Ulnar nerve | INICET 2020 |
| DAB / PAD — interossei? | Dorsal ABduct / Palmar ADduct | INICET 2020 |
| Rotator cuff muscles? | SITS | INICET 2021 |
| Supraspinatus — nerve? | Suprascapular (C5,C6) | INICET 2021 |
| Nerve above piriformis? | Superior gluteal nerve | INICET 2022 |
| Nerve below piriformis (all of them)? | Sciatic, Inf gluteal, PCNT, Pudendal, N.OI, N.QF | INICET 2022 |
| Trendelenburg sign — nerve? | Superior gluteal (L4–S1) | INICET 2021 |
| Trendelenburg sign: pelvis drops to which side? | Opposite (swing) side | INICET 2021 |
| Most common nerve at fibula neck? | Common peroneal (fibular) nerve | NEET PG (multiple) |
| Common peroneal injury → ? | Foot drop + dorsal foot sensory loss | NEET PG |
| Femoral nerve relation to sheath? | Lateral to femoral artery, OUTSIDE femoral sheath | INICET 2022 |
| Femoral canal — most medial compartment? | Contains lymphatics; site of femoral hernia | INICET 2022 |
| Adductor canal = ? | Hunter's/Subsartorial canal | INICET 2022 |
| Popliteal fossa — deepest structure? | Popliteal artery | NEET PG |
| ACL prevents? | Anterior displacement of tibia | INICET 2023 |
| PCL prevents? | Posterior displacement of tibia | INICET 2023 |
| Unhappy triad? | ACL + MCL + Medial meniscus | INICET 2023 |
| Muscle that unlocks the knee? | Popliteus | NEET PG |
| AVN of femoral head — fracture type? | Intracapsular (femoral neck) fracture | NEET PG |
| Scaphoid fracture — tenderness where? | Anatomical snuffbox | NEET PG |
| Radial groove fracture → ? | Wrist drop (radial nerve) | NEET PG |
INICET High-Yield Topic List (2020–2023 Confirmed)
| Year | Upper Limb | Lower Limb |
|---|
| 2020 | Joints of UL; Muscles of hand; Collagen fibres | Muscles of gluteal region; Vertebral landmarks |
| 2021 | Rotator cuff; Ulnar nerve; Nerve injuries UL; Muscles of hand | Trendelenburg; Nerve injuries UL/LL; Ulnar nerve |
| 2022 | Nerve injuries UL; Ulnar nerve; Joints of UL | Femoral triangle; Nerve injuries LL; Ulnar nerve |
| 2023 | Brachial plexus; Muscles of hand; Ligaments UL | Musculoskeletal/nerve supply; Knee joint |
Sources: Gray's Anatomy for Students | THIEME Atlas of General Anatomy & Musculoskeletal System | The Harriet Lane Handbook 23rd Ed. | Miller's Review of Orthopaedics 9th Ed. | Harrison's Principles of Internal Medicine 22nd Ed.