Clinical cases of acid base balance biochemistry for MBBS exams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed to write a thorough, exam-focused response. Let me compile everything.
Acid-Base Balance: Clinical Cases for MBBS Biochemistry Exams
Quick Reference: Normal ABG Values
| Parameter | Normal Value |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mmHg |
| HCO3- | 22 - 26 mmol/L |
| PaO2 | 80 - 100 mmHg |
| Anion Gap (AG) | 8 - 12 mEq/L |
Anion Gap formula: AG = Na+ - (Cl- + HCO3-)
Step-by-Step Approach to ABG Analysis
(Harrison's Principles of Internal Medicine 22E, Table 58-3)
- Draw ABG and serum electrolytes simultaneously
- Check that the calculated HCO3- (on ABG) matches measured HCO3- (on electrolyte panel) within ±2 mmol/L
- Calculate the Anion Gap; correct for hypoalbuminemia
- Identify high-AG or normal-AG pattern
- Apply the compensation formula (Table below)
- Compare delta values (ΔAG vs ΔHCO3-) to detect mixed disorders
Compensation Formulas (MUST MEMORISE)
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic acidosis | ΔPaCO2 = 1.3 × ΔHCO3- (Winter's formula: PCO2 = 1.5×HCO3- + 8 ± 2) |
| Metabolic alkalosis | ΔPaCO2 = 0.6 × ΔHCO3- |
| Respiratory acidosis (acute) | HCO3- rises by 1 mmol/L per 10 mmHg ↑ CO2 |
| Respiratory acidosis (chronic) | HCO3- rises by 4 mmol/L per 10 mmHg ↑ CO2 |
| Respiratory alkalosis (acute) | HCO3- falls by 2 mmol/L per 10 mmHg ↓ CO2 |
| Respiratory alkalosis (chronic) | HCO3- falls by 5 mmol/L per 10 mmHg ↓ CO2 |
(Roberts and Hedges' Clinical Procedures in Emergency Medicine)
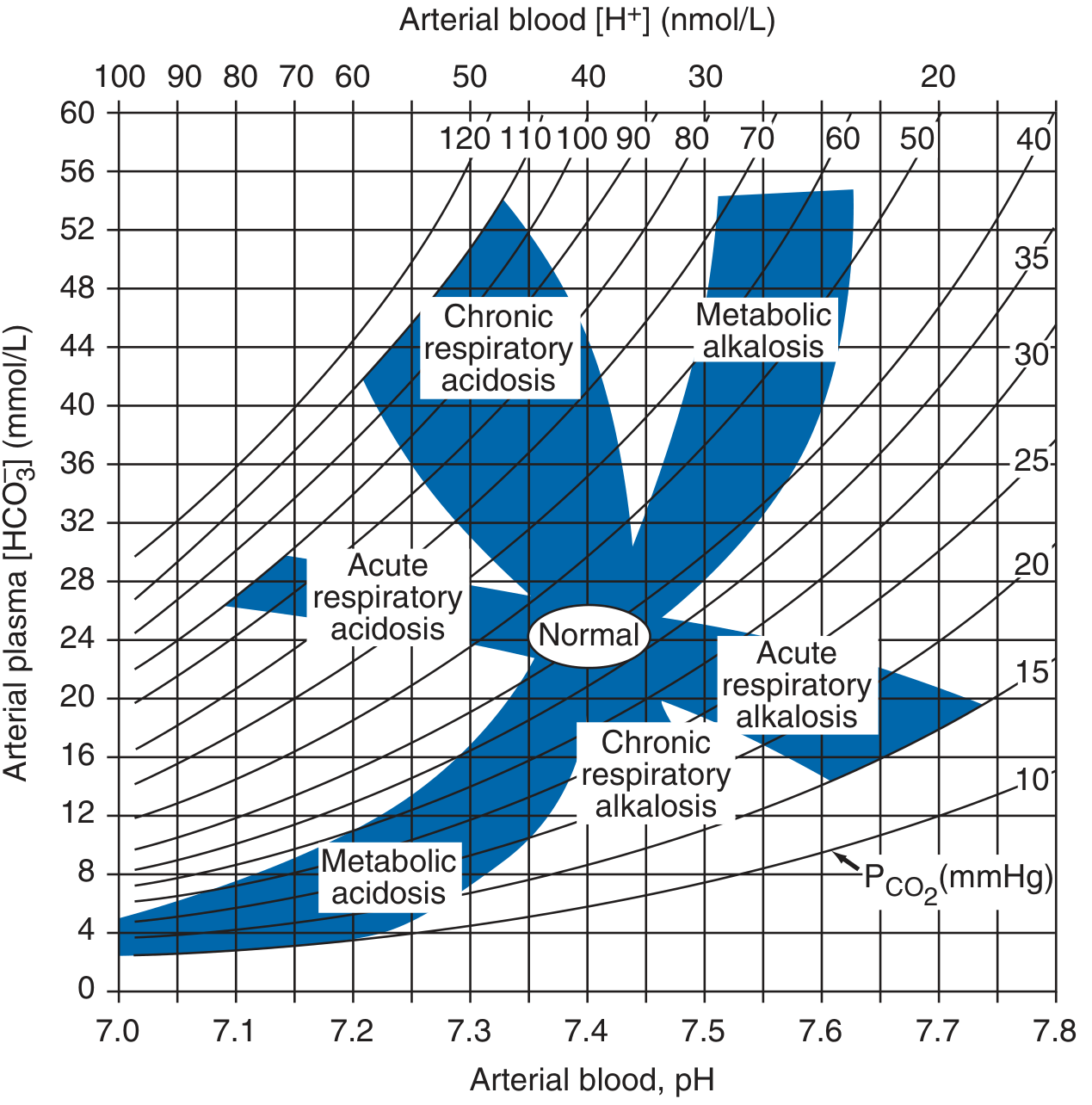
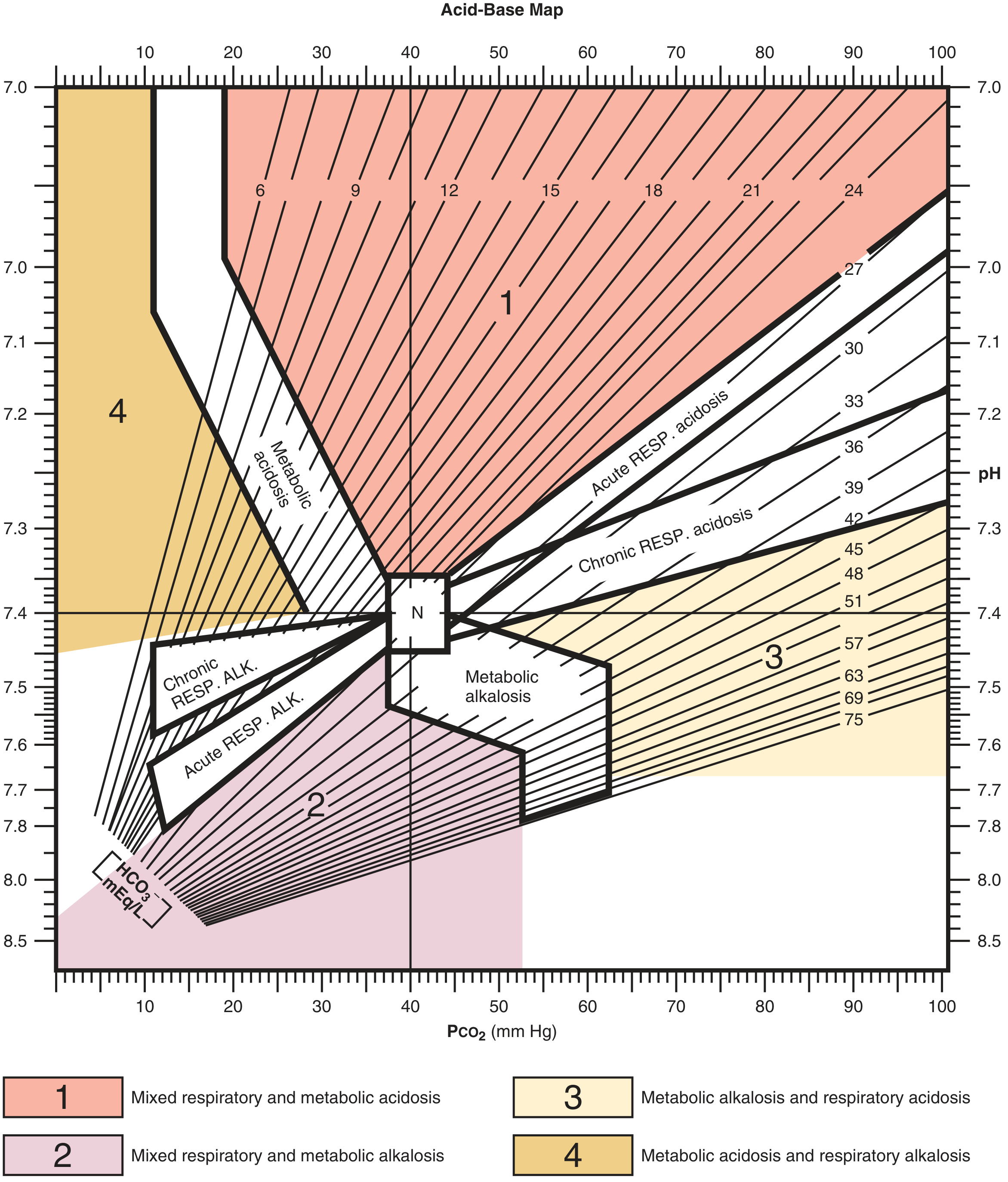
Acid-Base Nomogram
CLINICAL CASE 1 - Metabolic Acidosis (Non-Anion Gap)
Presentation: A 58-year-old woman has had profuse diarrhea for 1 week.
ABG + Electrolytes:
- Na+: 133 | K+: 2.8 | Cl-: 118
- pH: 7.26 | PaCO2: 13 mmHg | HCO3-: 5 mmol/L
Step-by-step analysis:
Step 1 - pH: 7.26 → Acidosis
Step 2 - Primary process: HCO3- is low (5 mmol/L) and PaCO2 is NOT elevated → Metabolic acidosis
Step 3 - Anion Gap: AG = 133 - (118 + 5) = 10 mEq/L → Normal AG (non-anion gap)
Step 4 - Compensation check (Winter's formula):
- Expected PaCO2 = 1.5 × 5 + 8 = 15.5 mmHg (range: 13.5 - 17.5)
- Actual PaCO2 = 13 mmHg → within predicted range
- ✓ Appropriate respiratory compensation; no mixed disorder
Diagnosis: Simple metabolic acidosis (non-anion gap / hyperchloremic) due to diarrhea (HCO3- loss from GI tract)
Key teaching point: Diarrhea causes direct loss of HCO3-, so Cl- rises to maintain electroneutrality → hyperchloremic, normal-AG acidosis. K+ is also low (co-secreted with HCO3- in stool).
CLINICAL CASE 2 - Respiratory Alkalosis (Acute)
Presentation: A 74-year-old nursing home resident admitted with fever (39°C), hypotension (96/70 mmHg), positive blood cultures for E. coli.
ABG + Electrolytes:
- Na+: 138 | K+: 3.2 | Cl-: 105
- pH: 7.49 | PaCO2: 25 mmHg | HCO3-: 22 mmol/L
Step 1 - pH: 7.49 → Alkalosis
Step 2 - Primary process: PaCO2 is low (25 mmHg), HCO3- is NOT elevated → Respiratory alkalosis
Step 3 - Compensation check:
- PaCO2 drop = 40 - 25 = 15 mmHg
- Expected HCO3- fall (acute) = 2 mmol/L per 10 mmHg drop → 15/10 × 2 = 3 mmol/L
- Expected HCO3- = 25 - 3 = 22 mmol/L
- Actual HCO3- = 22 mmol/L → ✓ Appropriate
Diagnosis: Acute respiratory alkalosis due to sepsis (gram-negative septicemia stimulates the respiratory centre directly via endotoxins and cytokines, causing hyperventilation)
Key teaching point: Sepsis is one of the most common causes of respiratory alkalosis. The HCO3- has not yet had time to fall renally (renal compensation takes 3-5 days), confirming this is acute.
CLINICAL CASE 3 - Metabolic Acidosis with High Anion Gap (DKA)
Presentation: A 22-year-old type 1 diabetic female, vomiting, Kussmaul breathing, fruity breath odour, drowsy.
ABG + Electrolytes:
- Na+: 136 | K+: 5.5 | Cl-: 98
- pH: 7.10 | PaCO2: 18 mmHg | HCO3-: 6 mmol/L
Step 1 - pH: 7.10 → Severe acidosis
Step 2 - Primary process: HCO3- markedly low → Metabolic acidosis
Step 3 - Anion Gap: AG = 136 - (98 + 6) = 32 mEq/L → High AG (normal = 10-12)
Step 4 - Winter's formula:
- Expected PaCO2 = 1.5 × 6 + 8 = 17 mmHg (range: 15-19)
- Actual PaCO2 = 18 mmHg → ✓ Appropriate respiratory compensation (Kussmaul breathing)
Step 5 - Delta-delta ratio (to check for hidden disorders):
- ΔAG = 32 - 10 = 22
- ΔHCO3- = 25 - 6 = 19
- ΔAG / ΔHCO3- ≈ 1.16 → between 1-2, consistent with pure high-AG acidosis
Diagnosis: High-AG metabolic acidosis from diabetic ketoacidosis (acetoacetate + β-hydroxybutyrate accumulate)
High-AG acidosis mnemonics: MUDPILES or KULT
- Ketoacidosis (DKA, AKA, starvation)
- Uremia (chronic kidney failure)
- Lactic acidosis (sepsis, shock, metformin)
- Toxins (methanol, ethylene glycol, salicylates, propylene glycol)
CLINICAL CASE 4 - Mixed Disorder: Metabolic Acidosis + Respiratory Alkalosis
Presentation: 35-year-old found unresponsive, tinnitus, hyperventilation. Suspected aspirin overdose.
ABG + Electrolytes:
- Na+: 140 | K+: 4.0 | Cl-: 106
- pH: 7.39 | PaCO2: 24 mmHg | HCO3-: 14 mmol/L | AG: 20
Step 1 - pH: 7.39 → Near-normal (misleadingly)
Step 2 - AG: AG = 140 - (106 + 14) = 20 → High-AG metabolic acidosis present
Step 3 - Compensation check:
- For pure metabolic acidosis (HCO3- = 14), expected PaCO2 = 1.5 × 14 + 8 = 29 mmHg
- Actual PaCO2 = 24 mmHg → Lower than expected
Diagnosis: Mixed high-AG metabolic acidosis + respiratory alkalosis
Key: The salicylate stimulates the respiratory centre directly → additional hyperventilation beyond what metabolic acidosis alone would produce → pH near normal despite both disorders being present.
(Harrison's 22E - Table 3-2: mixed metabolic acidosis-respiratory alkalosis, etiology: lactic acidosis/sepsis/salicylates)
CLINICAL CASE 5 - Metabolic Alkalosis (Vomiting)
Presentation: A 30-year-old woman with persistent vomiting for 4 days (pyloric stenosis). Muscle cramps, tetany.
ABG + Electrolytes:
- Na+: 138 | K+: 2.8 | Cl-: 82
- pH: 7.58 | PaCO2: 48 mmHg | HCO3-: 42 mmol/L
Step 1 - pH: 7.58 → Alkalosis
Step 2 - Primary process: HCO3- is markedly elevated → Metabolic alkalosis
Step 3 - Compensation check:
- For metabolic alkalosis, expected ΔPaCO2 = 0.6 × ΔHCO3- = 0.6 × (42 - 25) = 10.2 mmHg
- Expected PaCO2 = 40 + 10 = 50 mmHg (range: 48-52)
- Actual PaCO2 = 48 mmHg → ✓ Appropriate hypoventilation
Diagnosis: Metabolic alkalosis due to vomiting (loss of HCl from gastric acid → net gain of HCO3-)
Key teaching points:
- Vomiting = loss of H+ and Cl- → hypochloremic, hypokalemic metabolic alkalosis
- Cl- depletion prevents renal correction (kidney retains HCO3- to accompany Na+ when Cl- is low)
- Tetany/cramps occur because alkalosis causes decreased ionized Ca2+ (Ca2+ binds more to albumin at high pH)
CLINICAL CASE 6 - Respiratory Acidosis (COPD with Compensation)
Presentation: 65-year-old chronic smoker, COPD. Gradually worsening breathlessness, plethoric, drowsy.
ABG + Electrolytes:
- Na+: 140 | K+: 3.5 | Cl-: 88
- pH: 7.35 | PaCO2: 65 mmHg | HCO3-: 35 mmol/L
Step 1 - pH: 7.35 → Low-normal (acidosis compensated)
Step 2 - Primary process: PaCO2 is elevated → Respiratory acidosis
Step 3 - Compensation check:
- PaCO2 rise = 65 - 40 = 25 mmHg
- For chronic respiratory acidosis: HCO3- rises by 4 mmol/L per 10 mmHg ↑ CO2
- Expected ΔHC03- = (25/10) × 4 = 10 mmol/L; expected HCO3- = 25 + 10 = 35 mmol/L
- Actual HCO3- = 35 mmol/L → ✓ Fully compensated chronic respiratory acidosis
Diagnosis: Fully compensated chronic respiratory acidosis (Type 2 respiratory failure in COPD)
Key teaching point: The renal compensation (↑HCO3-) here is complete, which distinguishes chronic from acute respiratory acidosis. The pH is near-normal despite very high CO2.
CLINICAL CASE 7 - Mixed Disorder: Metabolic Alkalosis + Respiratory Acidosis (COPD + Diuretics)
Presentation: 70-year-old with COPD on long-term furosemide for cor pulmonale.
ABG + Electrolytes:
- Na+: 140 | K+: 3.5 | Cl-: 88
- pH: 7.42 | PaCO2: 67 mmHg | HCO3-: 42 mmol/L | AG: 10
Step 1 - pH: 7.42 → Normal, yet both PaCO2 and HCO3- are clearly abnormal. This is a red flag for a mixed disorder.
Step 2 - Primary processes:
- PaCO2 = 67 → Respiratory acidosis
- HCO3- = 42 → Metabolic alkalosis
- Both processes push pH in opposite directions → pH is deceptively normal
Diagnosis: Mixed metabolic alkalosis + respiratory acidosis
(Harrison's 22E - example from Table 3-2: COPD patient on diuretics)
Key teaching point: A normal pH does not rule out acid-base disorder. When PaCO2 and HCO3- move in the same direction (both elevated or both low), always suspect a mixed disorder. Furosemide causes urinary Cl- and K+ loss → contraction alkalosis → metabolic alkalosis superimposed on chronic respiratory acidosis.
CLINICAL CASE 8 - High-AG Metabolic Acidosis (Uremia)
Presentation: 55-year-old with known chronic kidney disease (CKD stage 5), on dialysis missed last 3 sessions, nausea, drowsy.
ABG + Electrolytes:
- Na+: 135 | K+: 6.2 | Cl-: 98
- pH: 7.22 | PaCO2: 22 mmHg | HCO3-: 9 mmol/L | AG: 28
Step 1 - pH: 7.22 → Severe acidosis
Step 2 - Primary process: HCO3- markedly low → Metabolic acidosis
Step 3 - AG: 135 - (98+9) = 28 → High-AG
Step 4 - Compensation (Winter's formula):
- Expected PaCO2 = 1.5 × 9 + 8 = 21.5 mmHg (range: 19.5-23.5)
- Actual PaCO2 = 22 mmHg → ✓ Appropriate
Diagnosis: High-AG metabolic acidosis from uremic acidosis (accumulated phosphate, sulfate, organic acids)
Key teaching point: In uraemia, non-metabolizable anions accumulate. Unlike DKA where ketones can be metabolized back to HCO3-, uremic anions cannot. Hence bicarbonate therapy is appropriate here (aim for HCO3- of 22 mmol/L). Hyperkalemia occurs because acidosis shifts K+ extracellularly.
Summary Table of All Cases
| Case | pH | PaCO2 | HCO3- | AG | Diagnosis | Classic Cause |
|---|---|---|---|---|---|---|
| 1 | ↓ | ↓ (comp.) | ↓↓ | Normal | Metabolic acidosis (non-AG) | Diarrhea |
| 2 | ↑ | ↓↓ | Normal | Normal | Acute respiratory alkalosis | Sepsis |
| 3 | ↓↓ | ↓ (comp.) | ↓↓ | ↑↑ | High-AG metabolic acidosis | DKA |
| 4 | ~Normal | ↓↓ | ↓ | ↑ | Mixed: met. acidosis + resp. alkalosis | Salicylate poisoning |
| 5 | ↑↑ | ↑ (comp.) | ↑↑ | Normal | Metabolic alkalosis | Vomiting (pyloric stenosis) |
| 6 | Low-normal | ↑↑ | ↑ (comp.) | Normal | Compensated chronic resp. acidosis | COPD |
| 7 | Normal | ↑↑ | ↑↑ | Normal | Mixed: met. alkalosis + resp. acidosis | COPD + furosemide |
| 8 | ↓↓ | ↓ (comp.) | ↓↓ | ↑↑ | High-AG metabolic acidosis | Uremia (CKD) |
High-Yield Exam Points
- pH direction tells you the primary disorder - compensation never overcorrects
- Same direction of PaCO2 and HCO3- = mixed disorder (e.g., both high = metabolic alkalosis + respiratory acidosis)
- Normal pH does not mean no disorder - opposite mixed disorders can cancel out the pH
- Winter's formula is key for confirming appropriate compensation in metabolic acidosis
- Anion gap must always be calculated; it often reveals a hidden high-AG acidosis even when total HCO3- looks normal
- Delta-delta ratio (ΔAG/ΔHCO3-) - if >2, a concurrent metabolic alkalosis is hiding; if <1, a concurrent non-AG acidosis is also present
- Causes of High-AG acidosis: MUDPILES (Methanol, Uremia, DKA, Propylene glycol, Iron/Isoniazid, Lactic acidosis, Ethylene glycol, Salicylates)
- Causes of Non-AG acidosis: HARDUPS (Hyperalimentation, Addison's, RTA, Diarrhea, Ureteroenteric fistula, Pancreatic fistula, Saline infusion)
- Respiratory compensation is fast (minutes to hours); renal compensation is slow (3-5 days) - this determines acute vs. chronic status
- Hypokalemia + metabolic alkalosis = vomiting or diuretics; Hyperkalemia + metabolic acidosis = DKA, renal failure, or Addison's disease
Sources: Harrison's Principles of Internal Medicine 22E (2025); Ganong's Review of Medical Physiology 26th Ed.; Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.