Cephal haematoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Here is the full answer:
Cephalhaematoma
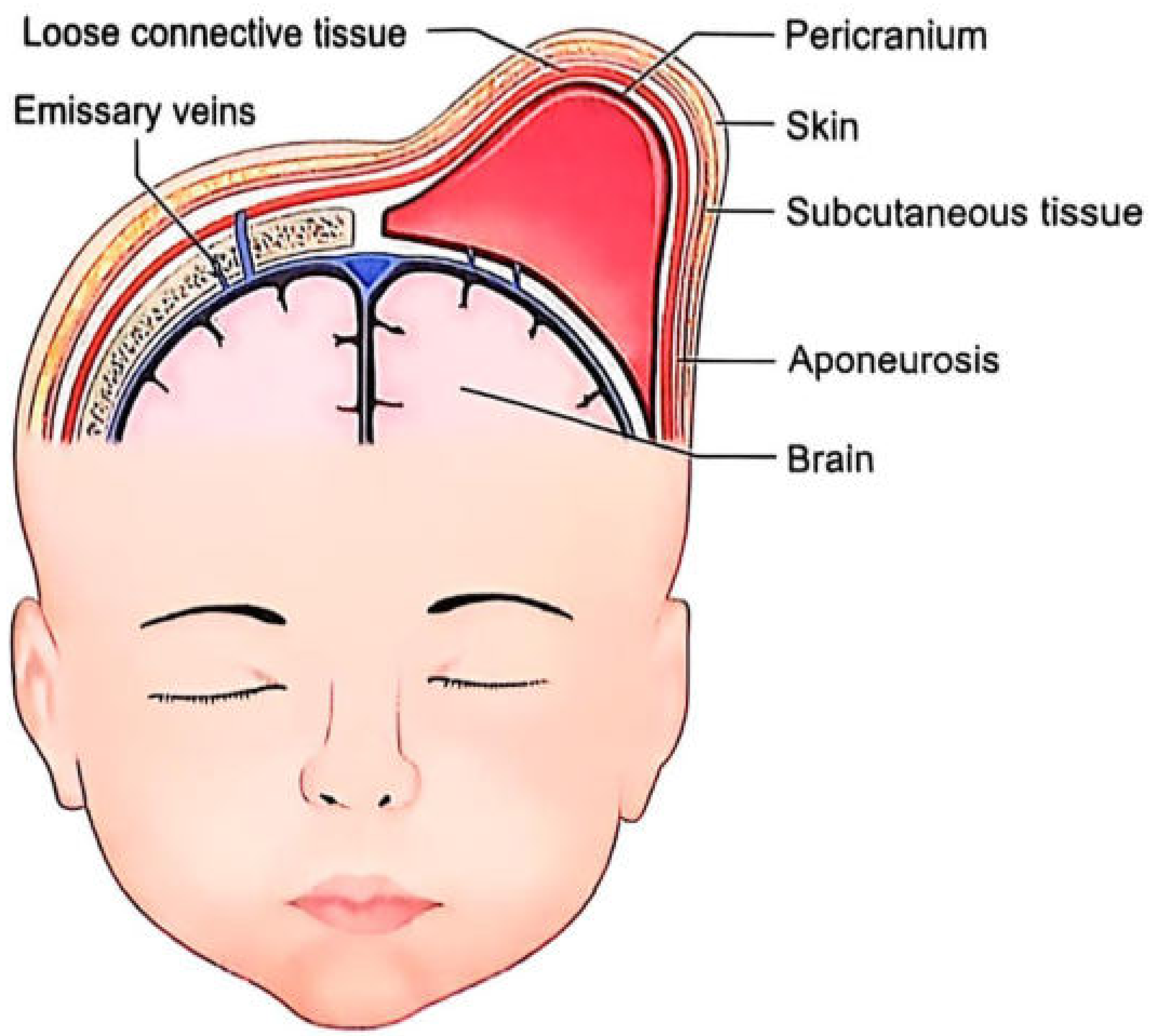
Fig. 19.3: Cephalhaematoma over the right parietal bone - note the blood collection between the pericranium and the outer skull bone surface.
Definition
Cephalhaematoma (also spelled cephalhematoma) is a subperiosteal haemorrhage - a localised accumulation of blood between the periosteum (pericranium) and the outer surface of a skull bone. It is caused by tearing of diploic veins from mechanical trauma during delivery.
- Essentials of Forensic Medicine & Toxicology (2026)
- Bradley and Daroff's Neurology in Clinical Practice
Anatomical Location and Key Feature
The hematoma is confined within the periosteal sheath of a single bone and never crosses a suture line - this is its most important distinguishing feature. The most common bone involved is the right parietal bone. It varies in size from 1 to 5 cm.
The diagram above shows the relevant scalp layers: skin > subcutaneous tissue > aponeurosis > loose connective tissue > pericranium > bone. In cephalhaematoma, blood collects deep to the pericranium but superficial to the bone (subperiosteal plane).
Aetiology / Cause
- Tearing of diploic veins due to mechanical trauma
- Associated with higher birth weight and instrumental delivery (vacuum extraction, forceps)
- Occurs in less than 1% of newborns
Clinical Features
| Feature | Detail |
|---|---|
| Onset | Not evident at birth; appears a few hours after delivery (as blood slowly accumulates) |
| Swelling progression | Tends to increase during the 1st - 2nd day as more blood accumulates |
| Feel | Fluctuant, boggy swelling |
| Limits | Strictly confined to one bone; does not cross sutures |
| Most common site | Right parietal bone |
| Neurological symptoms | Typically absent |
Comparison with Caput Succedaneum
| Feature | Caput Succedaneum | Cephalhaematoma |
|---|---|---|
| Nature | Oedematous swelling (blood + serum) | Pure blood (haematoma) |
| Plane | Above the pericranium (subcutaneous/subaponeurotic) | Below the pericranium (subperiosteal) |
| Crosses sutures? | Yes | No |
| Present at birth? | Yes, immediately | No - appears hours after birth |
| Resolution | 1-7 days | ~2 weeks (Parikh's); weeks to months |
The three extracranial haemorrhage types in order of tissue depth are:
- Caput succedaneum - between skin and epicranial aponeurosis
- Subgaleal haematoma - between aponeurosis and periosteum (most dangerous - can spread under entire scalp and cause haemorrhagic shock)
- Cephalhaematoma - between periosteum and cranial bone (deepest, but confined)
- Bradley and Daroff's Neurology in Clinical Practice
Complications
- Neonatal jaundice (hyperbilirubinaemia) - the degradation of the pooled blood adds to the bilirubin load, worsening physiological jaundice
- Anaemia - from significant blood loss into the haematoma
- Calcification - the haematoma can undergo periosteal ossification if not resorbed, leaving a bony ridge
- Rarely: infection / abscess formation
Forensic Significance
In forensic medicine, the presence of cephalhaematoma is used as one of the signs of live birth and to estimate the length of survival after birth. It shows the usual colour changes of a bruise and disappears in approximately a fortnight (15 days). It indicates the child survived long enough after birth for blood to accumulate subperiosteally, and that mechanical birth trauma occurred.
- PC Dikshit's Textbook of Forensic Medicine and Toxicology
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology
- Essentials of Forensic Medicine & Toxicology (2026)
Management
-
Conservative (watchful waiting) is the standard approach - most resolve spontaneously over weeks to months
-
Do not aspirate (risk of introducing infection)
-
Monitor bilirubin levels (treat jaundice if needed)
-
Monitor for anaemia
-
Neuroimaging if there is concern for underlying skull fracture or intracranial pathology
-
Instrumental deliveries that cause cephalhaematoma warrant postpartum counselling to parents
-
Textbook of Family Medicine 9e
-
Pfenninger and Fowler's Procedures for Primary Care
Hinglish
Cephalhaematoma - Hinglish mein
Definition
Cephalhaematoma ek subperiosteal haemorrhage hai - yaani periosteum (pericranium) aur skull bone ki outer surface ke beech mein blood ka ikatha ho jaana. Yeh delivery ke time mechanical trauma ki wajah se diploic veins ke tear hone se hota hai.
Anatomical Location - Sabse Important Point
Blood ek hi bone ke periosteal sheath ke andar confined rehta hai aur kabhi bhi suture line cross NAHI karta - yeh iska sabse important identifying feature hai.
Scalp ki layers upar se neeche ki taraf:
Skin → Subcutaneous tissue → Aponeurosis → Loose connective tissue → Pericranium → BONE
Cephalhaematoma mein blood pericranium ke neeche, bone ke upar collect hota hai (subperiosteal plane).
- Sabse common site: Right parietal bone
- Size: 1 se 5 cm tak
- Incidence: 1% se kam newborns mein hota hai
Cause (Aetiology)
- Diploic veins ka tear hona - mechanical trauma se
- Instrumental delivery (vacuum, forceps) ke baad zyada common
- High birth weight bhi associated factor hai
Clinical Features
| Feature | Detail |
|---|---|
| Onset | Birth ke time nahi dikhta - kuch ghante baad appear hota hai |
| Swelling | 1st-2nd day mein aur badhti hai jaise jaise blood accumulate hota hai |
| Feel | Fluctuant, boggy (geela-geela sa) |
| Limits | Ek hi bone tak confined - suture cross nahi karta |
| Neurological symptoms | Typically nahi hote |
Caput Succedaneum vs Cephalhaematoma - Comparison Table
| Feature | Caput Succedaneum | Cephalhaematoma |
|---|---|---|
| Nature | Blood + serum ka oedematous swelling | Pure blood (haematoma) |
| Plane | Pericranium ke upar | Pericranium ke neeche (subperiosteal) |
| Suture cross karta hai? | Haan | Nahi |
| Birth ke time present? | Haan, turant | Nahi - ghanton baad |
| Resolution | 1-7 din | ~2 hafte (15 din) |
Teen Extracranial Haemorrhages - Depth ke order mein
- Caput Succedaneum - skin aur aponeurosis ke beech (sabse superficial)
- Subgaleal Haematoma - aponeurosis aur periosteum ke beech (sabse dangerous - poore scalp mein spread ho sakta hai, haemorrhagic shock de sakta hai)
- Cephalhaematoma - periosteum aur bone ke beech (sabse deep, lekin confined)
Complications
- Neonatal Jaundice (Hyperbilirubinaemia) - haematoma mein blood ka breakdown hota hai, bilirubin load badh jaata hai
- Anaemia - significant blood loss hone se
- Calcification - agar absorb na ho to periosteal ossification ho jaati hai, bony ridge ban jaati hai
- Infection/Abscess - rare complication
Forensic Importance
Forensic medicine mein cephalhaematoma live birth ka sign maana jaata hai aur birth ke baad kitna time survival hua yeh estimate karne mein kaam aata hai.
- Bruise jaisi colour changes dikhata hai
- Lagbhag 15 din (fortnight) mein disappear ho jaata hai
- Yeh prove karta hai ki mechanical birth trauma hua aur bachcha delivery ke baad kuch time tak zinda raha
Management
- Conservative (watchful waiting) - zyada tar apne aap theek ho jaata hai
- Aspirate mat karo - infection ka risk hota hai
- Bilirubin monitor karo - jaundice treat karo agar zaroori ho
- Anaemia monitor karo
- Agar skull fracture ya intracranial pathology ka suspicion ho to neuroimaging karo
- Parents ko reassure karo - instrumental delivery ke baad counselling important hai
This is a shared conversation. Sign in to Orris to start your own chat.