49 year female known case of diabetes type 2 on metformin 1gm bd and glimiperide 2 mg bd her blood sugar fasting 118 and pp 180 came with complain of bilateral burning sensation of foot on and off increase since 2 weeks for that for that she was given methylcobalaine 1500 McG but the symptoms still persis on examination patient power 5/5 sensation intact planter down going how to manage this case
diabetic peripheral neuropathy treatment
Management of Painful Diabetic Peripheral Neuropathy (PDPN) - Case Analysis
Clinical Assessment First
- Power 5/5 - No motor involvement (typical of sensory-predominant DSPN)
- Sensation intact - Still in early-moderate neuropathy (loss of sensation is a later finding)
- Plantars downgoing - No upper motor neuron involvement (rules out myelopathy)
- Burning bilateral feet - Classic "stocking" distribution, worse recently = possibly related to glycemic variability
Step 1 - Optimize Glycemic Control
- Metformin 1g BD - appropriate
- Glimepiride 2mg BD - note: twice-daily glimepiride is unusual (glimepiride is typically once daily due to its long half-life); confirm this is correct
- SGLT2 inhibitor (empagliflozin/dapagliflozin) - added cardiometabolic benefit, weight neutral, and helps glycemic control
- GLP-1 receptor agonist (semaglutide/liraglutide) - excellent postprandial glucose lowering, weight reduction (beneficial in T2DM neuropathy)
- Consider HbA1c testing to quantify overall control - target <7% ideally <6.5% in this age group
Step 2 - Pharmacological Treatment of Neuropathic Pain
| Drug | Dose | Notes |
|---|---|---|
| Duloxetine (SNRI) | 30 mg OD x 1 week, then 60 mg OD | FDA-approved for PDPN; also helps mood/sleep which commonly co-exist |
| Pregabalin | 75 mg BD, titrate to 150-300 mg/day | Strong evidence; helps sleep; adjust for renal function |
| Gabapentin | 300 mg OD at night initially, titrate up to 900-3600 mg/day | More side effects, less preferred but effective |
- Amitriptyline 10-25 mg at bedtime - very cost-effective, effective for burning neuropathic pain; watch for anticholinergic effects and cardiac risk
- Venlafaxine 37.5-225 mg/day
- Sodium valproate 200-1200 mg/day (if other agents fail)
- Capsaicin cream (0.075%) applied to feet TID-QID - effective for burning; warn patient of initial worsening burning (TRPV1 desensitization)
- Lidocaine 5% patches - for localized pain (limited use on feet)
Step 3 - Continue and Optimize B12 Supplementation
- Check serum B12 level if not already done
- If serum B12 is low-normal or deficient: switch to IM methylcobalamin 1000 mcg daily x 7 days, then weekly x 4 weeks, then monthly
- If serum B12 is normal, continue oral supplementation but reconsider contribution to symptoms
Step 4 - Alpha Lipoic Acid (ALA)
- Alpha lipoic acid 600 mg OD or BD - can be added as adjunct; available OTC; particularly useful if patient prefers to avoid/minimize prescription medications
Step 5 - Non-Pharmacological Measures
- Foot care education - daily inspection of feet (especially important as sensation may worsen over time); use of protective footwear; avoid walking barefoot
- Exercise - regular moderate aerobic exercise improves nerve function and glycemic control
- Avoid neurotoxins - alcohol, smoking (both worsen neuropathy)
- Treat comorbidities - hypertension control is also important (BP target <130/80 in diabetics)
- Sleep hygiene - neuropathic pain is typically worse at night; addressing sleep often improves pain perception
Step 6 - Investigations to Order
| Test | Reason |
|---|---|
| HbA1c | Assess overall glycemic control over 3 months |
| Serum B12 | Confirm/rule out B12 deficiency (metformin effect) |
| Fasting lipids | Dyslipidemia worsens microvascular disease |
| Urine ACR/Creatinine | Check for diabetic nephropathy (affects drug dosing - pregabalin) |
| Renal function (eGFR) | Dose adjustment for pregabalin if needed |
| Thyroid function (TSH) | Hypothyroidism is a common reversible cause of neuropathy |
| NCS/EMG | If diagnosis unclear or atypical features (not mandatory here given classic picture) |
Summary Algorithm for This Patient
1. Optimize glycemia (HbA1c target <7%) → consider adding SGLT2i or GLP-1 agonist
2. Start Duloxetine 30mg OD → 60mg OD after 1 week
3. Check serum B12 → adjust methylcobalamin route if low
4. Add Alpha Lipoic Acid 600mg OD-BD
5. Foot care education + footwear + daily foot inspection
6. Investigate: HbA1c, B12, eGFR, lipids, TSH, urine ACR
7. Review in 4-6 weeks → if incomplete response, add Pregabalin 75mg BD
8. Refer pain management if refractory
Create a side-by-side comparison chart of PDN treatment options (duloxetine vs pregabalin vs gabapentin)
A clean, professional medical comparison chart titled "Painful Diabetic Neuropathy (PDN) - Treatment Comparison" comparing three drugs side by side: Duloxetine, Pregabalin, and Gabapentin. The chart should have clearly labeled columns for each drug with a distinct color header (blue for Duloxetine, green for Pregabalin, orange for Gabapentin). Rows should compare: Drug Class, Starting Dose, Target Dose, FDA Approval for PDN, Mechanism of Action, Time to Effect, Main Side Effects, Advantages, Disadvantages, Renal Dose Adjustment, Cost/Availability, and Best For. All text should be clear, readable, and well-organized in a table format with alternating row shading for readability. Medical infographic style, white background.
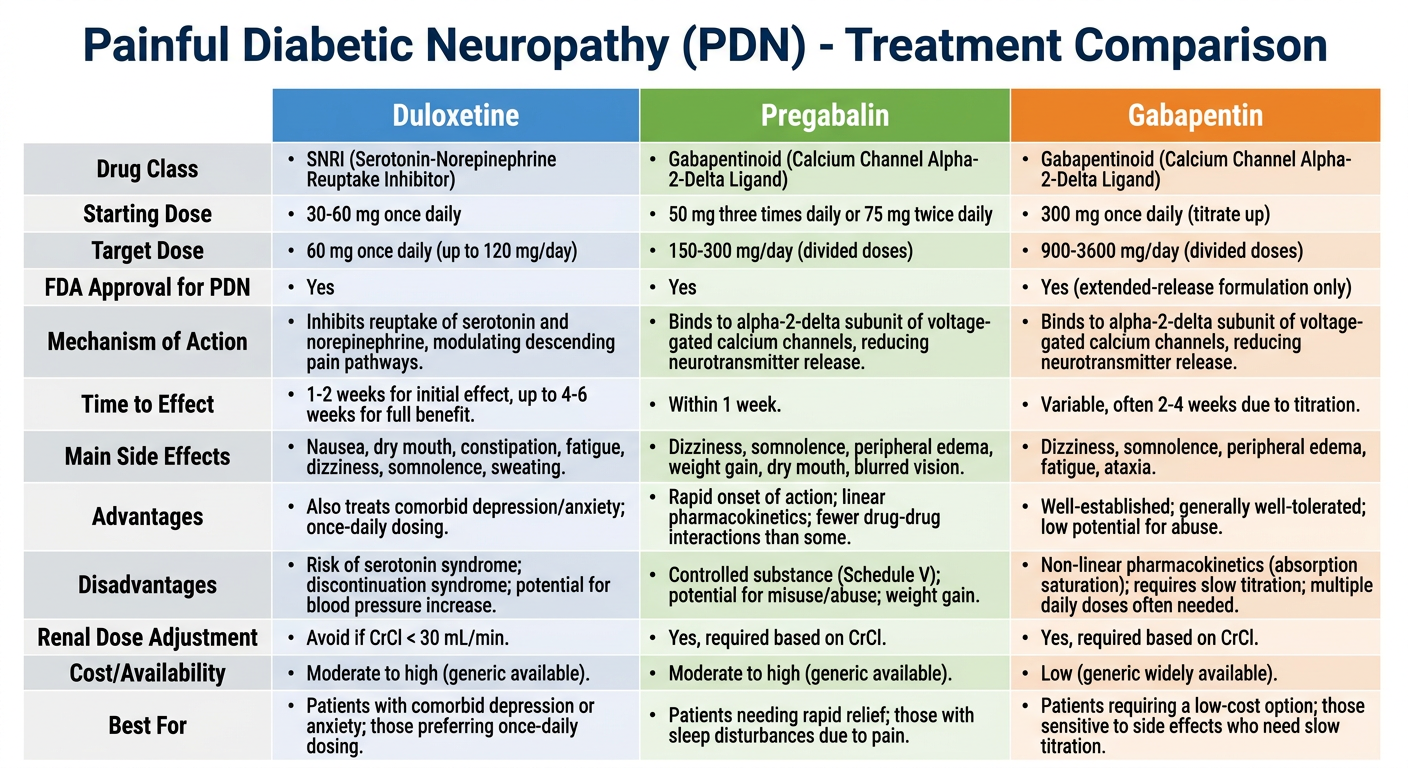
PDN Treatment: Duloxetine vs Pregabalin vs Gabapentin
| Parameter | Duloxetine | Pregabalin | Gabapentin |
|---|---|---|---|
| Drug Class | SNRI | Alpha-2-delta ligand (gabapentinoid) | Alpha-2-delta ligand (gabapentinoid) |
| Mechanism | Inhibits serotonin + norepinephrine reuptake in descending pain pathways | Binds voltage-gated Ca²⁺ channels, reduces excitatory neurotransmitter release | Same as pregabalin (less predictable binding) |
| Starting Dose | 30 mg OD x 1 week | 75 mg BD | 300 mg OD at night |
| Target Dose | 60 mg OD (max 120 mg/day) | 150-300 mg/day in divided doses | 900-3600 mg/day in 3 divided doses |
| FDA Approved for PDN | ✅ Yes (2004) | ✅ Yes (2004) | ❌ No (off-label) |
| Time to Effect | 2-4 weeks | 1-2 weeks | 2-4 weeks |
| NNT (pain relief) | ~5 | ~4-5 | ~6-7 |
| Key Side Effects | Nausea, dry mouth, insomnia, increased BP, sexual dysfunction | Dizziness, somnolence, weight gain, peripheral edema | Dizziness, somnolence, ataxia, weight gain |
| Advantages | Also treats depression/anxiety (common comorbidities); no renal dose adjustment at standard doses; once daily dosing | Predictable absorption; helps sleep; quick onset; proven in RCTs | Widely available; very low cost; can titrate flexibly |
| Disadvantages | Avoid in uncontrolled hypertension; caution in hepatic disease; withdrawal syndrome if stopped abruptly | Requires renal dose adjustment; weight gain problematic in T2DM; Schedule V (abuse potential in some countries) | Highly variable bioavailability; TID dosing required; slower titration |
| Renal Adjustment | Not required (hepatically metabolized) | ✅ Required - reduce dose if eGFR <60 | ✅ Required - reduce dose if eGFR <60 |
| Hepatic Caution | ⚠️ Avoid if significant hepatic impairment | Minimal hepatic metabolism | Minimal hepatic metabolism |
| Weight Effect | Neutral to slight loss | Weight gain ++ | Weight gain + |
| Best For | First choice when depression/anxiety co-exists; patients on once-daily regimens; normal renal function | When rapid pain relief needed; sleep disturbance prominent; if SNRI not tolerated | When cost is a major concern; combination therapy add-on |
| Avoid When | MAOIs within 14 days; uncontrolled HTN; glaucoma | Renal failure (needs dose cut); heart failure with edema | Renal failure (significant dose reduction needed) |
Burning feet syndrome
burning feet syndrome etiology management
Burning Feet Syndrome (BFS)
Definition
Pathophysiology
- First affected by metabolic insults (diabetes, nutritional deficiency)
- First affected by toxic exposures
- Sensitive to ischemia and inflammatory processes
Causes - Differential Diagnosis
1. Metabolic / Endocrine
| Cause | Mechanism | Clues |
|---|---|---|
| Diabetes mellitus (most common) | Chronic hyperglycemia → oxidative stress → small fiber axonopathy | Known DM, poor glycemic control, stocking distribution |
| Hypothyroidism | Myxedematous infiltration of nerves | Weight gain, cold intolerance, constipation, delayed reflexes |
| Chronic kidney disease | Uremic toxin accumulation | Elevated creatinine, uremia features |
| Liver disease | Toxic metabolite accumulation | Jaundice, ascites |
2. Nutritional Deficiencies
| Deficiency | Notes |
|---|---|
| Vitamin B12 | Most common nutritional cause; especially with metformin use, veganism, pernicious anemia |
| Vitamin B1 (Thiamine) | Alcoholics, malabsorption; "wet beriberi" includes burning feet |
| Vitamin B5 (Pantothenic acid) | Rare; classic "burning feet" - small fiber neuropathy with dysesthesias (Goldman-Cecil Medicine) |
| Vitamin B3 (Niacin/B3 deficiency) | Presumed small-fiber neuropathy causing "burning feet"; treat with B-complex vitamins |
| Folate deficiency | Co-exists with B12 deficiency |
| Vitamin B6 toxicity (paradox) | Excess pyridoxine (>200 mg/day) can itself cause sensory neuropathy |
3. Small Fiber Neuropathy (Idiopathic / Cryptogenic)
- Affects predominantly elderly women
- Burning hands and feet without autonomic features
- Normal NCS (large fibers spared) - diagnosis requires skin punch biopsy showing reduced intraepidermal nerve fiber density (IENFD)
- Accounts for a significant proportion of "idiopathic" cases
- Associated with: Sjögren's syndrome, SLE, sarcoidosis, celiac disease
4. Toxic / Drug-Induced
| Agent | Notes |
|---|---|
| Alcohol | Direct neurotoxin + nutritional deficiency |
| Chemotherapy (cisplatin, vincristine, paclitaxel) | Toxic neuropathy |
| Isoniazid | B6-depleting neuropathy |
| Metronidazole, nitrofurantoin | Sensory neuropathy |
| Statins | Rare association |
| Heavy metals (arsenic, thallium) | Occupational exposure |
5. Structural / Entrapment
| Cause | Notes |
|---|---|
| Tarsal tunnel syndrome | Tibial nerve compression behind medial malleolus → burning sole of foot; positive Tinel's sign at tarsal tunnel |
| Morton's neuroma | Burning between 3rd-4th toes; worse with narrow footwear |
| Plantar fasciitis | More pain than burning; worse first step in morning |
6. Vascular
| Cause | Notes |
|---|---|
| Erythromelalgia | Episodic burning + redness + warmth of feet; relieved by cooling; associated with polycythemia vera, essential thrombocythemia |
| Peripheral arterial disease | Burning with claudication; absent pulses |
| Raynaud's phenomenon | Usually hands; can involve feet |
7. Systemic Inflammatory / Autoimmune
- Sjögren's syndrome (small fiber ganglionopathy/neuropathy)
- Systemic lupus erythematosus
- Rheumatoid arthritis
- Sarcoidosis
- Vasculitis
8. Infectious
- HIV-associated distal sensory polyneuropathy
- Leprosy (pure neuritic - especially in endemic areas)
- Lyme disease
9. Hereditary
- Fabry disease (X-linked lysosomal storage disorder) - acral burning pain in young males
- Hereditary sensory and autonomic neuropathies (HSAN)
- Charcot-Marie-Tooth (some subtypes)
Clinical Features
- Burning, heat sensation predominantly in soles, extending to dorsum and lower leg
- Worse at night (classic)
- Relieved by cold surfaces / cold water (patients often sleep with feet outside blankets)
- May be accompanied by tingling, pins-and-needles, hyperesthesia (light touch feels painful)
- Normal motor exam in early/pure small fiber neuropathy (power and reflexes intact)
- Standard NCS may be normal (small fibers not tested by routine NCS)
Investigations
| Investigation | Purpose |
|---|---|
| FBS, HbA1c, OGTT | Diabetes / prediabetes |
| TSH, T3, T4 | Hypothyroidism |
| Serum B12, folate | Nutritional deficiency |
| Renal function (creatinine, eGFR) | CKD/uremic neuropathy |
| LFTs | Hepatic neuropathy |
| CBC | Anemia, polycythemia (erythromelalgia) |
| ANA, anti-SSA/SSB | Sjögren's, SLE |
| Serum protein electrophoresis (SPEP) | Paraproteinemic neuropathy |
| HIV serology | If risk factors |
| Leprosy slit-skin smear | Endemic areas |
| NCS/EMG | Large fiber assessment; normal in pure SFN |
| Skin punch biopsy (IENFD) | Gold standard for small fiber neuropathy diagnosis |
| Quantitative sensory testing (QST) | Warm/cold detection thresholds; detects SFN |
Management
Treat the Underlying Cause (Priority)
- Optimize glycemic control (diabetes)
- Thyroid hormone replacement (hypothyroidism)
- B12 injections (deficiency) - especially if on metformin
- B-complex vitamins (nutritional deficiency)
- Alcohol cessation
- Surgical decompression (tarsal tunnel syndrome)
- Aspirin + venesection (erythromelalgia/polycythemia)
Symptomatic Neuropathic Pain Relief
- Duloxetine 30-60 mg OD (first-line)
- Pregabalin 75-300 mg/day (first-line)
- Gabapentin 300-3600 mg/day (alternative)
- Amitriptyline 10-25 mg at night (cost-effective)
- Alpha lipoic acid 600 mg OD-BD (antioxidant; evidence in diabetic SFN)
- Capsaicin cream 0.075% applied to soles TID-QID (desensitizes TRPV1 channels)
- Lidocaine 5% patch (localized use)
Non-Pharmacological
- Sleep with feet uncovered or use cool water soaks before bed
- Avoid tight footwear; wear breathable socks
- Regular moderate exercise
- Avoid alcohol, smoking, neurotoxic drugs where possible
- TENS (transcutaneous electrical nerve stimulation) - moderate evidence
Key Distinguishing Point
In a patient presenting with burning feet, always ask:
- Both feet simultaneously? → Systemic (metabolic, toxic, nutritional)
- One foot or asymmetric? → Structural (tarsal tunnel, lumbar radiculopathy, mononeuropathy)
- Episodic with redness and warmth? → Erythromelalgia
- Better with cold? → Small fiber neuropathy, erythromelalgia
- Normal NCS? → Do skin biopsy to assess small fiber density