🦾 NAIL ANATOMY & DISORDERS — Dermatology Resident Study Note
Sources: Rook's Dermatology (Chapter 93, Pasch, Richert & Iorizzo); Dermatology 5e / Bolivnia (Tosti & Piraccini, Ch. 71); Fitzpatrick's Dermatology (Haneke, Ch. 91); Andrews' Diseases of the Skin (Ch. 33); Goldman-Cecil Medicine; Goodman & Gilman's; Recent JAAD/PubMed reviews (2024-2025)
PART 1 — ANATOMY OF THE NAIL UNIT
1.1 Gross Anatomy
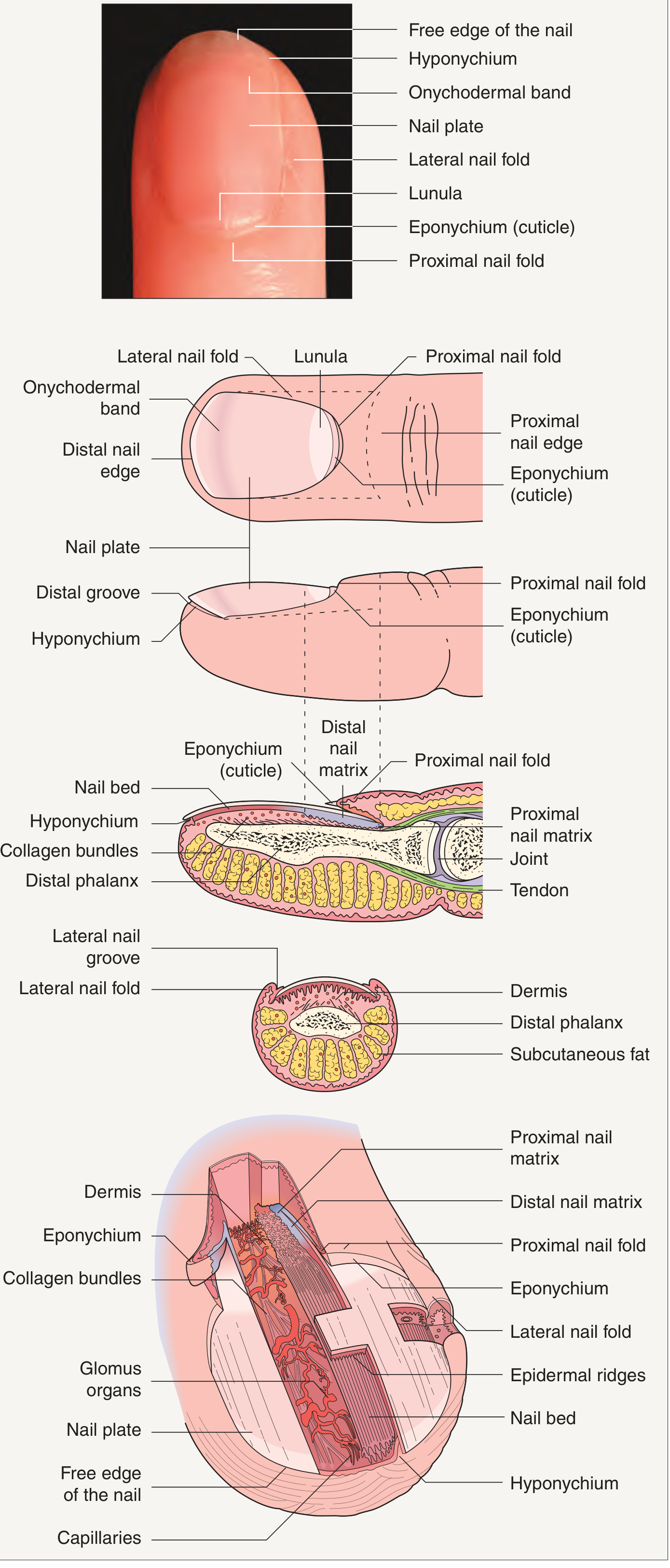
Fig. 68.7 - Complete Nail Unit Anatomy (Dermatology 5e / Bolivnia)
Full nail apparatus: dorsal view (top), sagittal sections showing matrix, nail bed, phalanx, glomus organs, capillaries, and collagen bundles.
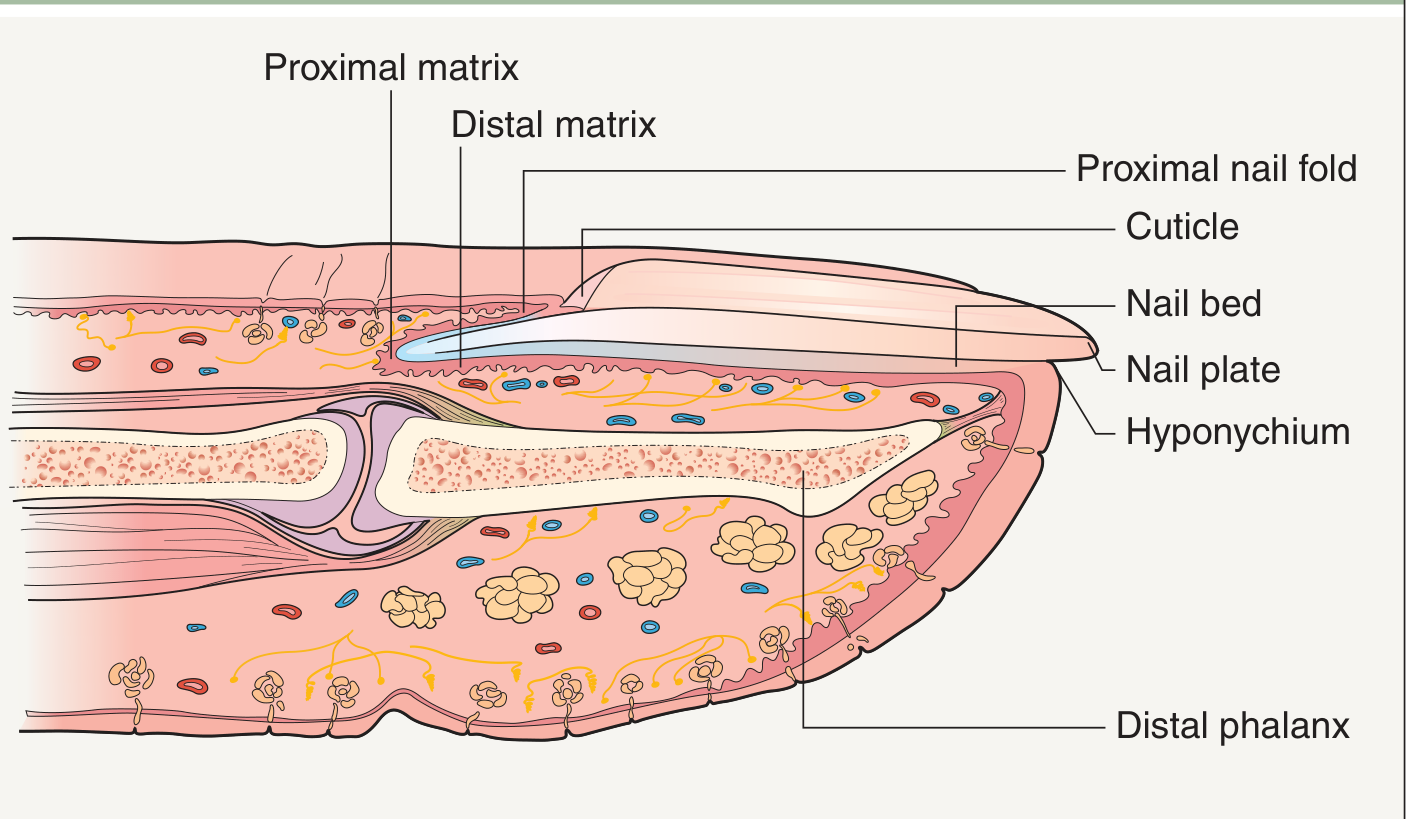
Fig. 71.1 - Nail Apparatus Cross-Section (Fitzpatrick/Bolivnia)
The nail apparatus consists of:
| Component | Description | Function |
|---|
| Nail plate | Hard, semitransparent, slightly convex sheet of tightly packed onychocytes ("hard" hair-type keratins) | Protection, fine touch, grooming |
| Nail matrix (germinal) | Proximal zone under the proximal nail fold; produces the nail plate | Primary nail plate production |
| - Proximal matrix | Ventral aspect of proximal nail fold | Produces dorsal nail plate (upper 80%) |
| - Distal matrix | The visible lunula | Produces ventral nail plate (lower 20%) |
| Lunula | White half-moon; distal margin of the germinal matrix visible through transparent plate | Junction matrix/bed |
| Nail bed (sterile matrix) | Epidermis 2-3 cells thick, no granular layer, tightly apposed to periosteum | Plate adherence; possibly contributes ~21% of nail thickness |
| Proximal nail fold (PNF) | Double-layered fold overlying proximal nail plate | Protects matrix from trauma/infection |
| - Dorsal layer | Continuation of digit skin | - |
| - Ventral layer | Continuous with nail matrix | - |
| Cuticle (eponychium) | Thin strip of cornified epithelium adhering to nail plate edge | Seal against ingress |
| Lateral nail folds | Compress nail from sides; guide longitudinal growth | Transverse curvature of plate |
| Hyponychium | Junction nail bed/digit tip; where plate detaches | Distal seal; barrier |
| Onychodermal band | Most distal attachment of cornified epithelium to nail undersurface (nail isthmus) | Critical for nail-bed adhesion; when breached → progressive onycholysis |
Sources: Rook's Ch.93, pp 93.2-93.3; Bolivnia Dermatology 5e pp 1382-1383; Fitzpatrick Ch.91; Andrews' Ch.33
1.2 Microscopic Anatomy
Nail plate structure:
- Trilaminar: dorsal plate (from ventral PNF), intermediate/main plate (germinal matrix), ventral plate (nail bed contribution)
- Contains hard "hair-type" keratins embedded in sulfur-rich, high-cysteine and high-glycine/tyrosine proteins
- No granular layer in health; granular layer appears in psoriasis, onychomycosis = pathological sign
Nail bed:
- Epidermis 2-3 cells thick; transition from living keratinocyte to dead ventral nail plate is abrupt (1 horizontal cell layer) — resembles Henle layer of inner root sheath
- Dermis sparse, no subcutaneous fat; collagen bundles closely attached to periosteum
- Clinical implication: bacterial infections spread rapidly to bone → osteomyelitis risk
Nail matrix:
- Keratinization occurs along an oblique axis (upward and distal)
- MIB-1 (Ki-67) staining labels proliferating matrix cells
- Contains dormant melanocytes (mainly distal matrix has an active compartment); nail bed has almost no melanocytes
Sources: Rook's Ch.93 pp 93.3-93.4; Bolivnia 5e p.1383; Fitzpatrick Ch.91
1.3 Keratins
| Keratin Pair | Location |
|---|
| K5/K14 | Basal layer of nail matrix AND nail bed |
| K1/K10 | Suprabasal nail matrix (absent in healthy nail bed; appears in disease with granular layer - psoriasis, onychomycosis) |
| K6/K16 | Various subungual locations during matrix development |
Source: Rook's Ch.93 p.93.4
1.4 Blood Supply
- Paired digital arteries (large palmar, small dorsal digital artery on each side)
- Palmar arteries supplied from superficial and deep palmar arcades
- Distally: extremely tortuous and coiled vessels (can distort without kinking)
- Superficial arcade: just distal to DIP joint → supplies nail fold, extensor tendon, germinal matrix
- Glomus bodies (Masson): specialized neuromyoarterial structures; regulate capillary circulation; abundant in nail bed with gradient toward distal nail bed; dilate with cold (opposite of arterioles) to maintain acral circulation
Source: Rook's Ch.93 pp 93.5
1.5 Nerve Supply
- Paired digital nerves follow arterial blood supply
- Periunugual soft tissues innervated by dorsal branches
- Main digital nerve passes under the nail bed and innervates both nail bed and matrix
- Dual sensory innervation is common → ring block anaesthesia must address both dorsal and palmar branches
Source: Rook's Ch.93 p.93.5
1.6 Nail Growth and Morphology
| Nail | Growth Rate |
|---|
| Fingernails | ~3 mm/month |
| Toenails | ~1 mm/month |
TABLE 93.1 — Factors Affecting Nail Growth Rate
| Factor | Faster | Slower |
|---|
| Time of day | Daytime | Night |
| Hand dominance | Right hand / dominant | Left hand |
| Age | Youth | Old age |
| Digits | Fingers; middle fingers | Toes; thumb/little finger |
| Season | Summer | Winter/cold |
| Sex | Male | Female |
| Behaviour | Nail biting/friction | — |
| Disease (faster) | Psoriasis, pityriasis rubra pilaris, hyperthyroidism, HIV, AV shunts | — |
| Disease (slower) | — | Beau lines, onycholysis, yellow nail syndrome, hypothyroidism, immobilization, denervation, poor nutrition, congestive heart failure, onychomycosis |
| Drugs (faster) | Levodopa, itraconazole, etretinate (rarely) | — |
| Drugs (slower) | — | Methotrexate, azathioprine, targeted therapies/immunotherapies, etretinate |
Source: Rook's Ch.93 Table 93.1 & 93.2
1.7 Immunology of the Nail
- Nail matrix exhibits immune privilege (similar to hair matrix, eye, testis)
- Contains human cathelicidin LL-37 (kills Candida albicans) and beta-defensins hβD-2 and hβD-3
- MHC class I molecules are restricted in the nail matrix, protecting it from autoimmune T-cell attack
Source: Rook's Ch.93 p.93.4-93.5
1.8 Signalling Pathways in Nail Formation
- Wnt/β-catenin signalling is crucial in nail embryogenesis and adult maintenance
- R-spondin 4 mutations → autosomal recessive anonychia
- Frizzled-6 (Wnt receptor) mutations → inherited nail dysplasia
- BMPs (bone morphogenetic proteins) work with Wnt signalling
- Spondins = family of proteins for intracellular communication
Source: Rook's Ch.93 p.93.3-93.4
PART 2 — NAIL SIGNS AND THEIR SIGNIFICANCE
Fig. 71.2 (Bolivnia/Dermatology 5e) — Overview of Nail Signs:
(Beau's lines, onycholysis, onychorrhexis, onychomadesis, onychoschizia, pitting in psoriasis/alopecia areata, lichen planus, Darier disease, koilonychia, leukonychia, clubbing, splinter haemorrhages, pincer nail, brachyonychia, onychogryphosis, pterygium, melanonychia, onychomatricoma, onychopapilloma)
2.1 Abnormalities of Shape
Clubbing (Hippocratic fingers, acropachy, watch-glass nails)
Geometric assessment:
| Measurement | Normal | Clubbing |
|---|
| Lovibond's angle (nail plate - PNF junction) | < 160° | > 180° |
| Curth's angle (DIP joint) | ~180° | < 160° |
| Schamroth's window | Open diamond window | Obliterated |
Pathophysiology: Increased blood flow through vasodilated nail unit vasculature; elevated circulating VEGF → nail bed angiogenesis; HPGD and SLCO2A1 mutations → pachydermoperiostosis
Causes of secondary clubbing (Table 93.3):
- Respiratory: thoracic carcinoma, mesothelioma, asbestosis, cryptogenic fibrosing alveolitis, sarcoidosis, cystic fibrosis, pulmonary AVM, tuberculosis
- Cardiac: cyanotic heart disease (PDA, septal defect), infective endocarditis, hepatopulmonary syndrome
- GI: inflammatory bowel disease, carcinoma of oesophagus, liver disease, laxative abuse, chronic parasitic infestation
- Endocrine: thyroid disease (thyroid acropachy)
- Other: HIV (37%), POEMS syndrome (70%), hemiplegia, subungual tumour, lupus erythematosus
Sources: Rook's Ch.93 pp 93.7-93.8; Andrews' Ch.33; Bolivnia 5e
Koilonychia (Spoon nail)
- Concave, spoon-shaped nail plate
- Most common systemic associations: iron deficiency and haemochromatosis
- Also: deficiency of cysteine-rich keratin (trichothiodystrophy), familial (AD) in adults
- Secondary: psoriasis, lichen planus, dermatophyte infection (nail bed hyperkeratosis pushes nail up distally)
- Occupational: mechanics (oil softens nail), hairdressers (permanent wave solutions)
Source: Rook's Ch.93 p.93.9
Pincer nail (Trumpet nail, Arched nail)
- Transverse overcurvature increasing toward the distal tip, pinching soft periungual tissues
- Three patterns:
- Associated with psoriasis (thumbs and big toes)
- Inherited form (gradient from thumbs/big toes outward, progresses with time)
- Isolated (independent nail fold)
- Treatment: orthopaedic braces, nail plate ablation/partial matricectomy, Z-plasty, dermal flap
Source: Rook's Ch.93 p.93.9
Pachyonychia
- Thickened nail plate with yellowish colour, increased transverse overcurvature, horseshoe-shaped free edge, extreme hardness
- Congenital: Jadassohn-Lewandowsky syndrome (pachyonychia congenita)
- Acquired: psoriasis, pityriasis rubra pilaris, chronic eczema, onychomycosis
Brachyonychia (Racquet nails)
- Width of nail plate > length; usually thumb, AD with higher prevalence in females
- Premature ossification of epiphysis of distal phalanx (age 7-10 years)
- Also in patients under chronic haemodialysis (tertiary hyperparathyroidism with phalangeal tuft resorption)
Anonychia / Micronychia
- Anonychia: absence of nail plate; mutations in R-spondin 4, Frizzled-6 or Wnt10a genes
- Nail-Patella Syndrome (hereditary osteo-onychodysplasia, Fong syndrome): triangular lunulae are pathognomonic; LMX1B gene mutation; associated with absent/hypoplastic patella, posterior iliac horns, glomerulonephritis (20% develop renal failure), "Lester iris"
Source: Andrews' Ch.33 p.914
2.2 Abnormalities of Nail Attachment
Onycholysis
- Separation of nail plate from nail bed starting distally at onychodermal band, moving proximally
- Detached nail plate looks white (apparent leukonychia) due to air underneath
- Green discoloration = Pseudomonas aeruginosa
- Causes: trauma, psoriasis (30% of psoriatics), fungal infection, contact dermatitis, photo-onycholysis (psoralens, doxycycline, demethylchlortetracycline), retinoids, drugs (5-FU, captopril), hypothyroidism, hyperthyroidism, yellow nail syndrome
Dermoscopic types:
- Post-traumatic: regular margin, usually lateral
- Psoriatic: irregular margin, involves whole free edge, erythematous border
- Onychomycosis: ragged/spike edge, mycelium visible proximally
Source: Rook's Ch.93 pp 93.10-93.11
Pterygium
- Dorsal (true) pterygium: fibrotic band from proximal nail fold divides nail in two; causes: lichen planus (most common), trauma, graft-versus-host disease, leprosy
- Ventral pterygium (pterygium inversum unguis): forward extension of nail bed epithelium, obscuring distal groove; causes: trauma, systemic sclerosis, Raynaud, lupus, familial
Source: Rook's Ch.93 p.93.12
2.3 Nail Surface Changes
Beau Lines (Transverse grooves)
- Transverse depressions = temporary interruption of proximal nail matrix mitotic activity
- Depth = extent of matrix damage; Width = duration of insult
- Migrate distally with nail growth
- Causes: manicure trauma, eczema, chronic paronychia (local); severe febrile illness, cytotoxic drugs, erythroderma (systemic — appears on all nails simultaneously)
- Beau lines → onychomadesis when full thickness groove
Source: Rook's Ch.93 p.93.13; Bolivnia 5e p.1443
Pitting
- Shallow depressions from foci of parakeratosis in proximal matrix
- Fine pits (<1mm): psoriasis (most common; >10 pits/nail or >60 total supports diagnosis)
- Coarse pits: eczema
- Geometric/geometric arranged: alopecia areata ("Elkonyxis" = single large pit = reactive arthritis, psoriasis)
- "Elkonyx": deep full-thickness single pit in nail plate
Trachyonychia (Twenty-nail dystrophy)
- Rough, sandpaper-like, opaque surface of all 20 nails; also "shiny" variant
- Associated with: alopecia areata (most common), psoriasis, lichen planus, eczema, vitiligo, idiopathic
- Histology: spongiosis and lymphocytic infiltrate of nail matrix
Onychoschizia (Lamellar dystrophy)
- Distal horizontal lamellar splitting of nail plate
- Causes: repeated wet-dry cycles, chemical exposure
Longitudinal Ridging / Beading
- Common with aging; not a sign of disease; more prominent in elderly
Median Canaliform Dystrophy of Heller
- Midline longitudinal split with fir-tree appearance of ridges angled backwards
- Thumbs most commonly affected; often self-resolving
- Distinct from habit-tic (washboard nails): habit-tic has disturbed cuticle
2.4 Nail Colour Changes
| Colour | Cause |
|---|
| White (true leukonychia) | Parakeratosis in nail plate (Mees' lines = arsenic/systemic insult) |
| White (apparent leukonychia) | Changes in nail bed shine through plate; disappear with pressure (Muehrcke's lines = hypoalbuminemia; Terry's nails = liver disease; half-and-half nails = renal disease) |
| Yellow | Yellow nail syndrome, psoriasis (subungual hyperkeratosis), fungal |
| Green | Pseudomonas aeruginosa (chloronychia) |
| Brown/black | Melanonychia (matrix melanocytes), subungual haematoma |
| Red/erythema of lunula | Psoriasis, cardiac failure, CO poisoning, alopecia areata |
| Splinter haemorrhages | Longitudinal capillary haemorrhages; psoriasis, endocarditis, trauma |
Melanonychia — ABCDEF rule for nail melanoma (Haneke/Fitzpatrick):
| Letter | Stands for |
|---|
| A | Age (40-70), African/Asian/Native American ancestry |
| B | Brown/Black band, >3mm, Blurred borders |
| C | Change in morphology |
| D | Digit (thumb > hallux > index; single digit) |
| E | Extension of pigment to nail fold (Hutchinson's sign) |
| F | Family/personal history of melanoma |
Source: Fitzpatrick's Ch.91; Rook's Ch.93 p.93.15
2.5 Nail Signs in Systemic Disease
| Sign | Disease |
|---|
| Clubbing | Cardiopulmonary, GI, liver, HIV, POEMS |
| Koilonychia | Iron deficiency anaemia, haemochromatosis |
| Splinter haemorrhages | Endocarditis, vasculitis, psoriasis, trauma |
| Muehrcke's lines (apparent leukonychia) | Hypoalbuminemia (liver disease, nephrotic syndrome) |
| Terry's nails | Hepatic cirrhosis (white proximally, normal distally) |
| Half-and-half nails (Lindsay's nails) | Chronic renal failure |
| Yellow nail syndrome | Lymphoedema, pleural effusion, primary lymphedema, bronchiectasis |
| Onycholysis | Hypothyroidism, hyperthyroidism |
| Periungual telangiectasia | Dermatomyositis (most specific), SLE, systemic sclerosis |
| Ragged cuticles | Dermatomyositis |
| Triangular lunula | Nail-patella syndrome |
| Red lunula | Psoriasis, CO poisoning, cardiac failure |
| Beau lines (all nails) | Systemic illness, cytotoxics, erythroderma |
| Periungual fibromas (Koenen tumours) | Tuberous sclerosis (develop around puberty) |
Sources: Rook's Ch.93; Bolivnia 5e; Fitzpatrick's Ch.91; Andrews' Ch.33
PART 3 — NAIL DISORDERS
3.1 Nail Psoriasis
Epidemiology: >50% prevalence in plaque psoriasis; lifetime incidence 80-90%; 5-10% nail psoriasis without skin/joint disease; major risk factor for psoriatic arthritis (annual risk 0.55-2.55% vs 0.26-1.14% without nail involvement)
Genetics: HLA-Cw6 negative (contrast with skin psoriasis which is HLA-Cw6 positive); Asian patients: HLA-B46, HLA-A*02:07 association
Pathophysiology: Enthesitis of extensor tendon at DIP → nail unit inflammation; same mediators as skin psoriasis (TNF-α, IL-6, IL-8, NF-κB, mast cells, LL-37, hβD-2, hβD-3)
Clinical Features by Anatomical Site (Table 93.4 — Zaias Classification):
| Clinical Feature | Site of Disease | Duration |
|---|
| MATRIX SIGNS | | |
| Pitting | Proximal matrix | Episodic (short) |
| Transverse furrows | Proximal matrix + distal extension | 1-2 weeks |
| Crumbling nail plate | Entire matrix | Prolonged |
| Leukonychia with rough surface | Proximal (± distal) matrix | Variable |
| NAIL BED SIGNS | | |
| Splinter haemorrhages | Nail bed dermal ridge haemorrhage | Short |
| Oil spot / onycholysis (salmon patch) | Nail bed psoriasis | Prolonged |
| False nail post-onychomadesis | Nail bed psoriasis | Prolonged |
| Subungual hyperkeratosis | Nail bed psoriasis | Prolonged |
| Yellow/green discoloration | Secondary yeast/Pseudomonas infection | Prolonged |
Special features:
- Salmon (oil drop) patch: characteristic yellowish-red translucent zone at leading edge of onycholysis — pathognomonic
- Acrodermatitis continua of Hallopeau (ACH): sterile pustular form; severe destruction
- POPP (Psoriatic onychopachydermoperiostitis): nail thickening, periosteal reaction, bone erosion without joint involvement
- Onychomycosis co-infection: more common in psoriatics; must treat with antifungals alongside nail psoriasis treatment (Koebner effect)
Investigation: Clinical diagnosis; nail unit biopsy (gold standard); onychoscopy: dilated tortuous capillaries in nail bed/hyponychium (90%), coarse pits, salmon patches, splinter haemorrhages
Treatment Algorithm (Figure 93.69):
≤3 nails (matrix) → Intralesional steroid injections FIRST LINE
→ Topical vitamin D ± topical steroids SECOND LINE
≤3 nails (nail bed) → Topical steroids or vitamin D FIRST LINE
>3 nails → Intralesional steroids ± topical vitamin D + steroids FIRST LINE
→ Systemic: methotrexate (≤15mg/week), ciclosporin (3-5mg/kg short-term),
acitretin (0.2-0.4mg/kg, 6 months)
→ Biologics: adalimumab (only FDA-approved for nail psoriasis), infliximab,
etanercept, certolizumab pegol, golimumab, ustekinumab, secukinumab,
ixekizumab, risankizumab, brodalumab, guselkumab
→ Small molecules: apremilast, tofacitinib
Sources: Rook's Ch.93 pp 93.44-93.50; Hwang JK et al. JAAD 2024 Mar [PMID 38007038]
3.2 Lichen Planus of the Nails (NLP)
Epidemiology: 5-10% of LP patients; most common 5th-6th decade
Clinical features (Andrews' Ch.33; Rook's Ch.93):
- Irregular longitudinal grooving and ridging (onychorrhexis)
- Thinning of nail plate
- Dorsal pterygium (fusion of PNF with matrix/nail bed) — most characteristic
- Nail shedding with atrophy
- Subungual keratosis
- Erythronychia (red streaks/longitudinal erythronychia)
- Subungual hyperpigmentation
- Nail degloving
- Trachyonychia (20-nail dystrophy, shiny variant)
- Idiopathic atrophy of nails = most severe variant (acute onset, rapid irreversible nail destruction)
Histology: Most frequently involves matrix; interface dermatitis with band-like lymphocytic infiltrate, basal cell liquefaction (identical to cutaneous LP)
Treatment:
- Intralesional triamcinolone acetonide (matrix/nail bed; digital nerve block first)
- Oral prednisone (0.5-1 mg/kg for 3 weeks) or IM triamcinolone (0.5-1mg/kg/month x 3-6 months in children)
- Combination: oral retinoids + topical corticosteroids
- Tazarotene + topical steroids under occlusion
Andrews' note: "Oral prednisone (0.5-1 mg/kg for 3 weeks) or oral retinoids in combination with topical corticosteroids... Children with typical NLP respond to 0.5-1 mg/kg/month IM triamcinolone for 3-6 months"
Clinical image — Nail Lichen Planus:
Fig. 33.38 - Pterygium caused by lichen planus (Andrews' Diseases of the Skin Ch.33)
Fig. 33.39 - Nail lichen planus (Andrews' Diseases of the Skin Ch.33)
Sources: Andrews' Ch.33 pp 501-519; Rook's Ch.93 p.93.52-93.54; Hwang JK et al. JAAD 2024 Mar [PMID 38007038]
3.3 Onychomycosis
Causative organisms (DLSO most common):
- Dermatophytes: Trichophyton rubrum (most common, 70-80%), T. mentagrophytes
- Yeasts: Candida spp. (mainly fingernails; associated with chronic paronychia)
- Moulds: Aspergillus, Fusarium, Scytalidium (Neoscytalidium)
Classification (types):
| Type | Description | Common Organism |
|---|
| DLSO (Distal and Lateral Subungual Onychomycosis) | Most common; starts at free edge/lateral margins; subungual hyperkeratosis, onycholysis | T. rubrum |
| PSO (Proximal Subungual Onychomycosis) | Infection via nail fold; leukonychia at lunula; immunocompromised patients (HIV) | T. rubrum |
| SWO (Superficial White Onychomycosis) | Powdery white patches on dorsal nail surface | T. interdigitale, moulds |
| Endonyx | Nail plate milky white without subungual hyperkeratosis | T. soudanense, T. violaceum |
| CDLSO (Candida distal onychomycosis) | Chronic mucocutaneous candidiasis | Candida spp. |
| Total dystrophic | Advanced end stage | Any |
Diagnosis:
- KOH direct microscopy (filaments — see Table 93.5)
- Fungal culture (gold standard); PAS histology of nail clippings
- PCR (faster, more sensitive)
Treatment (Goodman & Gilman's; Goldman-Cecil; Fitzpatrick's):
- Terbinafine oral: 250mg/day × 6 weeks (fingernails), 12 weeks (toenails) — most effective
- Itraconazole oral: 200mg/day continuous OR pulse (400mg/day × 1 week/month × 2 for fingernails, 3 for toenails)
- Fluconazole: 150-450mg weekly × 3 months (fingernails), 6 months (toenails)
- Topical: ciclopirox lacquer (8%), efinaconazole, tavaborole (less effective alone; useful in mild SWO or adjunct)
- Laser therapy: limited evidence
- Nail avulsion (partial/total) as adjunct to reduce fungal mass
Differential from psoriasis (Table 93.5 — Rook's):
| Feature | Onychomycosis | Psoriasis | Chronic Paronychia | Dermatitis |
|---|
| Colour | Yellow/brown | Normal/yellow/brown | Brown/black edge | Normal |
| Onycholysis | Frequent | Frequent | Usually absent | Tip/absent |
| Pitting | Infrequent | Often, fine | Uncommon | Coarse |
| KOH | Filaments abundant | Up to 20% also have onychomycosis | Spores in lateral nail fold | Absent |
| Cross-ridging | Absent | Uncommon | Frequent | Frequent |
Sources: Rook's Ch.93 Table 93.5; Andrews' Ch.33; Zaraa I et al. Hand Surg Rehabil 2024 [PMID 38218374]; Goldman-Cecil
3.4 Paronychia
Acute Paronychia
- Inflammation, swelling, pain of proximal and lateral nail folds ± abscess
- 3× more common in females; index finger and thumb most affected
- Causes: Staphylococcus aureus (most common); also Streptococcus, herpes simplex (herpetic whitlow), orf virus, Candida, Treponema pallidum
- Neutropenic patients: Fusarium, Aspergillus
- Artificial nails/gel polish → can harbour bacteria inaccessible to routine hand hygiene
Treatment:
- Superficial abscess → drain with pointed scalpel (no anaesthesia needed)
- Deep → penicillinase-resistant antibiotic + surgery if no response in 48h
- Herpetic whitlow: oral aciclovir/famciclovir/valaciclovir for frequent recurrences; topical has no benefit
Chronic Paronychia
- Inflammatory dermatosis of nail folds; retraction of periunugal tissues, loss of cuticle
- Predominantly domestic/catering workers (wet work); females; first 3 fingers of dominant hand
- Pathophysiology: Candida is NOT the primary pathogen — it is irritant reaction/contact allergy/food hypersensitivity; Candida is a secondary coloniser
- Clinical: loss of cuticle, Beau lines, cross-ridging, ± dark discoloration lateral edges
Treatment:
- Avoid wet work (gloves); topical imidazoles (for Candida colonization)
- Topical/intralesional steroids
- Systemic antifungals are NOT useful (Candida not primary pathogen)
- Surgical: crescent-shaped excision of PNF when refractory (heals by secondary intention in <2 weeks)
Source: Rook's Ch.93 pp 93.40-93.44
3.5 Darier Disease of the Nails
- Multiple nails with multiple red and white bands = candy-cane appearance (longitudinal erythronychia + longitudinal leukonychia) = pathognomonic
- Free margin: V-shaped notch and fissure (fragility)
- Histology: acantholysis + multinucleate giant cells + epithelial hyperplasia in nail bed
Source: Rook's Ch.93 pp 93.50-93.51
3.6 Eczematous Nail Dystrophy
- Prevalence: almost all hand eczema patients; ~16% in atopic dermatitis
- Features: thickened/pitted/rough/discoloured nails; Beau lines (very common); loss of cuticle → Candida/bacterial superinfection; coarse pits (distinguish from fine pits of psoriasis)
- Phototoxic dermatitis (tetracyclines, 5-FU, capecitabine) → onycholysis matching shape of proximal nail fold
3.7 Yellow Nail Syndrome
Triad:
- Yellow, thickened, overcurved nails with absent lunula and loss of cuticle
- Lymphoedema (legs)
- Pleural effusion
- Also associated with: bronchiectasis, rhinosinusitis, chronic cough
- Growth arrest: nails grow extremely slowly (<0.1mm/week)
- Treatment: vitamin E (tocopherol) topically or systemically; triazoles; treat underlying condition
Source: Andrews' Ch.33; Rook's Ch.93
3.8 Nail Tumours
Benign
Glomus Tumour:
- 1-2% of all hand tumours; predominantly women (up to 90%); 4th-5th decade
- Triad: Love test (point tenderness over lesion), Hildreth's sign (pain relief with tourniquet), cold sensitivity test
- Presentations: small reddish/bluish spot under nail plate; OR longitudinal erythronychia with distal notching/fissure
- Investigation: MRI (gold standard — highest sensitivity, best extent assessment); high-resolution ultrasound with colour Doppler
- Treatment: surgical excision (transungual approach preferred)
- Complication: bone erosion in 50% of cases
Subungual Exostosis:
- Benign osteochondral outgrowth from distal phalanx
- 75% great toenail; porcelain white hue with surface telangiectasias + collarette in early stage
- Investigation: X-ray (cup-shaped bone outgrowth)
- Treatment: surgical excision
Digital Myxoid Pseudocyst (Synovial cyst):
- Leakage of synovial fluid through DIP joint capsule breach (>85% confirmed on MRI)
- Types: A (nodule between DIP and PNF), B (in PNF → longitudinal groove in nail), C (under matrix → reddish/bluish lunula)
- Treatment: cryotherapy (type A); drainage + compression; methylene-blue guided surgery (94% success on fingers)
Acquired Ungual Fibrokeratoma:
- Pedunculated fibroepithelial lesion; garlic-clove fibroma; from proximal nail fold; lies in longitudinal groove
- NO histological difference from Koenen tumours of tuberous sclerosis (but Koenen tumours have no hyperkeratotic tip)
- When multiple → rule out tuberous sclerosis
Onychomatricoma:
- Rare benign matrix tumour (described 1992 by Baran and Kint)
- Classic features: longitudinal xanthopachyonychia, woodworm cavities at free edge, transverse + longitudinal overcurvature, proximal splinter haemorrhages
- Nail avulsion reveals sea-anemone matrix tumour
- MRI/ultrasound/OCT helpful
Onychopapilloma:
- Benign longitudinal subungual tumour; presents as isolated pink longitudinal nail streak (erythronychia) with subungual keratosis and distal onycholysis
Malignant
Subungual Melanoma (Nail Apparatus Melanoma):
- 0.18-2.8% of all cutaneous melanomas; higher proportion in African/Asian/Native American populations (~25% of melanomas in Japanese/African Americans)
- Most melanomas arise from matrix (75%) → longitudinal melanonychia
- Histological subtype: usually acral lentiginous melanoma
- BRAF mutations LOW; KIT and NRAS mutations HIGH
- Hutchinson's sign (pigment extending to nail fold) = strongly suggestive of melanoma; pseudo-Hutchinson's sign = benign mimic (transparent cuticle showing nail bed pigment)
- Treatment: in situ → en bloc removal with 5-10mm margins; invasive → amputation guided by balance of tumour thickness and function
- Sentinel lymph node biopsy for melanoma >1mm thickness
Squamous Cell Carcinoma (most common malignant nail tumour):
- Mean age 60; 75% male
- HPV-associated (up to 60% genito-digital transmission; right index/middle fingers)
- Presents: subungual hyperkeratosis, onycholysis, oozing (underrecognised), nail plate destruction
- Bowen disease = in situ SCC; mean diagnosis delay 6 years
- Standard X-ray: bone involvement in 2-30%
- Treatment: Mohs surgery first line; amputation only if bone involved
Sources: Rook's Ch.93 pp 93.24-93.39; Fitzpatrick's Ch.91; Ricardo JW et al. JAAD 2025 Jul [PMID 40023404]
3.9 Traumatic Nail Disorders
| Condition | Description |
|---|
| Nail biting (onychophagia) | Compulsive behaviour; complications: herpetic whitlow, MRSA transfer, viral warts (Koebner) |
| Onychotillomania | Repetitive nail picking/manipulation; habit-tic deformity (washboard nails) |
| Onychogryphosis | Ram's horn / oyster nail; elderly (11-38% prevalence); causes: neglect, poor circulation, trauma, onychomycosis |
| Ingrowing toenail | Penetration of lateral nail fold by nail edge/spike; Stage 1 (pain/redness) → Stage 2 (seropurulent discharge) → Stage 3 (granulation tissue) |
| Retronychia | Nail embeds in PNF; new nail grows beneath; dislodges old nail upward; treatment: nail avulsion |
| Subungual haematoma | Post-traumatic; fringed distal edge on dermoscopy; purple-dark pooled blood |
| Median canaliform dystrophy of Heller | Midline fir-tree groove in nail; thumbs; often self-resolving |
Ingrowing toenail treatment:
- Stage 1 & 2: conservative (correct cutting habit, topical steroids for granulation, antiseptics, appropriate footwear)
- Stage 3 (refractory): chemical cautery with 88% phenol (partial avulsion + 4 min phenol application = <3% recurrence; several Cochrane reviews support this); TCA 100% equally effective but same oozing time
3.10 Nail Changes in Connective Tissue Diseases
| Disease | Nail Findings |
|---|
| Systemic sclerosis | Periungual telangiectasias; megacapillaries + avascular areas on capillaroscopy (4 stages); pterygium inversum unguis; acro-osteolysis on X-ray |
| SLE | Periungual erythema; splinter haemorrhages; onycholysis; ventral pterygium (rarely) |
| Dermatomyositis | Dilated irregular nail fold capillaries (pathognomonic); ragged cuticles (Gottron's sign equivalent) |
| Raynaud | Capillaroscopy: overactive vasomotor tone (primary); decreased (secondary) |
| Rheumatoid arthritis | Tortuous/ramified capillary loops in nail fold; "fish shoal" pattern |
3.11 Drug-Induced Nail Disorders
| Drug | Nail Change |
|---|
| Retinoids | Onycholysis, paronychia, ingrown toenails, PG, fragility |
| EGFR inhibitors (cetuximab, gefitinib) | Multiple pyogenic granulomas, paronychia |
| Taxanes (docetaxel, paclitaxel) | Multiple PGs, onycholysis, subungual haematoma, pain |
| Capecitabine | Onycholysis, pigmentation |
| Antiretrovirals (indinavir) | Paronychia, PG |
| Hydroxyurea | Melanonychia |
| β-blockers | Pincer nails, digital necrosis |
| ACE inhibitors (captopril) | Onycholysis |
| Methotrexate | Slower nail growth |
| Doxycycline/psoralens | Photo-onycholysis |
| Ciclosporin | Ingrown toenails, PG |
PART 4 — IMAGING OF THE NAIL
| Modality | Key Uses |
|---|
| X-ray | Subungual exostosis, acro-osteolysis, keratoacanthoma (cup-shaped erosion), bone involvement in SCC |
| Ultrasound (>15 MHz, hockey stick probe) | Real-time blood flow; solid vs cystic lesions; foreign bodies; glomus tumour; psoriatic enthesitis/dactylitis |
| MRI | Gold standard for glomus tumour; myxoid cysts; soft tissue masses; melanoma extent; 1mm resolution |
| Dermoscopy (onychoscopy) | Non-invasive; pitting, onycholysis patterns, capillaries, melanonychia evaluation |
| Capillaroscopy | Connective tissue disease (4-stage systemic sclerosis pattern); dermatomyositis megacapillaries |
| OCT | Very high resolution (5-10 μm) but low penetrance (2mm); onychomycosis monitoring |
| Reflectance Confocal Microscopy | In vivo/ex vivo for onychomycosis diagnosis and intraoperative melanonychia assessment |
PART 5 — NAIL SURGERY (Overview)
Anaesthesia: Distal digital block (1 cm proximal/lateral to PNF-lateral nail fold junction; 0.5 mL dorsal + 0.5 mL palmar branches × both sides)
Key procedures:
- Nail avulsion (partial preferred; total avulsion causes nail bed shrinkage and distal pulp expansion)
- Punch biopsy (3 mm for small pigmented lesion <3mm in distal matrix)
- Longitudinal ellipse excision (for longitudinal pigmented bands)
- Tangential excision (for wide pigmented areas)
- Lateral longitudinal biopsy (sigmoid-shaped; includes all lateral nail unit structures)
- Crescent-shaped PNF excision (chronic paronychia; heals by secondary intention in <2 weeks)
- Chemical cautery (88% phenol 4 min for ingrowing toenail; tourniquet mandatory for bloodless field; oozing lasts up to 5 weeks)
PART 6 — CLINICAL PEARLS 💎
-
The onychodermal band is the Achilles heel of nail plate attachment — once breached (psoriasis, trauma), onycholysis becomes progressive and difficult to reverse. Clipping, drying, and topical antiseptics are the cornerstone of management.
-
Chronic paronychia ≠ Candida infection. Candida is a secondary coloniser. The primary aetiology is irritant/allergic dermatitis. Systemic antifungals do NOT help — treat the inflammation first.
-
Proximal subungual onychomycosis (PSO) in a young patient = think HIV. PSO is the classic nail presentation in immunocompromised patients and should trigger HIV testing.
-
Nail-fold capillaroscopy distinguishes primary Raynaud from secondary Raynaud (connective tissue disease). Megacapillaries + avascular areas = secondary (scleroderma pattern); normal capillary architecture = primary Raynaud disease.
-
Pseudo-Hutchinson's sign: Periungual pigmentation that simulates Hutchinson's sign but is actually visible nail plate pigmentation through a transparent cuticle. Seen in racial melanonychia, benign nevi. The real Hutchinson's sign = actual extension of melanin pigment into the nail fold skin.
-
Glomus tumour triad = Love test (point tenderness) + Hildreth's sign (tourniquet pain relief) + cold sensitivity. Affects predominantly women under age 40. If you feel a mismatch of pain severity to clinical exam, think glomus tumour.
-
Darier disease candy-cane nails = red + white longitudinal bands with V-notch at free edge. This is pathognomonic and can be diagnosed even when nail is the only manifestation of Darier disease.
-
Nail psoriasis is HLA-Cw6 negative — opposite of cutaneous plaque psoriasis. This suggests a genetically distinct subset with stronger association with psoriatic arthritis.
-
Koenen tumours (periungual fibromas) of tuberous sclerosis develop around puberty, histologically identical to acquired ungual fibrokeratomas, but LACK the hyperkeratotic tip.
-
Nail melanoma in dark-skinned individuals: ~25% of all melanomas in Japanese and African Americans are nail apparatus melanomas. The absolute incidence may be similar across races, but proportionately nails matter much more in these populations.
-
The free edge of the nail reveals where pigment originates: pigment in upper portion of free edge → proximal/dorsal matrix origin (higher risk of dystrophy post-biopsy); pigment in lower portion → distal matrix (safer to biopsy, less post-biopsy dystrophy).
-
SCC is the most common malignant nail tumour, not melanoma. HPV-associated (genito-digital route); right index finger is most commonly affected. Mean diagnosis delay = 6 years.
-
Onychomycosis in toenails does NOT cure with topical treatment alone in most cases. Systemic terbinafine is the most effective single agent. Always get a KOH/culture before treating — misdiagnosis rate is significant.
-
Beau lines at same level in all 20 nails = systemic cause (cytotoxics, severe illness). Beau lines on only 1-2 nails = local trauma or paronychia.
-
The distal digital block, not a ring block, is the preferred anaesthesia for nail surgery — dual innervation requires addressing both dorsal and palmar nerve branches at the lateral digit, not the classic ring block which may miss dorsal branches.
PART 7 — VIVA QUESTIONS & ANSWERS
Q1. Describe the layers of the nail plate and their origin.
A: The nail plate is a trilaminar structure: (1) dorsal plate — from ventral aspect of proximal nail fold; (2) intermediate/main plate — from germinal matrix (main contributor); (3) ventral plate — from nail bed (contributes ~21% thickness). The proximal matrix generates the dorsal plate while the distal matrix (lunula) generates the ventral plate. Hard hair-type keratins are embedded in sulfur-rich proteins (high cysteine/glycine/tyrosine). [Rook's Ch.93; Bolivnia 5e]
Q2. What is the onychodermal band and why is it clinically important?
A: The onychodermal band (nail isthmus) is the most distal zone of cornified epithelium attached to the undersurface of the nail plate — the structural anchor for nail plate to nail bed adhesion. It appears as a yellowish-white margin proximal to the free edge. Once breached — as in psoriasis, trauma, or infection — nail plate separation (onycholysis) becomes progressive and is difficult to reverse. [Rook's Ch.93 p.93.2]
Q3. What are the causes of proximal subungual onychomycosis (PSO) and why is it important?
A: PSO is infection entering via the proximal nail fold, presenting as leukonychia beginning at the lunula and extending distally. The most important organism is Trichophyton rubrum. PSO is strongly associated with HIV/immunosuppression — a young, otherwise healthy patient with PSO should be tested for HIV. Rare in immunocompetent individuals. [Rook's Ch.93; Fitzpatrick's Ch.91]
Q4. Enumerate the criteria for ABCDEF assessment of longitudinal melanonychia.
A: Age (40-70, African/Asian/Native American), Brown/Black >3mm width with Blurred borders, Change in band morphology/colour, Digit (thumb > hallux > index finger; single digit involvement), Extension to nail fold (Hutchinson's sign), Family/personal history of melanoma. This guides the decision for biopsy. [Fitzpatrick's Ch.91; Ricardo JW et al. JAAD 2025]
Q5. What is the difference between Hutchinson's sign and pseudo-Hutchinson's sign?
A: Hutchinson's sign = actual extension of melanin pigment from the nail matrix into the periungual skin (PNF, lateral folds, cuticle) — strongly suggestive of subungual melanoma. Pseudo-Hutchinson's sign = apparent periungual pigmentation due to transparency of the cuticle revealing the underlying nail plate pigmentation — seen in racial/ethnic melanonychia, benign nevi, Laugier-Hunziker syndrome. Dermoscopy distinguishes the two. [Fitzpatrick's Ch.91; Rook's Ch.93]
Q6. What are the four dermoscopic patterns of onycholysis and their significance?
A: (1) Post-traumatic — regular margin, usually lateral (where the first toenail hits the second); (2) Psoriatic — irregular margin involving the whole free edge with an erythematous border; (3) Onychomycosis — ragged/spike "dermato" edge with mycelium visible in a proximal direction; (4) Drug-induced — uniform pattern in the midline (photo-onycholysis). [Rook's Ch.93 Fig. 93.11]
Q7. Describe the clinical features of glomus tumour under the nail. How do you investigate it?
A: Glomus tumour presents with severe pulsating pain (worse at night, cold-triggered, radiating to shoulder) and either: (a) a small reddish/bluish spot under the nail, or (b) longitudinal erythronychia with distal notching/fissure. Clinical triad: Love test (point tenderness), Hildreth's sign (tourniquet relieves pain), cold sensitivity. Investigation: MRI (gold standard — highest sensitivity, determines exact spatial location for excision). High-resolution ultrasound with Doppler as alternative. Bone erosion occurs in 50%. [Rook's Ch.93 pp 93.26-93.27]
Q8. What are the nail changes of Darier disease and what makes them pathognomonic?
A: Multiple red (erythronychia) and white (leukonychia) longitudinal bands resembling candy-canes in multiple nails — this combination is pathognomonic for Darier disease. At the free margin, the bands have a V-shaped notch and fissure (fragility). In severe cases, the nail may be almost completely lost. Histology shows acantholysis similar to skin disease, plus multinucleate giant cells and epithelial hyperplasia in the nail bed. Darier disease can be diagnosed from nails alone. [Rook's Ch.93 pp 93.50-93.51]
Q9. Compare and contrast acute and chronic paronychia.
A: Acute paronychia — rapid onset; exquisite pain/swelling/erythema; most common cause: Staphylococcus aureus; treat with drainage ± antibiotics. Chronic paronychia — insidious; predominantly in wet-work workers/females; loss of cuticle; Beau lines/cross-ridging; Candida is a secondary coloniser, NOT primary pathogen; systemic antifungals are useless; treat with anti-inflammatory approach (topical steroids/imidazoles), avoidance of wet work; surgical crescent excision if refractory. [Rook's Ch.93 pp 93.40-93.44]
Q10. What is Schamroth's window test and how does it demonstrate clubbing?
A: When the dorsal aspects of two homologous fingers from opposite hands are opposed, a diamond-shaped window of light bordered laterally by the Lovibond angles is normally visible. In clubbing, as Lovibond's angle increases to >180°, this window is obliterated. It is a bedside clinical test for clubbing. [Rook's Ch.93 Fig. 93.7]
Q11. Describe the nail changes of psoriasis according to the Zaias classification.
A: Based on anatomical site: Matrix involvement → pitting (proximal matrix, episodic), transverse furrows (proximal matrix, 1-2 weeks), crumbling (entire matrix, prolonged), leukonychia. Nail bed involvement → splinter haemorrhages (short), oil spot/salmon patch/onycholysis (prolonged), subungual hyperkeratosis (prolonged), false nail, yellow/green discoloration. Nail fold involvement → periungual inflammation (associated with psoriatic arthritis). [Rook's Ch.93 Table 93.4]
Q12. What are the HLA associations in nail psoriasis vs cutaneous psoriasis?
A: Cutaneous plaque psoriasis is positively correlated with HLA-Cw6. Nail psoriasis patients are more frequently HLA-Cw6 NEGATIVE, indicating a separate genotype. HLA-Cw6-positive patients have milder nail involvement. Asian patients with nail psoriasis show increased HLA-B46 and HLA-A*02:07. This suggests nail psoriasis is a genetically distinct disease entity with stronger association with psoriatic arthritis. [Rook's Ch.93 p.93.45]
Q13. What is the NAPSI score?
A: The Nail Psoriasis Severity Index scores each nail from 0-8 based on matrix features (pitting, leukonychia, red spots in lunula, nail plate crumbling) and nail bed features (oil drop/onycholysis, subungual hyperkeratosis, splinter haemorrhages, nail bed discolouration) — each scored 0-4 per nail (0=none, 1=1/4 nail, 2=2/4, 3=3/4, 4=4/4). Total maximum score = 160 (80 fingernails + 80 toenails). [Standard scoring; referenced in Rook's Ch.93]
Q14. Name the causes of apparent leukonychia and their systemic significance.
A: Muehrcke's lines (paired transverse white bands that disappear with pressure) = hypoalbuminemia; Terry's nails (white proximally, normal 1-2mm distally) = hepatic cirrhosis; half-and-half nails/Lindsay's nails (proximal white, distal red-brown) = chronic renal failure; azure lunula = Wilson's disease/argyria; in all apparent leukonychia, changes are in the nail bed (not plate) and disappear with pressure. [Bolivnia 5e p.1447; Fitzpatrick's Ch.91]
Q15. What are the four clinical types of digital myxoid pseudocyst (synovial cyst) and their nail significance?
A: De Berker classification: Type A (nodule between DIP and PNF — most common); Type B (in PNF → pressure on matrix → longitudinal groove in nail, varies with cyst size — must distinguish from fibrokeratoma); Type C (under matrix → reddish/bluish lunula — requires ultrasound/MRI). All result from leakage of synovial fluid through a breached DIP joint capsule (confirmed on MRI in >85%). [Rook's Ch.93 pp 93.28-93.29]
PART 8 — QUIZ (Side-by-Side with Answers)
| # | Question | Answer |
|---|
| 1 | What is the normal fingernail growth rate? | 3 mm/month |
| 2 | Which matrix zone produces the ventral nail plate? | Distal matrix (lunula) |
| 3 | The onychodermal band is also called the: | Nail isthmus |
| 4 | Lovibond's angle in clubbing exceeds: | 180° |
| 5 | Koilonychia is most commonly associated with which systemic deficiency? | Iron deficiency (anaemia) |
| 6 | Which keratin pair is abnormally expressed in nail bed in psoriasis/onychomycosis (indicating granular layer formation)? | K1/K10 |
| 7 | Chronically reduced nail growth + yellow nails + lymphoedema + pleural effusion = ? | Yellow nail syndrome |
| 8 | In chronic paronychia, what is the PRIMARY pathogen? | None (irritant/allergic dermatitis); Candida is secondary coloniser |
| 9 | What is the most common organism in DLSO onychomycosis? | Trichophyton rubrum |
| 10 | PSO (proximal subungual onychomycosis) in a young patient should prompt testing for: | HIV |
| 11 | Candy-cane nails (red + white longitudinal bands + V-notch at free margin) = ? | Darier disease |
| 12 | Pterygium of nail is most characteristically seen in: | Lichen planus |
| 13 | Which nail sign is pathognomonic for tuberous sclerosis? | Koenen tumours (periungual fibromas), develop around puberty |
| 14 | Triangular lunulae are pathognomonic of: | Nail-patella syndrome (LMX1B gene mutation) |
| 15 | Nail fold capillaroscopy showing megacapillaries + avascular areas + hazy background is characteristic of: | Systemic sclerosis (scleroderma) |
| 16 | The most common MALIGNANT tumour of the nail unit is: | Squamous cell carcinoma (not melanoma) |
| 17 | Most nail melanomas in African/Asian patients arise from: | Nail matrix (75%) → presents as longitudinal melanonychia |
| 18 | Hutchinson's sign is defined as: | Extension of melanin pigment into periungual skin (nail fold), strongly suggestive of subungual melanoma |
| 19 | Gold standard imaging for glomus tumour: | MRI |
| 20 | NAPSI maximum total score: | 160 (80 fingernails + 80 toenails) |
| 21 | FDA-approved biologic specifically for nail psoriasis: | Adalimumab (anti-TNF) |
| 22 | What is the significance of Muehrcke's lines disappearing with pressure? | They are "apparent leukonychia" (nail bed, not nail plate changes) — caused by hypoalbuminemia/oedema |
| 23 | Nail pitting histologically represents: | Foci of parakeratosis in the proximal nail matrix |
| 24 | HPV genito-digital transmission accounts for what proportion of nail SCC? | Up to 60% |
| 25 | Which drug is the most effective single agent for toenail onychomycosis? | Oral terbinafine (250mg/day × 12 weeks) |
| 26 | Chemical cautery time for phenol in ingrowing toenail matricectomy: | 4 minutes with tourniquet; oozing lasts up to 5 weeks |
| 27 | What is the ABCDEF rule "E" for longitudinal melanonychia? | Extension of pigment to the nail fold (Hutchinson's sign) |
| 28 | Nail psoriasis HLA association: | HLA-Cw6 NEGATIVE (opposite of skin psoriasis) |
| 29 | Crescent-shaped excision of proximal nail fold is used for: | Chronic paronychia (refractory cases) |
| 30 | Green discolouration under an onycholytic nail is caused by: | Pseudomonas aeruginosa (pyocyanin pigment) |
REFERENCES / SOURCES PER SECTION
| Section | Source |
|---|
| Gross anatomy, microscopic anatomy, blood/nerve supply, growth | Rook's Dermatology 9e, Ch.93 (Pasch, Richert & Iorizzo), pp 93.2-93.6 |
| Nail signs, clubbing, koilonychia, colour changes | Rook's Ch.93 pp 93.7-93.18 |
| Nail unit anatomy diagram (detailed) | Dermatology 5e (Bolivnia), Ch.71 (Tosti & Piraccini), Fig. 68.7/71.1, pp 1382-1384 |
| Nail signs table | Bolivnia Dermatology 5e, Fig.71.2, p.1443 |
| Beau lines, systemic significance | Bolivnia 5e p.1443 |
| Nail disorders chapter overview | Fitzpatrick's Dermatology, Ch.91 (Haneke), pp 2420-2530 |
| Chromonychia (leukonychia, colour changes) | Fitzpatrick's Ch.91 pp 2442-2450 |
| Lichen planus of nails, treatment | Andrews' Diseases of the Skin, Ch.33 pp 501-519 |
| Nail-patella syndrome, hapalonychia | Andrews' Ch.33 pp 911-922 |
| Yellow nail syndrome | Andrews' Ch.33 pp 1250-1271 |
| Onychomycosis treatment | Goodman & Gilman's (pharmacology); Goldman-Cecil Medicine Ch.59; Fitzpatrick's Ch.91 |
| Nail psoriasis treatment algorithm | Rook's Ch.93 Fig. 93.69; Hwang JK et al. JAAD 2024 [PMID 38007038] |
| Onychomycosis review | Zaraa I et al. Hand Surg Rehabil 2024 [PMID 38218374] |
| Longitudinal melanonychia evaluation | Ricardo JW et al. JAAD 2025 Jul [PMID 40023404] |
Recent evidence note: A 2024 JAAD review by
Hwang JK, Grover C, Iorizzo M provides updated diagnostic criteria and management algorithms for nail psoriasis and nail lichen planus, confirming the superiority of biologics (especially IL-17 and IL-23 inhibitors) over conventional systemics for nail psoriasis. A 2025 JAAD expert group review by
Ricardo JW et al. updates the clinical evaluation approach for longitudinal melanonychia.