kindly explain briefly about DIC
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a concise overview of Disseminated Intravascular Coagulation (DIC):
Disseminated Intravascular Coagulation (DIC)
Definition
DIC is an acquired clinicopathologic syndrome in which the coagulation and fibrinolytic systems are simultaneously activated, leading to widespread thrombin and plasmin formation, consumption of clotting factors and platelets, fibrin deposition in small vessels, and paradoxical bleeding. — Henry's Clinical Diagnosis and Management by Laboratory Methods
Pathophysiology
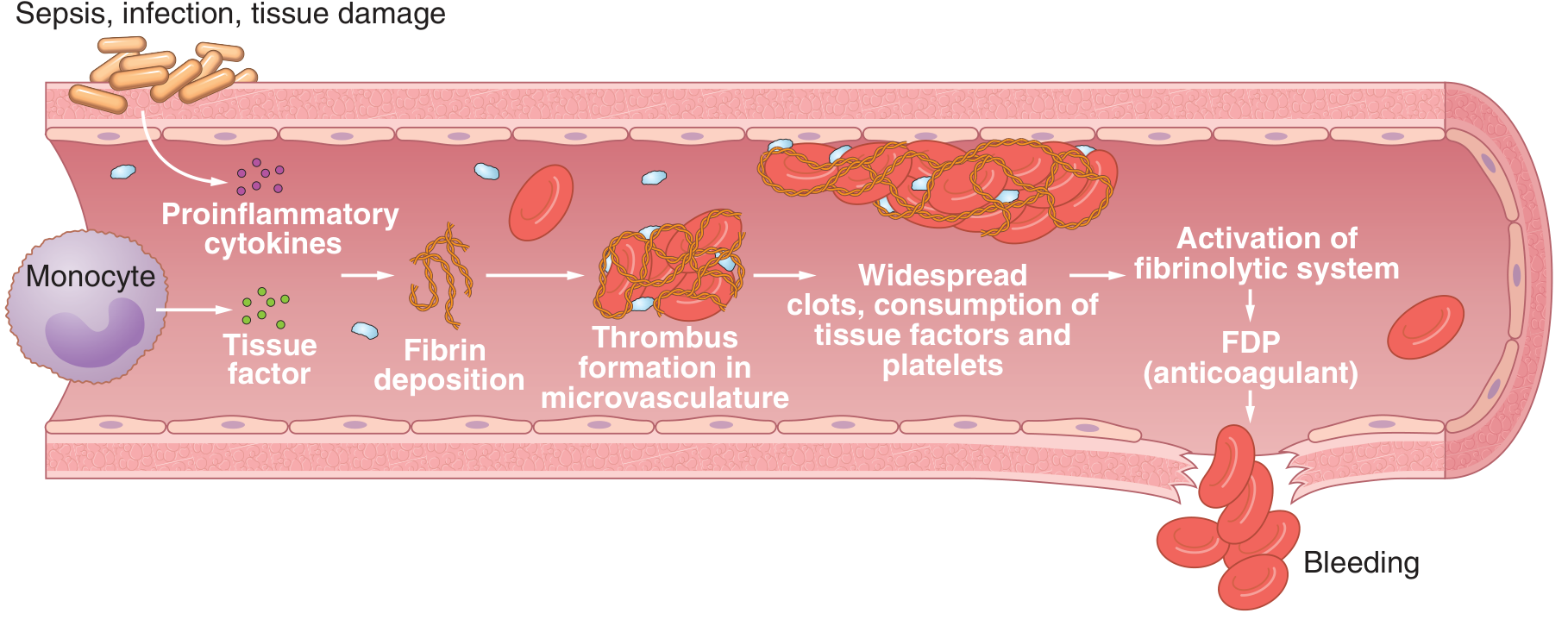
The sequence of events:
- Trigger (sepsis, tissue injury, etc.) → release of tissue factor and proinflammatory cytokines
- Activation of the coagulation cascade → massive thrombin generation
- Fibrin deposition in small vessels → microthrombi → organ ischemia
- Consumption of platelets, fibrinogen, and factors V, VIII, XIII
- Activation of the fibrinolytic system → plasmin lyses fibrin → fibrin degradation products (FDPs) released
- FDPs impair platelet function and fibrin polymerization → bleeding tendency
The net result is the paradox of simultaneous clotting and bleeding. — Guyton & Hall Textbook of Medical Physiology
Common Causes (Triggers)
| Category | Examples |
|---|---|
| Sepsis / Infection | Gram-negative bacteria (endotoxin), gram-positive, fungemia |
| Obstetric | Abruptio placentae, amniotic fluid embolism, retained dead fetus, HELLP syndrome |
| Malignancy | Acute leukemia, solid tumors |
| Massive tissue injury | Trauma, burns, major surgery |
| Transfusion reactions | Acute hemolytic reactions |
— Henry's Clinical Diagnosis and Management by Laboratory Methods
Clinical Features
- Bleeding: from puncture sites, wounds, mucosal surfaces, and deep tissues (petechiae, ecchymoses)
- Thrombosis: organ ischemia (kidneys, lungs, brain, skin necrosis, acral ischemia)
- Signs of organ dysfunction: oliguria/renal failure, confusion, respiratory distress
- Microangiopathic hemolytic anemia (MAHA): schistocytes and helmet cells on blood smear
Laboratory Findings
| Test | Finding in DIC |
|---|---|
| PT / APTT | Prolonged |
| Platelet count | Decreased (<100 k/µL, often <50 k/µL) |
| Fibrinogen | Decreased (<100 mg/dL) |
| D-dimer | Markedly elevated |
| Blood smear | Schistocytes, helmet cells |
ISTH Scoring System (overt DIC): Score ≥5 is diagnostic
- Platelets: >100k=0, <100k=1, <50k=2
- D-dimer: normal=0, moderate rise=2, strong rise=3
- PT prolongation: <3s=0, 3–6s=1, >6s=2
- Fibrinogen: >1g/L=0, <1g/L=1
— Henry's Clinical Diagnosis and Management by Laboratory Methods
Management
- Treat the underlying cause — this is the most critical step; many episodes are self-limited once the trigger is removed
- Replacement therapy (for active bleeding):
- Fresh Frozen Plasma (FFP) — replenishes clotting factors
- Platelet transfusion — if count is very low
- Cryoprecipitate — replaces fibrinogen, factor VIII, factor XIII
- Heparin — considered when thrombosis predominates (e.g., purpura fulminans, retained dead fetus, giant hemangioma); used cautiously
- Monitor: platelet count, fibrinogen, FDPs/D-dimer, clotting times
— ROSEN's Emergency Medicine
Key Distinction from Similar Conditions
| Feature | DIC | Severe Liver Disease | Primary Fibrinolysis |
|---|---|---|---|
| Platelets | ↓↓ | ↓ | Normal/near-normal |
| Factor V & VIII | ↓ | ↓ | Normal/near-normal |
| D-dimer | ↑↑ | Variable | ↑ |
| Schistocytes | Present | Absent | Absent |
In summary, DIC is a life-threatening syndrome driven by a primary illness that overwhelms normal hemostatic control. The simultaneous bleeding and clotting make it clinically challenging. Early recognition, diagnosis by scoring, and aggressive treatment of the underlying cause are the cornerstones of management.
This is a shared conversation. Sign in to Orris to start your own chat.