Auto peep for md anaesthesia exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive MD anaesthesia exam answer on Auto-PEEP. Here is the complete structured response:
Auto-PEEP (Intrinsic PEEP) — MD Anaesthesia Exam
Definition
Auto-PEEP (also called intrinsic PEEP / iPEEP / occult PEEP) is the positive alveolar pressure that remains at end-expiration above the set (extrinsic) PEEP, due to incomplete lung emptying before the next breath begins.
"This positive end-expiratory pressure (PEEP) in the alveoli at rest has been termed auto-PEEP or intrinsic PEEP." — Miller's Anesthesia, 10e
Formally: Auto-PEEP = Total PEEP − Set PEEP
Pathophysiology / Mechanism
Normal expiration ends when alveolar pressure equilibrates with atmospheric pressure (FRC is reached). Auto-PEEP arises when expiration is cut short before this equilibration, causing dynamic hyperinflation — i.e., end-expiratory lung volume rises above the static FRC.
The major determinants are:
| Factor | Direction | Effect |
|---|---|---|
| ↑ Minute ventilation | Worsens | Less time per breath |
| ↑ Expiratory airway resistance | Worsens | Slower emptying |
| ↑ Respiratory system compliance | Worsens | Longer time constant |
| ↓ Expiratory time (↑ I:E ratio) | Worsens | Incomplete exhalation |
| ↑ Tidal volume | Worsens | More volume to exhale |
| Expiratory flow limitation | Worsens | Especially in COPD/emphysema |
— Goldman-Cecil Medicine
Why Auto-PEEP Is Not Detected on Standard Ventilators
The pressure drop that creates auto-PEEP occurs across the airways proximal to the alveoli. Standard ventilator manometers measure pressure at the airway opening (circuit side), not in the alveoli. When the expiratory valve is open and flow is present, the gradient cannot be seen.
"The presence of auto-PEEP is not detected by the manometer of standard anesthesia ventilators." — Miller's Anesthesia, 10e
This is why auto-PEEP is sometimes called "occult PEEP".
Conditions Where Auto-PEEP Occurs
- COPD / emphysema — the classic setting; decreased elastic recoil + flow limitation
- Acute severe asthma — high airway resistance, bronchospasm
- ARDS — elevated time constants in heterogeneous lung
- Sepsis with respiratory muscle weakness
- One-lung ventilation (OLV) — commonly 4–6 cmH₂O in lung cancer/COPD patients
- High respiratory rate on mechanical ventilation (e.g., assist-control)
- Post-intubation period — compensatory venous tone lost due to drugs
Measurement of Auto-PEEP
1. End-Expiratory Occlusion Maneuver (Gold Standard)
- Occlude the expiratory port at end-exhalation for <4 seconds
- Pressures equilibrate across the circuit; the ventilator manometer now reads total PEEP
- Auto-PEEP = reading on manometer − set PEEP
- Only valid in passive (non-spontaneously breathing) patients
2. Flow-Time Waveform
- Observe the expiratory flow waveform — if flow has not returned to zero before the next breath begins, auto-PEEP is present
3. Esophageal Balloon (Spontaneously Breathing Patients)
- Measures pleural pressure; auto-PEEP = the negative deflection in Poes the patient must generate before inspiratory flow starts
4. Dynamic Hyperinflation Volume
- Prolonged expiration (20–30 sec) releases the trapped volume — measured as the excess volume above normal tidal expiration
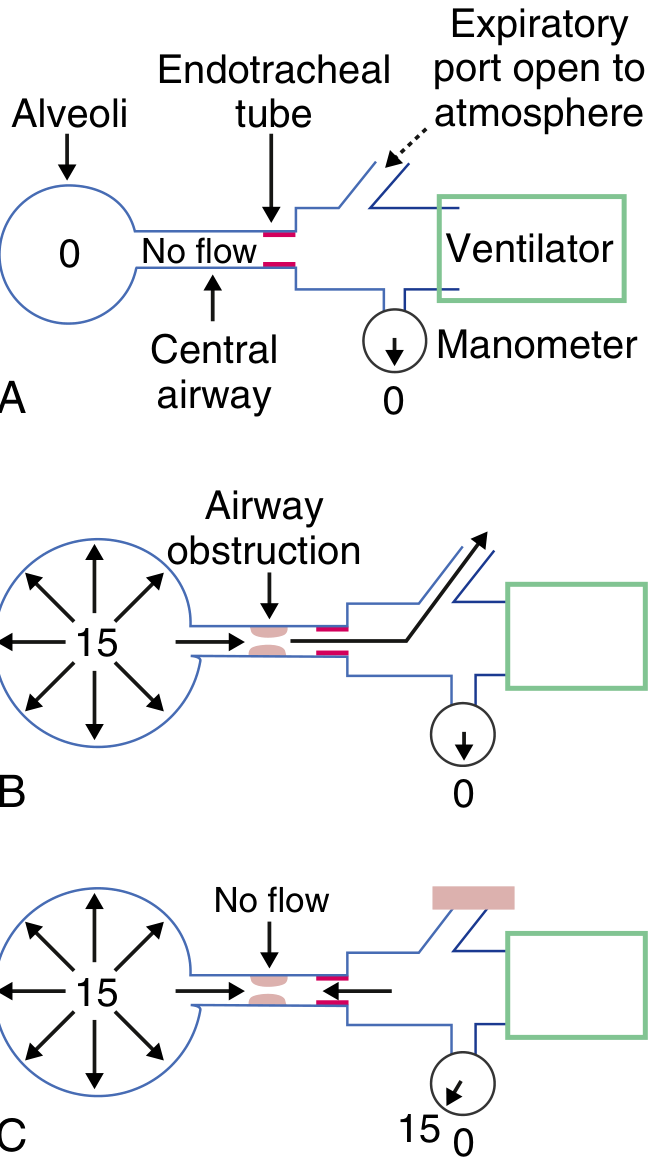
A = Normal (no auto-PEEP, alveolar = 0). B = Obstruction, expiratory port open (alveoli = 15, manometer = 0 — auto-PEEP hidden). C = Expiratory port occluded — pressures equilibrate, manometer reads 15 cmH₂O = auto-PEEP revealed. (Modified from Pepe & Marini, Am Rev Respir Dis, 1982)
Clinical Consequences
Haemodynamic
- ↑ Intrathoracic pressure → ↑ right atrial pressure → ↓ venous return → ↓ cardiac output → hypotension
- Especially dangerous immediately after intubation (compensatory mechanisms blunted by anaesthetic drugs)
- Can mimic tension pneumothorax
Respiratory Mechanics
- Triggers inspiratory failure — patient must first generate pressure to overcome auto-PEEP before triggering the ventilator → ineffective efforts (>10% of efforts in ~25% of PSV patients)
- Ventilator respiratory rate appears lower than the patient's true rate
- False low compliance readings if auto-PEEP is not accounted for
- ↑ Work of breathing during spontaneous respiration — intrapleural pressure must drop below auto-PEEP level before inspiratory flow starts
- Barotrauma / volutrauma risk if unrecognised
One-Lung Ventilation (OLV) Specific
- Auto-PEEP of 4–6 cmH₂O is common; can partially counteract the FRC-reducing effects of lateral positioning
- External PEEP interaction is complex — patients with low auto-PEEP (<2 cmH₂O) experience greater increase in total PEEP from external PEEP than those with high auto-PEEP (>10 cmH₂O)
Management / How to Minimise Auto-PEEP
| Strategy | Mechanism |
|---|---|
| ↓ Respiratory rate | ↑ Expiratory time per cycle |
| ↑ Expiratory time (↓ I:E ratio, e.g., 1:3 or 1:4) | More time to empty |
| ↓ Tidal volume | Less volume to exhale per breath |
| Bronchodilators (β₂ agonists, anticholinergics) | ↓ Airway resistance |
| Sedation / muscle relaxation | Eliminates active expiratory muscle activity prolonging obstruction |
| Disconnect from ventilator briefly | Allows complete passive exhalation; can diagnose and treat simultaneously |
| External PEEP (in spontaneous breathing patients) | Reduces trigger threshold (stenting open airways to within ~75–85% of auto-PEEP level so patient doesn't have to overcome entire iPEEP) |
| Permissive hypercapnia | Allows ↓ minute ventilation to prioritise lung emptying |
"Minimizing auto-PEEP, which is a fundamental principle in ventilating patients who have severe airway obstruction, can best be achieved by decreasing minute ventilation, increasing expiratory time, and decreasing airway resistance." — Goldman-Cecil Medicine
External PEEP in the Presence of Auto-PEEP
A key exam concept: applying external (set) PEEP to a spontaneously breathing patient with auto-PEEP does not simply add to total PEEP (as it would in a passive patient). Instead, it reduces the inspiratory trigger work by stenting the airway open to a pressure approaching but not exceeding auto-PEEP. The threshold for triggering the ventilator falls. However, if external PEEP exceeds auto-PEEP, total PEEP rises and further hyperinflation occurs.
Relationship to Driving Pressure
- Total PEEP (set PEEP + auto-PEEP) must be used in the driving pressure calculation:
$$\Delta P = P_{plat} - \text{Total PEEP}$$
- Ignoring auto-PEEP causes underestimation of driving pressure and underestimation of tidal stress on lung tissue
- Driving pressure >15 cmH₂O is associated with ↑ mortality in ARDS
Quick Memory Summary for Exam
| Definition | Alveolar pressure > atmospheric at end-expiration (above set PEEP) |
| Formula | Auto-PEEP = Total PEEP − Set PEEP |
| Classic setting | COPD + mechanical ventilation |
| Not detected | Standard anaesthesia ventilator manometer |
| Detected by | End-expiratory occlusion; flow not returning to zero |
| Haemodynamic effect | ↓ Venous return → ↓ CO → hypotension |
| Trigger effect | Patient cannot trigger ventilator (ineffective efforts) |
| Treatment | ↓ RR, ↑ expiratory time, ↓ VT, bronchodilators, disconnect |
| External PEEP role | Reduces trigger work in spontaneous breathers; does NOT simply add |
Sources: Miller's Anesthesia 10e; Goldman-Cecil Medicine International Edition; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.