PCOS management
Reading File
Finding Sources
Searching PubMed
"polycystic ovary syndrome" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information to provide a detailed, well-structured response on PCOS management. Let me compile the answer.
Polycystic Ovary Syndrome (PCOS) - Management
Diagnosis First: Rotterdam Criteria
PCOS is diagnosed when 2 of 3 criteria are met (after excluding other causes):
- Ovarian dysfunction - oligomenorrhea or amenorrhea
- Hyperandrogenism (HA) - clinical (hirsutism, acne, alopecia) or biochemical (elevated bioavailable testosterone)
- Polycystic ovarian (PCO) morphology on ultrasound - ≥20 follicles in either ovary measuring 2-9 mm and/or ovarian volume >10 mL
This yields four phenotypes: HA + ovarian dysfunction + PCO morphology; HA + ovarian dysfunction; HA + PCO morphology; or ovarian dysfunction + PCO morphology alone.
Diagnoses to exclude before confirming PCOS:
- Hyperprolactinemia
- Nonclassic congenital adrenal hyperplasia (check basal follicular-phase 17-OHP)
- Cushing's syndrome
- Androgen-secreting neoplasm
- Thyroid disorder
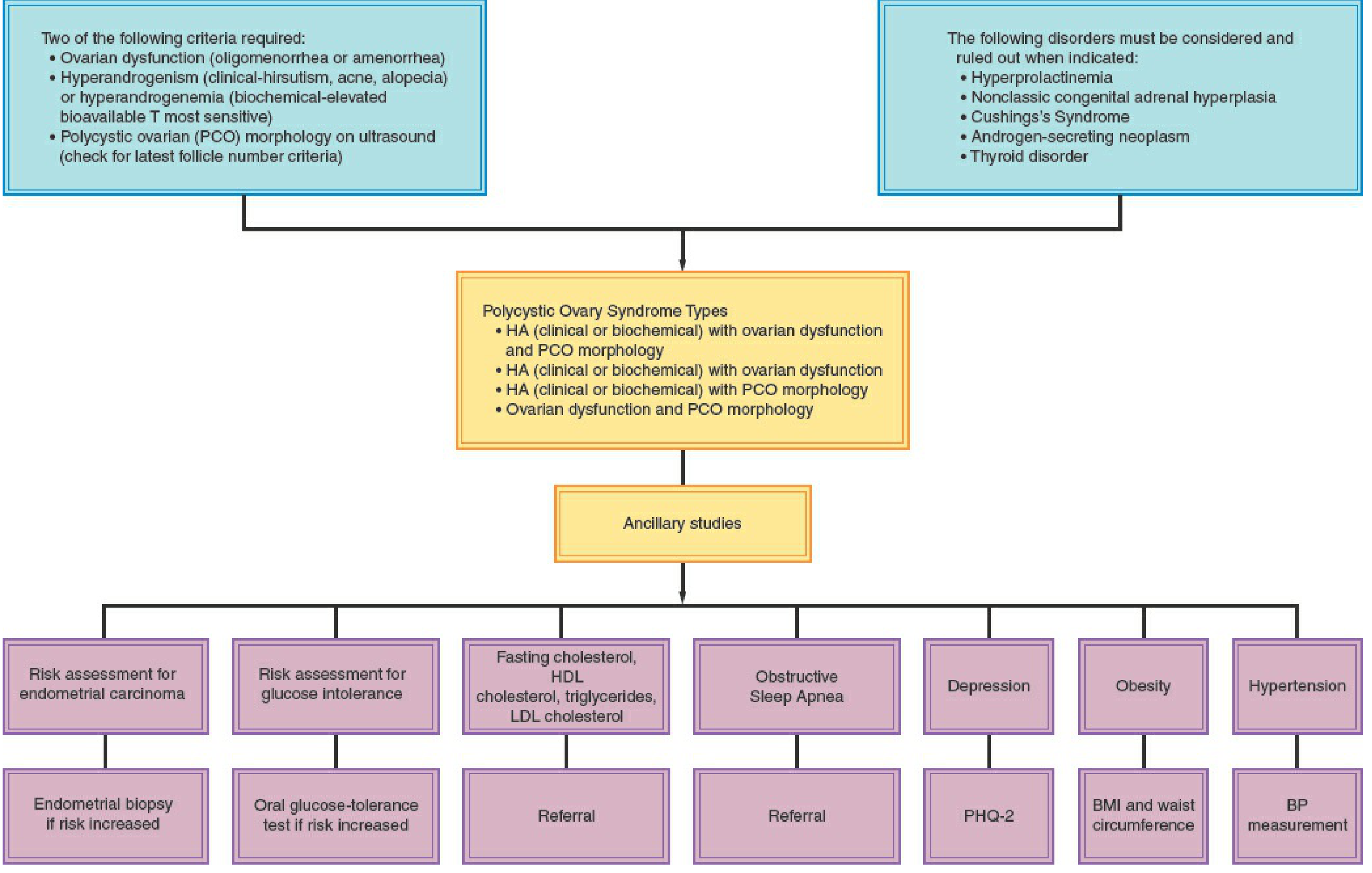
Initial Assessment (All Women with PCOS)
Screen at diagnosis and at regular intervals for:
| Parameter | Method |
|---|---|
| Obesity / central adiposity | BMI + waist circumference at every visit |
| Glucose intolerance / T2DM | 2-hour 75g OGTT (preferred over HbA1c alone) |
| Dyslipidemia | Fasting lipid profile (reassess every 2 years) |
| Hypertension | BP at every visit (target <120/80) |
| Depression & anxiety | PHQ-2 screen |
| Endometrial protection risk | Endometrial biopsy if anovulation is prolonged |
| Obstructive sleep apnea | Refer if suspected |
- 30-45% of obese PCOS women have glucose intolerance or T2DM
- Dyslipidemia is present in up to 70% of PCOS women (decreased HDL, elevated triglycerides, altered LDL quality)
- Acanthosis nigricans is a clinical marker of insulin resistance (IR)
1. Lifestyle Management (First-Line for All)
Recommended for all women with PCOS regardless of weight. In overweight/obese women, even modest weight loss (5-10%) can restore ovulation and improve metabolic and hormonal parameters.
- Structured exercise + dietary modification
- Targets: reduce central adiposity, improve IR, lower androgen levels
- A 2025 systematic review (PMID 39861440) confirms lifestyle interventions improve hormonal balance, insulin sensitivity, and menstrual regularity
2. Management Based on Presenting Goal
A. Menstrual Regulation / Endometrial Protection (Not Seeking Pregnancy)
Combined oral contraceptives (COCs) - first-line:
- Regulate cycles and reduce androgens by increasing SHBG, reducing LH, and inhibiting 5α-reductase
- Prefer formulations with newer progestins (desogestrel, gestodene, norgestimate, drospirenone) which have minimal androgenic activity
- Avoid norgestrel, norethindrone - these are androgen-dominant progestins
- Use lowest effective estrogen dose, either cyclic or continuous
- Alternatively: medroxyprogesterone acetate (MPA) 10 mg or progesterone 200 mg for 10-14 days every ≥3 months, or levonorgestrel IUD
Harrison's 22e notes: COCs are first-line for women not attempting pregnancy; metformin alone is NOT recommended for endometrial protection.
B. Hyperandrogenism (Hirsutism / Acne)
- COCs - initial therapy; allow 6 months before assessing response
- If inadequate response after 6 months, add antiandrogens:
- Spironolactone (50-200 mg/day) - most commonly used; blocks androgen receptors and inhibits 5α-reductase. Requires contraception (teratogenic)
- Flutamide - non-steroidal antiandrogen; liver toxicity risk limits use
- Finasteride (5α-reductase inhibitor) - less effective than spironolactone
- GnRH agonists (e.g., leuprolide) - reserved for severe/refractory hirsutism; suppress ovarian androgens to castrate levels. Add "add-back" estrogen/OC to prevent bone loss
- Dexamethasone - for adrenal or mixed adrenal/ovarian hyperandrogenism; very low doses (0.25 mg at bedtime)
- Physical methods (laser, electrolysis) - adjunctive cosmetic treatment; do not treat the underlying cause
Note: COC monotherapy has a relatively low success rate (<10%) for hirsutism in PCOS; combination with an antiandrogen is often needed for significant cases.
C. Metabolic / Insulin Resistance Management
Metformin:
- Consider in overweight/obese women for prevention of cardiometabolic risk factors
- Useful adjunct with diet and exercise; indicated for impaired glucose tolerance or T2DM
- NOT recommended as monotherapy for hyperandrogenism, endometrial protection, or infertility
GLP-1 Receptor Agonists (emerging):
- A 2024 meta-analysis (PMID 39178623) shows GLP-1 agonists (e.g., semaglutide) promote significant weight loss and improve hormonal parameters in obese PCOS women - increasingly used in this population
Dyslipidemia: treat per standard cardiovascular guidelines (statins if indicated)
D. Fertility / Ovulation Induction
First-line through third-line:
- Letrozole (aromatase inhibitor) - first-line for ovulation induction; superior to clomiphene for live birth rates in PCOS
- Clomiphene citrate (SERM) - second-line; with or without metformin
- Injectable gonadotropins - used judiciously by specialists; risk of ovarian hyperstimulation syndrome (OHSS) is elevated in PCOS - target monofollicular growth
- Laparoscopic ovarian drilling (LOD) - surgical option for clomiphene-resistant anovulation; can restore ovulation via reduction of ovarian androgen production
- IVF - for treatment failures or where other indications coexist
Pre-pregnancy counseling: women with PCOS have increased risk of miscarriage, gestational diabetes, gestational hypertension, preeclampsia, and preterm birth. Lifestyle optimization before conception is recommended.
3. Special Populations
Adolescents
- Diagnosis should require both persistent anovulation AND clinical/biochemical HA (PCO morphology alone is insufficient in adolescents)
- Distinguish from normal pubertal development
Pregnancy
- PCOS and insulin resistance worsen outcomes; metformin may be continued in some cases per specialist guidance
- Screen for gestational diabetes early
Mental Health
- Depression and anxiety occur at higher rates in PCOS - screen routinely with PHQ-2 and refer as needed
Summary Table: Management by Goal
| Goal | First-Line | Second-Line / Add-On |
|---|---|---|
| Menstrual regulation | COC | Progestins / LNG-IUD |
| Hirsutism / acne | COC | Spironolactone, flutamide |
| Ovulation induction | Letrozole | Clomiphene ± metformin, gonadotropins |
| Metabolic protection | Lifestyle modification | Metformin, GLP-1 agonists |
| Cardiovascular risk | Lipid profile + lifestyle | Statins per guidelines |
| Endometrial protection | Cyclic progestins / COC | LNG-IUD |
Sources:
- Berek & Novak's Gynecology, Chapter 35 (pp. 1919-1936)
- Harrison's Principles of Internal Medicine 22E, Chapter 405
- Recent evidence: lifestyle interventions (PMID 39861440, 2025), GLP-1 agonists (PMID 39178623, 2024), pregnancy outcomes (PMID 38965226, 2024)
This is a shared conversation. Sign in to Orris to start your own chat.