HAVE LESS TIME TO REVISE. GENERATE MOST HIGH YIELD MCQS FOR BATTERJEE MEDICAL COLLEGE EXAMS JEDDAH I=WITH IMAGES FAST
Reading File
Running Command
cd /home/daytona/workspace/attachments/9b3721c3-3bc6-40ae-9c4f-d282f2923c91 && p…
Searching Images
complement activation pathways classical alternative lectin diagram
Searching Images
innate immunity cells neutrophils macrophages dendritic NK cells
Searching Images
membrane attack complex MAC C5b C6 C7 C8 C9 pore formation
Here are your High-Yield MCQs for Batterjee Medical College — directly mapped to your lecture slides with images. 🎯
🧬 HIGH-YIELD MCQs — INNATE IMMUNITY & COMPLEMENT
Batterjee Medical College | Microbiology Department
📚 LECTURE 1: INNATE IMMUNITY
Q1 — Features of Innate Immunity
Which of the following is a feature of innate immunity that distinguishes it from adaptive immunity?
- A) Produces memory cells after infection
- B) Recognition of specific antigens via B-cell receptors
- C) Responds within minutes to hours without prior exposure ✅
- D) Involves somatic recombination of gene segments
- E) Provides protection only after repeated antigen exposure
Answer: C Innate immunity acts immediately or within minutes to hours. It has no immunological memory and provides the same magnitude of response on repeated exposure — key distinguishing features from adaptive immunity.
Q2 — PAMPs Recognition
Lipopolysaccharide (LPS), peptidoglycan, and double-stranded RNA are examples of:
- A) Danger-associated molecular patterns (DAMPs)
- B) Pathogen-associated molecular patterns (PAMPs) ✅
- C) Antibody epitopes
- D) MHC class II ligands
- E) Acute phase proteins
Answer: B PAMPs are molecular structures found on many microbes, absent from normal human cells, and are essential for microbial survival (making them difficult for microbes to mutate). They are recognized by PRRs of innate immune cells.
Q3 — Pattern Recognition Receptors
A child presents with recurrent severe bacterial, viral, and fungal infections from birth. Genetic testing reveals a mutation affecting pathogen recognition by innate immune cells. Which receptor family is most likely defective?
- A) T-cell receptors (TCRs)
- B) B-cell receptors (BCRs)
- C) Toll-like receptors (TLRs) ✅
- D) MHC class I molecules
- E) Fc receptors
Answer: C TLRs are a major class of Pattern Recognition Receptors (PRRs). Mutations in PRR genes predispose to severe bacterial, viral, and fungal infections. Other PRRs include NLRs, RLRs, and CLRs.
Q4 — Comparison Table: Innate vs. Adaptive
Which statement correctly compares innate and adaptive immunity?
| Feature | Innate | Adaptive |
|---|---|---|
| Receptor diversity | ~1,000 patterns | >10⁷ antigens |
| Receptor encoding | Germline | Somatic recombination |
| Distribution | Nonclonal | Clonal |
A) Innate receptors are encoded by somatic recombination in B cells
B) Adaptive receptors recognize conserved PAMPs shared by many microbes
C) Innate receptors are nonclonal — identical receptors on all cells of same lineage ✅
D) Adaptive immunity provides the immediate first-line response
E) Innate immunity recognizes >10⁷ different antigens
Answer: C Innate receptors are germline-encoded and nonclonal — all cells of the same lineage carry identical receptors. Adaptive immunity uses somatic recombination to create enormous diversity (>10⁷).
Q5 — Mechanical Barriers
A patient with cystic fibrosis suffers from recurrent Pseudomonas aeruginosa respiratory infections. The underlying defect involves:
- A) Absence of tight junctions in epithelium
- B) Deficiency of defensins
- C) Impaired mucociliary escalator due to thick mucus ✅
- D) Loss of HCl secretion in stomach
- E) Decreased commensal bacteria
Answer: C In CF, mucus becomes thick and difficult to move, impairing the mucociliary escalator. This results in retention of bacteria (especially Pseudomonas aeruginosa) and recurrent respiratory infections.
Q6 — Chemical Barriers / Defensins
A 25-year-old woman presents with recurrent skin and mucosal infections. Laboratory testing shows defective antimicrobial peptides produced by neutrophils. Which of the following is most likely deficient?
- A) Interferons
- B) Complement C3
- C) α-Defensins ✅
- D) CRP
- E) IL-8
Answer: C α-defensins are produced by neutrophils and Paneth cells in intestinal crypts. They are highly cationic peptides that create pores in bacterial membranes, killing them. β-defensins are expressed predominantly in epithelial cells.
Q7 — Biological Barriers & Pseudomembranous Colitis
A 60-year-old patient develops severe bloody diarrhea after a prolonged course of broad-spectrum antibiotics. Stool culture grows Clostridium difficile. What is the primary mechanism by which antibiotics predisposed to this infection?
- A) Direct stimulation of C. difficile growth
- B) Destruction of epithelial tight junctions
- C) Suppression of innate immune cytokines
- D) Reduction of commensal bacteria competing with C. difficile ✅
- E) Inhibition of defensin production
Answer: D Commensal microbes protect via competition for nutrients and bacteriocin production. Antibiotics reduce normal flora → overgrowth of C. difficile → pseudomembranous colitis.
Q8 — Acute Phase Response
Which of the following cytokines are the key mediators of the acute phase response?
- A) IL-4, IL-5, IL-13
- B) IL-2, IL-7, IL-15
- C) IL-6, TNF-α, IL-1 ✅
- D) IL-8, IL-12, IFN-γ
- E) IL-10, TGF-β, IL-35
Answer: C IL-6, TNF-α, and IL-1 drive hepatocytes to produce acute phase proteins (APPs) including CRP, serum amyloid A, fibrinogen, haptoglobin, and ferritin.
Q9 — C-Reactive Protein (CRP)
A patient with bacterial pneumonia has a CRP of 180 mg/L (normal <5). Which of the following best describes CRP's mechanism of action?
- A) CRP directly kills bacteria by forming pores in bacterial membranes
- B) CRP binds phosphorylcholine on bacterial cell walls → activates complement + acts as opsonin ✅
- C) CRP stimulates mast cell degranulation
- D) CRP neutralizes viral particles
- E) CRP acts as a chemotactic factor for neutrophils
Answer: B CRP binds phosphorylcholine (a component of bacterial cell wall phospholipids), activates complement, and acts as an opsonin (enhancing phagocytosis). CRP can rise up to 1000-fold during infection.
Q10 — Interleukin-8 (IL-8) — High Yield!
IL-8 is the main chemotactic factor for which cell type?
- A) Lymphocytes
- B) Macrophages
- C) Mast cells
- D) Granulocytes (neutrophils, basophils, eosinophils) ✅
- E) Natural killer cells
Answer: D IL-8 is produced at infection sites by epithelial cells, endothelial cells, smooth muscle cells, and macrophages. It is the main chemotactic factor for granulocytes, recruiting neutrophils to phagocytose bacteria and cellular debris.
Q11 — Interferons
A virus-infected cell produces a protein that diffuses to adjacent cells and induces an antiviral state. This protection is mediated by Protein Kinase R (PKR), which inhibits viral protein synthesis. What protein initiated this response?
- A) IL-6
- B) TNF-α
- C) IFN-γ (gamma interferon)
- D) Alpha/Beta interferons ✅
- E) CRP
Answer: D IFN-α and IFN-β are synthesized early in viral infection, bind to adjacent cells, and induce an antiviral state via:
- PKR → inhibits viral protein synthesis
- 2′,5′-oligoadenylate synthetase → activates RNase → degrades viral RNA IFN-γ has modest antiviral activity but primarily enhances macrophage killing.
Q12 — Cells of Innate Immunity
A patient with a pyogenic abscess. Which cell is responsible for the yellowish-green color of pus and is the most numerous leukocyte in peripheral blood?
- A) Eosinophil
- B) Monocyte
- C) Natural killer cell
- D) Neutrophil ✅
- E) Basophil
Answer: D Neutrophils comprise 60% of peripheral blood leukocytes. Their granules contain myeloperoxidase, which is responsible for the yellowish-green color of pus. They are also called polymorphonuclear (PMN) cells (3–5 nuclear segments).
Q13 — Cells & Their Functions (High Yield Table)
Match: Eosinophils are especially important in:
- A) Antigen presentation to T lymphocytes
- B) Allergic reactions and IgE-mediated responses
- C) Immune responses against parasitic helminth infections ✅
- D) Phagocytosis of intracellular bacteria
- E) Killing virus-infected cells
Answer: C Eosinophil granules contain basic proteins that bind acidic dyes (eosin) and toxic molecules active against helminths and other parasites. Basophils/mast cells handle allergic reactions; NK cells kill virus-infected cells.
Q14 — Natural Killer Cells
NK cells are best characterized as:
- A) Small, agranular lymphocytes that produce antibodies
- B) Cells that require MHC-antigen presentation to kill
- C) Large granular lymphocytes that kill virus-infected and malignantly transformed cells ✅
- D) Phagocytic cells that engulf extracellular bacteria
- E) Cells that present antigens to B lymphocytes
Answer: C NK cells are large granular lymphocytes that kill virus-infected and malignantly transformed cells (tumor cells) without prior sensitization or MHC restriction — a key innate immunity feature.
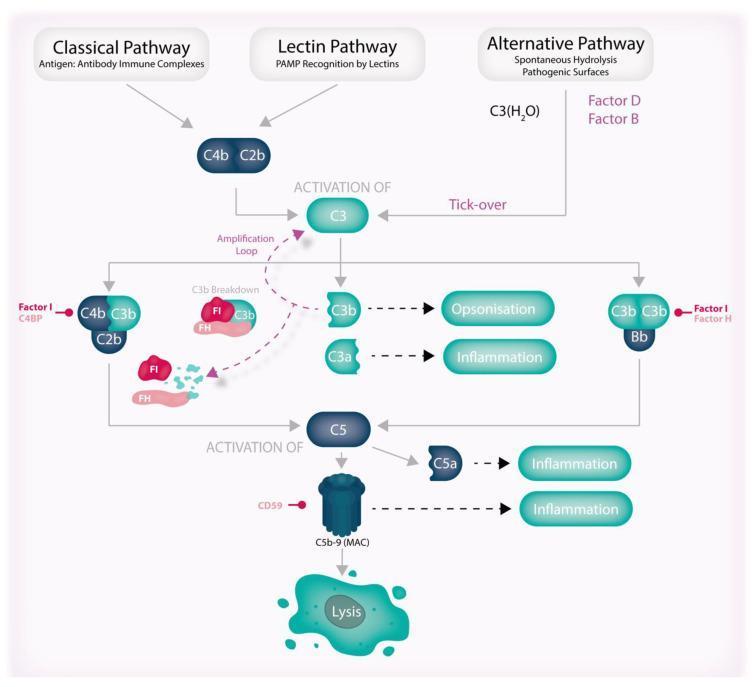
🔬 LECTURE 2: COMPLEMENT ACTIVATION
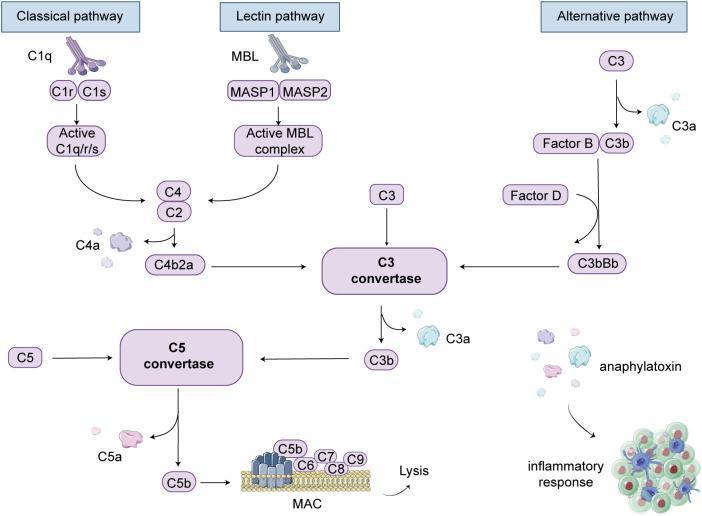
Q15 — Complement Pathways Overview
Which immunoglobulins activate the classical complement pathway?
- A) IgA and IgE
- B) IgD and IgM
- C) IgG and IgM ✅ (mainly IgG1, IgG3)
- D) IgE and IgG4
- E) IgA and IgG
Answer: C The classical pathway requires antibody-antigen complexes — specifically IgG (mainly IgG1 and IgG3) and IgM binding to C1. The alternative pathway is antibody-independent; the lectin pathway uses MBL.
Q16 — Classical Pathway Sequence
In the classical complement pathway, which complex acts as the C3 convertase?
- A) C1q–C1r–C1s
- B) C3bBb
- C) C4b2b (C2b + C4b) ✅
- D) C5b-6-7-8-9
- E) C3bBbP
Answer: C In the classical pathway: C1 is activated → cleaves C4 into C4a + C4b and C2 into C2a + C2b → C4b + C2b form the C3 convertase → cleaves C3 into C3a + C3b. (In the alternative pathway, the C3 convertase is C3bBb.)
Q17 — C3b Functions
A patient's bacteria are coated with C3b. What is the expected effect?
- A) Inhibition of phagocytosis
- B) Direct cytolysis of bacteria
- C) Increased phagocytosis by 1,000-fold (opsonization) ✅
- D) Activation of mast cells and histamine release
- E) Chemotaxis of eosinophils
Answer: C C3b is the key opsonin of the complement system. Phagocytes have C3b receptors on their surface. Opsonization with C3b increases phagocytosis 1,000-fold. C3b can also combine with other proteins to form C5 convertase.
Q18 — Anaphylatoxins (Highest Yield!)
Which complement fragment is the most powerful chemotactic factor for leukocytes AND causes mast cell degranulation?
- A) C3a
- B) C4a
- C) C3b
- D) C5a ✅
- E) C2b
Answer: D C5a is the most powerful chemotactic factor for leukocytes. It also:
- Enhances neutrophil adhesion to endothelium
- Causes mast cell degranulation → histamine release → increased vascular permeability C3a also causes mast cell degranulation but is less potent. Anaphylatoxins = C3a, C4a, C5a.
Q19 — C5 Convertase Formation
In the classical pathway, the C5 convertase is formed when:
- A) C1 binds to IgM
- B) C3b binds to C2b and C4b ✅
- C) Factor B binds C3b
- D) MASP-2 cleaves C4
- E) Properdin stabilizes C3bBb
Answer: B Once enough C3b accumulates on the bacterial surface, C3b binds to C2b + C4b → forms the C5 convertase (C2b+C4b+C3b) → cleaves C5 into C5a + C5b → initiates MAC assembly.
Q20 — Membrane Attack Complex (MAC)
What is the correct sequence of MAC assembly?
- A) C5b → C6 → C7 → C8 → C9(×multiple) ✅
- B) C5a → C6 → C7 → C8 → C9
- C) C3b → C5b → C6 → C7 → C8
- D) C1 → C4 → C2 → C3 → C5b
- E) C9 → C8 → C7 → C6 → C5b
Answer: A MAC assembly: C5b binds C6 → activates C6 to bind C7 → C7 binds C8 → C8 binds multiple C9 molecules → forms a circular pore in the bacterial membrane → cytolysis (cytoplasm rushes out, water rushes in).
Q21 — Alternative Pathway Initiation
How does the alternative complement pathway initiate?
- A) IgG binds to C1q
- B) MBL binds mannose on pathogens
- C) Spontaneous hydrolysis of C3 due to an unstable thioester bond ✅
- D) CRP activates C1
- E) Factor D cleaves C4 and C2
Answer: C C3 contains an unstable thioester bond → undergoes slow spontaneous hydrolysis to C3b → C3b binds to nearby cell surfaces. On foreign cells (but not host cells), this triggers Factor B binding → Factor D cleaves Factor B → forms C3bBb (C3 convertase).
Q22 — Alternative Pathway Stabilization
Which factor stabilizes the C3bBb complex in the alternative pathway?
- A) Factor I
- B) Factor H
- C) C1 inhibitor
- D) Properdin (Factor P) ✅
- E) CD59
Answer: D Properdin (Factor P) binds to the C3bBb complex to stabilize it, forming C3bBbP — the functional C3 convertase of the alternative pathway. This amplification loop allows repeated C3 activation.
Q23 — Lectin Pathway
The lectin (MBL) pathway differs from the classical pathway in that:
- A) It produces C3b but not MAC
- B) It requires IgM to activate C1
- C) It is activated by MBL binding to mannose residues on pathogens (no antibody required) ✅
- D) It uses Factor B and Factor D as its C3 convertase components
- E) It bypasses C4 and C2
Answer: C The lectin pathway is activated by mannose-binding lectin (MBL) or ficolins binding to mannose residues on pathogen surfaces. MASP-2 then cleaves C4 and C2 — same as the classical pathway downstream — but no antibody is required.
Q24 — Complement Regulation: C1 Inhibitor
A 35-year-old woman presents with recurrent episodes of facial swelling, lip edema, difficulty swallowing, and hoarseness — without urticaria. Lab shows low C4 levels. What is the diagnosis and deficient protein?
- A) Paroxysmal nocturnal hemoglobinuria — DAF deficiency
- B) Hereditary angioedema — C1 inhibitor deficiency ✅
- C) C3 deficiency — recurrent pyogenic infections
- D) SLE — immune complex disease
- E) Leukocyte adhesion deficiency — CD18 mutation
Answer: B Hereditary angioedema = C1 inhibitor (C1 INH) deficiency. C1 INH normally inactivates C1r–C1s from C1q. Without it, uncontrolled classical pathway activation → bradykinin overproduction → angioedema (swollen lips/eyes, abdominal cramping, breathing/swallowing difficulty). No urticaria (key differentiator from allergic angioedema).
Q25 — PNH (Complement Regulation)
A 40-year-old man develops dark (cola-colored) urine in the morning, with episodic hemolysis. Lab shows hemoglobinuria and flow cytometry shows absent CD55 (DAF) on red blood cells. What is the mechanism?
- A) IgG autoantibodies against RBC antigens
- B) Deficiency of C3, allowing uncontrolled infection
- C) Loss of decay-accelerating factor → complement-mediated hemolysis ✅
- D) Deficiency of C1 inhibitor → angioedema
- E) MAC formation in large vessels only
Answer: C Paroxysmal Nocturnal Hemoglobinuria (PNH) = acquired deficiency of DAF (CD55) on RBC surfaces. DAF normally displaces C2b from C4b and Bb from C3b (dissociating C3 convertases). Without DAF, complement activates on RBCs → MAC → hemolysis, especially at night (nocturnal, when blood is more acidic).
Q26 — CD59 (Protectin)
Which membrane protein protects host cells from MAC-mediated lysis?
- A) C1 inhibitor
- B) Factor H
- C) Factor I
- D) DAF (CD55)
- E) CD59 (Protectin) ✅
Answer: E CD59 (Protectin) is expressed on many cell types and inhibits MAC formation by preventing the binding of C9 to the C5b-8 complex. It is the terminal complement inhibitor protecting host cells.
Q27 — C3 Deficiency
A 5-year-old child has recurrent sinusitis, pneumonia, and meningitis caused by encapsulated bacteria. Complement studies show markedly reduced C3. What is the expected immunological consequence?
- A) Susceptibility to viral infections only
- B) Failure of the lectin pathway only
- C) Severe, recurrent pyogenic bacterial infections ✅
- D) Susceptibility to Neisseria species only
- E) Inability to form IgG antibodies
Answer: C C3 deficiency leads to severe, recurrent pyogenic bacterial infections (e.g., sinusitis, RTIs, meningitis). C3 is the central molecule — its deficiency impairs ALL three complement pathways, opsonization, and MAC formation.
Q28 — C5–C9 Deficiency (Terminal Complement)
Deficiency of C5–C9 specifically predisposes to infection with which organism?
- A) Staphylococcus aureus
- B) Streptococcus pneumoniae
- C) Neisseria species (N. meningitidis, N. gonorrhoeae) ✅
- D) Pseudomonas aeruginosa
- E) Candida albicans
Answer: C Terminal complement deficiency (C5–C9) = inability to form MAC → greatly enhanced susceptibility to Neisseria species. Neisseria (gram-negative diplococci with thin cell walls) rely on MAC for killing. Encapsulated bacteria are better handled by opsonization (C3b).
Q29 — Immune Complex Diseases
A patient with SLE (systemic lupus erythematosus) has low serum C3 and C4 levels. Why?
- A) The liver is destroyed and cannot synthesize complement
- B) Immune complexes bind and consume complement ✅
- C) Autoantibodies directly cleave complement proteins
- D) SLE causes C1 inhibitor deficiency
- E) The alternative pathway is constitutively overactivated
Answer: B In immune complex diseases (SLE, acute glomerulonephritis), immune complexes bind and activate complement, consuming complement proteins → low C3 and C4 levels. This is useful diagnostically — low complement levels + immune complex disease.
Q30 — Clinical Case (From Lecture Slide!)
A 40-year-old man presents to the emergency department with swelling involving the lips and lower part of the face, difficulty swallowing, and hoarseness of voice.
Which is the most likely explanation for the edema?
- A) Decrease in factor C3b
- B) Decrease in C1 inhibitor ✅
- C) Decrease in C5a
- D) Decrease in factor B
- E) Decrease in properdin
Answer: B This is the classic presentation of hereditary angioedema — facial/lip swelling + airway compromise. Caused by C1 inhibitor deficiency → uncontrolled complement activation → bradykinin accumulation → angioedema. This question is directly from your lecture slide!
🧪 BONUS RAPID-FIRE SUMMARY TABLE
| Complement Fragment | Key Function |
|---|---|
| C3b | Opsonin (↑phagocytosis 1000×) |
| C3a | Anaphylatoxin (mast cell degranulation) |
| C5a | Most potent chemotaxin + anaphylatoxin |
| C5b-9 | Membrane Attack Complex (MAC) → lysis |
| C4b2b | Classical C3 convertase |
| C3bBb | Alternative C3 convertase |
| C3bBbP | Alternative C3 convertase (stabilized by Properdin) |
| Deficiency | Consequence |
|---|---|
| C3 | Severe pyogenic bacterial infections |
| C5–C9 | Neisseria susceptibility |
| C1 INH | Hereditary angioedema |
| DAF (CD55) | PNH (hemolysis) |
| CD59 | MAC-mediated lysis of host cells |
30 MCQs total — all directly mapped to your L1 and L2 lecture slides. Focus especially on Q15–Q30 for complement (highest exam density) and Q5, Q10, Q11 for innate immunity traps. Good luck! 💪
This is a shared conversation. Sign in to Orris to start your own chat.