Write a complete note on apml causes differntial lab management and latest trial and all landmark trial like the world best hematologist
"acute promyelocytic leukemia" AND treatment
APL acute promyelocytic leukemia landmark trials ATRA ATO AIDA 2025 guidelines
"acute promyelocytic leukemia" AND "arsenic trioxide" AND "ATRA"
PMID: 23841729
PMID: 27400939
PMID: 40825164
PMID: 38554737
PMID: 41906112
https://www.nature.com/articles/s41408-021-00514-3
Acute Promyelocytic Leukemia (APL / AML-M3) - Complete Clinical Note
1. DEFINITION AND OVERVIEW
- Harrison's Principles of Internal Medicine, 22E (2025), p.877
- Henry's Clinical Diagnosis and Management by Laboratory Methods
2. ETIOLOGY AND PATHOGENESIS
2.1 Molecular Basis
- Blocks normal retinoic acid receptor signaling
- Recruits nuclear co-repressors (NCoR, SMRT, HDAC complexes) causing transcriptional repression of myeloid differentiation genes
- Arrests maturation at the promyelocyte stage
- Promotes self-renewal of malignant promyelocytes
- Prevents apoptosis via aberrant epigenetic silencing
2.2 Variant Translocations (Rare, ~1-2%)
| Translocation | Fusion Gene | Response to ATRA |
|---|---|---|
| t(11;17)(q23;q12) | PLZF-RARA | Resistant to ATRA |
| t(5;17)(q35;q12) | NPM1-RARA | Partially sensitive |
| t(11;17)(q13;q12) | NuMA-RARA | Sensitive |
| t(17;17)(q11;q12) | STAT5b-RARA | Resistant |
Clinically critical: PLZF-RARA variants are ATRA-resistant and must be identified early.
2.3 Risk Classification (Sanz Score - PETHEMA)
| Risk Group | WBC at Diagnosis | Platelet Count |
|---|---|---|
| Low | ≤10 × 10⁹/L | >40 × 10⁹/L |
| Intermediate | ≤10 × 10⁹/L | ≤40 × 10⁹/L |
| High | >10 × 10⁹/L | Any |
- Standard-risk: WBC ≤10,000/μL
- High-risk: WBC >10,000/μL
3. CLINICAL FEATURES
3.1 Presenting Symptoms
- Bleeding diathesis (most distinctive): ecchymoses, petechiae, gingival bleeding, menorrhagia, epistaxis, CNS hemorrhage
- Fatigue, pallor (anemia)
- Fever (infection or leukemic fever)
- Bone pain
- Hepatosplenomegaly (less common than other AMLs)
- Notably absent: lymphadenopathy is rare
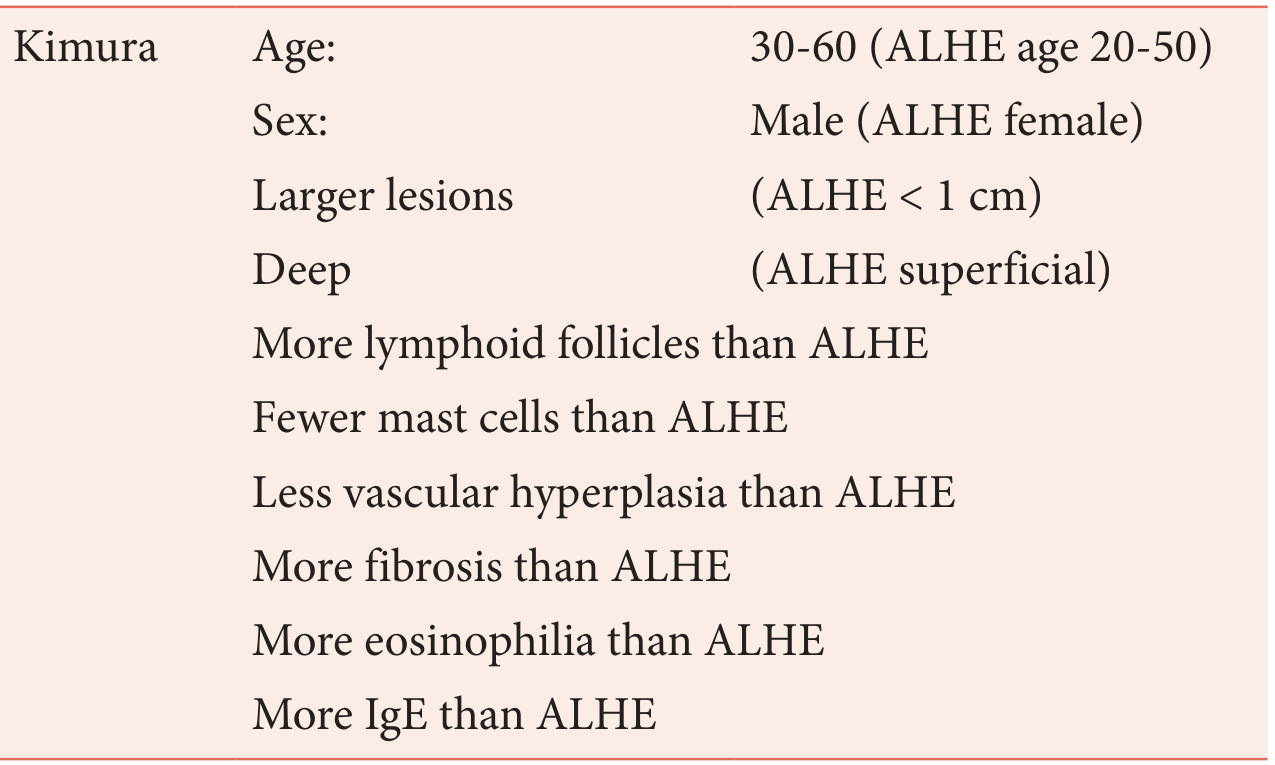
3.2 Morphologic Subtypes
| Subtype | Frequency | Features |
|---|---|---|
| Hypergranular (typical) | ~75% | Large, densely granulated promyelocytes; Auer rods (often "faggot cells" with bundles of Auer rods); HLA-DR negative |
| Microgranular (M3v) | ~25% | Bilobed/monocytoid nuclei; few/invisible granules on light microscopy; high WBC; quickly fatal if unrecognized |
The microgranular variant is a trap - morphology can be mistaken for monocytic leukemia but granules are abundant on electron microscopy. FISH/PCR is mandatory.
4. DIFFERENTIAL DIAGNOSIS
| Diagnosis | Distinguishing Features |
|---|---|
| AML-M4 (myelomonocytic) | Mixed myeloid + monocytic differentiation; no PML-RARA; no Auer rod faggots; HLA-DR positive |
| AML-M2 | Maturation to myelocyte stage; t(8;21); no DIC coagulopathy profile |
| AML-M5 (monocytic) | CD14+, CD64+; no PML-RARA; gum infiltration more common |
| Microgranular APL vs. AML-M5 | Critical distinction: FISH/PCR for PML-RARA; electron microscopy shows abundant granules in M3v |
| Reactive promyelocytosis | Seen in G-CSF treatment, drug reactions; normal karyotype; resolves with cause removal |
| CML blast crisis (myeloid) | Philadelphia chromosome t(9;22); BCR-ABL1; prior CML history; DIC uncommon |
| APML-like coagulopathy in other AMLs | AML with complex karyotype can mimic DIC; lacks PML-RARA |
5. LABORATORY DIAGNOSIS
5.1 Complete Blood Count
| Parameter | Typical Finding |
|---|---|
| WBC | Variable (low in hypergranular, very high in M3v) |
| Hemoglobin | Low (usually <10 g/dL) |
| Platelets | Markedly low (often <50 × 10⁹/L) |
| Blasts/Promyelocytes | >20% (often >80%) in marrow |
5.2 Coagulation Profile (Critical in APL)
| Test | Finding in APL |
|---|---|
| PT/INR | Prolonged |
| aPTT | Prolonged |
| Fibrinogen | Markedly low (<100 mg/dL is critical threshold) |
| D-dimer | Markedly elevated |
| FDP (fibrin degradation products) | Elevated |
| Thrombin time | Prolonged |
| Platelet count | Low |
| Blood film | Schistocytes (microangiopathy) |
Mechanism: Promyelocyte granules contain tissue factor, cancer procoagulant, and annexin II (promotes plasminogen → plasmin conversion), driving simultaneous DIC + hyperfibrinolysis.
5.3 Bone Marrow Examination
- Aspirate: >20% hypergranular promyelocytes; Auer rods/faggots; marrow usually hypercellular
- Biopsy: Not always required if aspirate diagnostic
- Cytochemistry: MPO strongly positive; NSE negative (unlike monocytic)
5.4 Immunophenotype (Flow Cytometry)
| Marker | APL |
|---|---|
| CD13, CD33 | Positive |
| CD34 | Usually negative |
| HLA-DR | Negative (key distinguishing feature) |
| CD117 | Variable |
| CD56 | Expressed in ~25% (adverse prognosis) |
| CD11b, CD14, CD64 | Negative |
HLA-DR negativity with CD34 negativity and strong CD13/33 in a bleeding patient = start ATRA NOW.
5.5 Cytogenetics and Molecular
| Test | Finding |
|---|---|
| Conventional karyotype | t(15;17)(q22;q12) - seen in ~95% |
| FISH for PML-RARA | Most rapid (result in 24-48 hours) - GOLD STANDARD for urgent diagnosis |
| RT-PCR for PML-RARA | Confirms diagnosis AND determines isoform (bcr1/long, bcr2/variable, bcr3/short) |
| NGS | Not first-line; used for variant translocations |
RT-PCR isoform matters: bcr3 (short) correlates with higher WBC and microgranular variant. Also critical for MRD monitoring.
5.6 Chemistry Panel
- LDH: elevated (tumor burden)
- Uric acid: elevated
- Creatinine: check baseline (ATO nephrotoxic)
- Electrolytes: check K, Mg (QTc risk with ATO)
- LFTs: baseline (both ATRA and ATO can be hepatotoxic)
- ECG: baseline QTc before starting ATO (prolongation is contraindication to ATO)
6. MANAGEMENT
6.1 EMERGENCY MANAGEMENT (Before Genetics Are Confirmed)
- ATRA 45 mg/m²/day orally in two divided doses
- Aggressive transfusion support:
- Platelets: keep >50 × 10⁹/L (>30 × 10⁹/L minimum)
- Cryoprecipitate/FFP: keep fibrinogen >150 mg/dL (>100 mg/dL minimum)
- Correct coagulopathy aggressively - hemorrhagic death kills before therapy works
- AVOID heparin (worsens hemorrhage)
- AVOID lumbar puncture until coagulopathy corrected
6.2 INDUCTION THERAPY
Standard-Risk APL (WBC ≤10,000/μL) - CURRENT STANDARD OF CARE
| Drug | Dose | Route | Duration |
|---|---|---|---|
| ATRA | 45 mg/m²/day in 2 divided doses | Oral | Until morphologic CR |
| ATO | 0.15 mg/kg/day | IV | Until morphologic CR (usually day 25-35) |
High-Risk APL (WBC >10,000/μL)
- ATRA 45 mg/m² + ATO 0.15 mg/kg/day + idarubicin 12 mg/m² IV on days 1 and 3
- Followed by 4 cycles of ATRA-ATO consolidation (no further anthracycline)
- ATRA 45 mg/m²/day + idarubicin 12 mg/m² IV on days 2, 4, 6, 8
- Followed by anthracycline-based consolidation + 2 years ATRA maintenance
The 2025 APOLLO Trial (Platzbecker et al., JCO 2025, PMID 40825164) demonstrated 2-year EFS of 88% with ATRA-ATO + minimal idarubicin vs. 71% with ATRA-CHT (AIDA) in high-risk APL, supporting ATRA-ATO extension to high-risk disease.
If Contraindications to ATO
- Prolonged QTc (>500 ms after correction)
- Severe hepatic impairment
- Uncontrolled electrolyte abnormalities
6.3 DIFFERENTIATION SYNDROME (DS) - MANAGEMENT
- Mild DS: Start dexamethasone 10 mg IV every 12 hours
- Moderate/severe DS: Dexamethasone + temporary hold of ATRA and/or ATO
- Continue dexamethasone until symptoms resolve (minimum 3 days)
- Cytoreduction with hydroxyurea if WBC rising rapidly
6.4 CONSOLIDATION THERAPY
- 4 consolidation cycles (each cycle = 4 weeks on/4 weeks off)
- ATRA 45 mg/m²/day × 2 weeks every 4 weeks for 7 cycles total
- ATO 0.15 mg/kg/day × 5 days/week × 4 weeks per cycle (4 cycles total)
- 4 cycles of ATRA + ATO (0.15 mg/kg/day × 5 days/week × 4 weeks per cycle)
- No additional anthracycline consolidation needed
6.5 MOLECULAR REMISSION MONITORING (MRD)
| Timing | Action |
|---|---|
| After consolidation cycle 2 | First PCR check |
| After final consolidation | Must be PCR negative - if positive → molecular relapse protocol |
| Every 3 months × 2 years | Surveillance in high-risk patients |
- Persistent/rising PCR after consolidation = relapse signal → act before hematologic relapse
- Sensitivity of PCR: 10⁻⁴ to 10⁻⁵ (one leukemic cell per 10,000-100,000 normal cells)
7. RELAPSED APL
7.1 Salvage with ATO
7.2 Gemtuzumab Ozogamicin (GO)
- Anti-CD33 antibody-drug conjugate
- Used in combination or alone in relapsed APL
- Achieves molecular CR in patients who have received both ATRA and ATO
- Particularly valuable as bridge to transplant
7.3 Transplantation in Relapsed APL
| Modality | EFS | OS | NRM |
|---|---|---|---|
| Auto-HCT | ~71% | ~82% | ~5% |
| Allo-HCT | ~54% | ~58% | ~29% |
- PCR-positive at time of transplant (GVL benefit needed)
- Third or later relapse
- High-risk features not achieving molecular CR
8. LANDMARK CLINICAL TRIALS - CHRONOLOGICAL
Era 1: Discovery of ATRA (1987-1997)
- First clinical use of ATRA in 24 APL patients - CR rate 96%
- Revolutionized APL from a fatal to a curable disease
- Established that pharmacologic doses of ATRA cause terminal differentiation of leukemic promyelocytes
- Randomized ATRA → chemotherapy vs. concurrent ATRA + chemotherapy vs. chemotherapy alone
- Established ATRA + chemotherapy as standard of care
- 2-year DFS: ATRA → chemo 62%, concurrent 79%, chemo 50%
- ATRA + idarubicin (without cytarabine) as induction
- CR ~95%, OS at 5 years ~75-80%
- Established AIDA as the gold standard chemotherapy-based regimen for APL
Era 2: Arsenic Trioxide (1996-2010)
- First systematic clinical trial of ATO in relapsed APL
- CR rate ~85% with ATO monotherapy in relapsed/refractory APL
- Launched the ATO revolution
- ATO + ATRA pilot studies demonstrated synergistic efficacy
- ATRA + ATO ± gemtuzumab in newly diagnosed APL, all risk groups
- CR 92%, 3-year OS 85% - first suggestion that chemotherapy could be eliminated
Era 3: Chemotherapy-Free Regimens (2013-2017) - PARADIGM SHIFT
- Phase III RCT: ATRA + ATO vs. ATRA + idarubicin-chemotherapy in low/intermediate-risk APL (WBC ≤10 × 10⁹/L)
- n = 156 patients (80 ATRA-ATO, 79 ATRA-CHT)
- CR: 100% ATRA-ATO vs. 95% ATRA-CHT (P=0.12)
- 2-year EFS: 97% vs. 86% (P=0.02 for superiority of ATRA-ATO)
- OS at 2 years: 99% vs. 91% (P=0.02)
- Less hematologic toxicity, fewer infections with ATRA-ATO
- Established ATRA + ATO as the new standard of care for non-high-risk APL
- Confirmed and extended: 50-month EFS 97.3% vs. 80% (P<0.001)
- CIR: 1.9% vs. 13.9% (P=0.0013)
- OS: 99.2% vs. 92.6% (P=0.0073)
- No maintenance needed in ATRA-ATO arm
- Two therapy-related myeloid neoplasms in ATRA-CHT arm - NONE in ATRA-ATO arm
- UK AML Working Party Phase III RCT: ATRA + ATO vs. ATRA + chemotherapy (with/without GO)
- n = 235 patients (non-high-risk)
- 2-year OS: 93% ATRA-ATO vs. 89% ATRA-chemo
- Lower relapse rate, less toxicity with ATRA-ATO
- Confirmed ATRA-ATO superiority across different ATO dosing schedule
- Pediatric APL: confirmed ATRA + ATO effective and safer than ATRA-chemo in children
- Updated in AAML1331 (Kutny et al., JAMA Oncol 2022, PMID 34762093): ATO + ATRA equivalent to ATRA-chemo in pediatric APL
Era 4: Extending ATRA-ATO to High-Risk and Novel Approaches (2020-Present)
- Phase III RCT: ATRA + ATO + low-dose idarubicin (days 1,3) vs. ATRA-AIDA in high-risk APL (WBC >10,000/μL)
- n = 133 patients (68 ATRA-ATO, 65 ATRA-CHT)
- Primary endpoint: 2-year EFS: 88% ATRA-ATO vs. 71% ATRA-CHT (HR 0.4, P=0.02)
- Molecular relapse: 1.5% vs. 12.3% (P=0.014)
- Serious adverse events: 32% ATRA-ATO vs. 68% ATRA-CHT (P<0.01)
- Conclusion: ATRA + ATO + minimal idarubicin is now supported for high-risk APL - extends the ATRA-ATO paradigm to all risk groups
- Academic community partnership study addressing early mortality in APL
- Focused on real-world implementation of early ATRA initiation to reduce hemorrhagic death
- Systematic review and meta-analysis of 12 studies (GRADE framework)
- ATRA + ATO vs. ATRA + chemotherapy:
- CR: RR 1.04 (95% CI 1.02-1.06)
- DFS: RR 1.22 (95% CI 1.11-1.34)
- EFS: RR 1.25 (95% CI 1.20-1.29)
- OS: RR 1.07 (95% CI 1.03-1.12)
- QTc prolongation higher with ATRA-ATO: RR 3.79 (P=0.05) - mandates cardiac monitoring
- Definitively confirms ATRA + ATO superiority across all outcomes
9. ORAL ATO - EMERGING DATA
- Phase III pediatric RCT (Huang et al., Blood Cancer J 2023, PMID 38052803): oral vs. IV ATO in children - equivalent efficacy and safety
- Significant pharmacoeconomic and logistic advantages (outpatient consolidation)
- Currently used widely in Asia; regulatory approval pending in Western countries
10. SPECIAL POPULATIONS
Pregnancy
- ATRA is teratogenic (Category X) in first trimester
- ATO is teratogenic and embryotoxic
- Manage with ATO alone in second/third trimester if possible, or deliver early
- Multidisciplinary approach mandatory
Elderly (>70 years)
- ATRA + ATO preferred (avoid anthracyclines)
- Full dose ATRA-ATO achievable with careful supportive care
- Dose reduction of ATO may be needed if QTc or renal issues
CNS Relapse
- CNS APL is rare (2-3%) but serious
- Managed with intrathecal cytarabine + MTX
- ATO penetrates CNS poorly - systemic therapy + IT chemotherapy needed
11. MONITORING AND TOXICITY MANAGEMENT
ATRA Toxicities
| Toxicity | Frequency | Management |
|---|---|---|
| Differentiation syndrome | 10-30% | Dexamethasone 10 mg Q12h; hold ATRA if severe |
| Pseudotumor cerebri (headache) | ~15% | Acetazolamide, analgesics; dose reduction |
| Hypertriglyceridemia | Common | Dietary modification; statin if severe |
| Hepatotoxicity (LFT elevation) | 20-30% | Monitor LFTs; dose reduction if >5× ULN |
| Skin dryness, cheilitis | Common | Moisturizers; symptomatic |
ATO Toxicities
| Toxicity | Frequency | Management |
|---|---|---|
| QTc prolongation | 30-40% | Baseline ECG; correct K⁺/Mg²⁺; hold if QTc >500 ms |
| Hepatotoxicity | 30-50% | Monitor LFTs weekly |
| Peripheral neuropathy | 5-10% | Dose reduction; B vitamins |
| Fatigue, leukocytosis | Common | Hydroxyurea for WBC control |
| Differentiation syndrome | <15% | Dexamethasone |
| APL hyperleukocytosis | ~25% high-risk | Hydroxyurea/dexamethasone; cytoreduction |
12. PROGNOSIS
| Risk Group | CR Rate | 5-Year OS (ATRA-ATO era) |
|---|---|---|
| Standard-risk (ATRA-ATO) | ~100% | ~95% |
| High-risk (ATRA-ATO + low IDA) | ~95% | ~85-90% |
| Relapsed APL (ATO-based salvage) | ~70-85% | ~60-70% (with HCT) |
- WBC >10,000/μL at diagnosis
- CD56 expression (poor prognosis)
- FLT3-ITD mutation (associated with microgranular variant, high WBC)
- Secondary APL (therapy-related)
- Advanced age
- High LDH
13. SUMMARY OF CURRENT TREATMENT ALGORITHM (2026)
APL Suspected (bleeding + promyelocytes + morphology)
↓
IMMEDIATE ATRA 45 mg/m²/d + aggressive coagulopathy support
(Do NOT wait for FISH/PCR)
↓
FISH/PCR confirms PML-RARA
↓
Risk stratify
/ \
Standard-risk High-risk (WBC >10,000)
(WBC ≤10,000) ↓
↓ ATRA + ATO + idarubicin (days 1,3) [APOLLO]
ATRA + ATO OR ATRA + AIDA (if ATO contraindicated)
(chemotherapy- ↓
free; APL0406) Cytoreduction with hydroxyurea + dexamethasone
↓ Watch for differentiation syndrome
Consolidation ↓
4 cycles Consolidation
ATRA + ATO 4 cycles ATRA + ATO
↓ ↓
PCR monitoring q3mo × 2 years
↓
PCR negative: CURE (no maintenance needed)
PCR positive: Salvage with ATO ± GO → Auto-HCT if molecular CR achieved
REFERENCES
- Harrison's Principles of Internal Medicine 22E (2025), p.877 - Treatment of APL
- Henry's Clinical Diagnosis and Management by Laboratory Methods - APL with PML-RARA
- Goldman-Cecil Medicine - Table 168-3: Management of Newly Diagnosed APL
- Lo-Coco F et al. NEJM 2013 - APL0406 initial results; ATRA+ATO vs ATRA+CHT, PMID 23841729
- Platzbecker U et al. JCO 2017 - APL0406 final results at 50 months, PMID 27400939
- Platzbecker U et al. JCO 2025 - APOLLO Trial: ATRA-ATO in high-risk APL, PMID 40825164
- Ahmad H et al. BMC Cancer 2026 - GRADE meta-analysis ATRA+ATO vs ATRA+CHT, PMID 41906112
- Mohty R et al. Transplant Cell Ther 2024 - HCT in relapsed APL meta-analysis, PMID 38554737
- Yilmaz M et al. Blood Cancer J 2021 - Current APL treatment algorithms, PMID 34193815
- Huang DP et al. Blood Cancer J 2023 - Oral vs IV ATO in pediatric APL, PMID 38052803
- NCCN Guidelines AML v3.2026 (November 2025)
Complete APL Note - Summary Card
| Domain | Key Points |
|---|---|
| Genetics | t(15;17) → PML-RARA; PLZF-RARA = ATRA resistant |
| Hallmark lab | DIC + hyperfibrinolysis; HLA-DR negative; Auer rod faggots |
| Diagnosis | FISH (fast) + RT-PCR (isoform + MRD); start ATRA before results |
| Standard risk Rx | ATRA + ATO - chemotherapy-free; CR ~100%; OS ~95% |
| High risk Rx | ATRA + ATO + low-dose idarubicin (APOLLO 2025) |
| Differentiation syndrome | Dexamethasone 10 mg Q12h; hold ATRA/ATO if severe |
| MRD monitoring | PCR PML-RARA after consolidation; q3mo × 2 years |
| Relapse | ATO salvage → molecular CR → Auto-HCT |
| Paradigm-shifting trial | APL0406 (Lo-Coco, NEJM 2013) - proved ATRA+ATO superior to ATRA+chemo |
| Newest trial | APOLLO (Platzbecker, JCO 2025) - extends ATRA-ATO to high-risk APL |
Management of apml low and high risk like world best hematologist with trials if present landmark and latest
"acute promyelocytic leukemia" AND "high risk" AND "arsenic trioxide"
APL management 2025 low risk high risk ATRA ATO APOLLO trial NCCN guidelines standard of care
PMID: 36404343
PMID: 40825164
"acute promyelocytic leukemia" AND relapse AND "gemtuzumab" AND "arsenic"
PMID: 41029961
PMID: 38431521
https://www.albertahealthservices.ca/assets/info/hp/cancer/i…
APL Management - Low Risk & High Risk
A Complete Expert Hematology Reference (2026)
STEP 0 - BEFORE ANYTHING ELSE: THE EMERGENCY RULE
Start ATRA the moment you suspect APL. Do not wait for FISH, PCR, or karyotype.
- ATRA 45 mg/m²/day orally in 2 divided doses - START NOW
- Platelet transfusion: maintain >50 × 10⁹/L (or >30 at minimum)
- Cryoprecipitate/FFP: maintain fibrinogen >150 mg/dL
- Check and correct K⁺ and Mg²⁺ (QTc risk with ATO)
- Baseline ECG (QTc before starting ATO)
- Baseline LFTs, creatinine
- Send FISH + RT-PCR for PML-RARA urgently
- No heparin. No LP until coagulopathy resolved.
RISK STRATIFICATION
| Risk Group | WBC (×10⁹/L) | Platelets (×10⁹/L) |
|---|---|---|
| Low | ≤10 | >40 |
| Intermediate | ≤10 | ≤40 |
| High | >10 | Any |
- NCCN (2026) simplifies: Standard-risk = WBC ≤10,000/μL / High-risk = WBC >10,000/μL
- Low + intermediate = "non-high-risk" = treated identically (ATRA-ATO, no chemotherapy)
PART A: STANDARD-RISK APL (WBC ≤10,000/μL)
~70-75% of newly diagnosed APL patients
A1. INDUCTION - THE LO-COCO / APL0406 REGIMEN
| Drug | Dose | Route | Duration |
|---|---|---|---|
| ATRA | 45 mg/m²/day in 2 divided doses | Oral | Until hematologic CR (max 60 days) |
| ATO | 0.15 mg/kg/day (capped at 10 mg/day) | IV over 2 hours | Until hematologic CR (max 60 days) |
| Prednisone | 0.5 mg/kg/day | Oral | Day 1 until end of induction (DS prophylaxis) |
- Bone marrow aspirate at hematologic recovery (platelets >100 × 10⁹/L, ANC >1 × 10⁹/L, typically day 28-42)
- Confirm morphologic CR (blasts <5%, no Auer rods)
- Molecular CR by PCR is NOT required after induction - aim for this after consolidation
A2. CONSOLIDATION - 4 CYCLES (No chemotherapy)
- ATO 0.15 mg/kg/day × 5 days/week for 4 consecutive weeks
- ATRA 45 mg/m²/day days 1-28 (or 2-week pulses per modified schedule)
- ATO 0.15 mg/kg/day × 5 days/week × 4 weeks
- ATRA 45 mg/m²/day × 2 weeks on / 2 weeks off within each cycle
- ATRA 45 mg/m²/day: Days 1-28
- ATO 0.15 mg/kg/day: Days 1-28
- ATRA 45 mg/m²/day: Days 1-7, 15-21, 29-35
- ATO 0.15 mg/kg/day: Days 1-5, 8-12, 15-19, 22-26, 29-33
A3. MAINTENANCE
- APL0406 trial: no maintenance in ATRA-ATO arm; 50-month CIR only 1.9%
- AML17 trial: no maintenance in ATRA-ATO arm; outcomes superior to ATRA-chemo with maintenance
- This is a definitive paradigm shift - spare patients 2 years of maintenance toxicity
Exception: If patient was treated with ATRA-chemotherapy (AIDA) due to ATO contraindication, give maintenance: ATRA 45 mg/m²/day × 15 days every 3 months + 6-mercaptopurine 50-90 mg/m²/day + methotrexate 5-15 mg/m² weekly for 2 years.
A4. MRD MONITORING AFTER CONSOLIDATION
| Timepoint | Test | Action |
|---|---|---|
| After consolidation cycle 2 | RT-PCR PML-RARA (bone marrow) | If positive → continue consolidation |
| After final consolidation (cycle 4) | RT-PCR PML-RARA (bone marrow) | Must be PCR negative. If positive = molecular relapse protocol |
| Every 3 months × 2 years (surveillance) | RT-PCR PML-RARA (peripheral blood acceptable) | Rising signal = early relapse intervention |
PCR sensitivity: 10⁻⁴ to 10⁻⁵. A rising/persistent PCR after consolidation = treat before hematologic relapse.
A5. EXPECTED OUTCOMES - STANDARD RISK (ATRA-ATO)
| Outcome | Result |
|---|---|
| CR rate | ~100% |
| 2-year EFS | 97% |
| 50-month OS | ~99% |
| Cumulative incidence of relapse (50 months) | 1.9% |
| Therapy-related myeloid neoplasm | Zero (vs. 2 cases in chemo arm) |
PART B: HIGH-RISK APL (WBC >10,000/μL)
~25-30% of newly diagnosed APL patients - the clinical challenge
WHY HIGH-RISK IS DIFFERENT
- ATRA alone causes massive hyperleukocytosis (WBC can shoot to >50 × 10⁹/L within days) → fatal DS
- Higher rate of differentiation syndrome with ATRA
- More severe coagulopathy → higher early death rate (hemorrhagic)
- FLT3-ITD mutations more common (especially in microgranular M3v variant)
- Historically: 5-year RFS with ATRA-chemotherapy (AIDA) ~70-75% vs. ~90% for standard risk
- Hydroxyurea 0.5-1g every 6-8 hours to bring WBC down rapidly
- Dexamethasone 10 mg IV every 12 hours from Day 1 (DS prophylaxis when WBC >10,000)
- ATRA - begin simultaneously
B1. INDUCTION - HIGH-RISK APL
Option 1 (CURRENT PREFERRED): APOLLO Protocol - 2025
| Drug | Dose | Route | Day |
|---|---|---|---|
| ATRA | 45 mg/m²/day in 2 divided doses | Oral | Day 1 → until CR (max 60 days) |
| ATO | 0.15 mg/kg/day | IV over 2 hrs | Day 1 → until CR (max 60 days) |
| Idarubicin | 12 mg/m² | IV | Days 1 and 3 only (just 2 doses) |
| Hydroxyurea | 0.5-1g Q6-8h | Oral | Titrate to WBC; stop when WBC <10 × 10⁹/L |
| Dexamethasone | 10 mg Q12h | IV/Oral | Days 1-14 (DS prophylaxis) |
Option 2 (APML4 Protocol - Australian, still used):
| Drug | Dose | Day |
|---|---|---|
| ATRA | 45 mg/m²/day | Day 1 → until CR |
| ATO | 0.15 mg/kg/day IV | Day 1 → until CR |
| Idarubicin | 12 mg/m² IV | Days 2, 4, 6, 8 (4 doses) |
Option 3 (Classic AIDA - if ATO contraindicated):
| Drug | Dose | Day |
|---|---|---|
| ATRA | 45 mg/m²/day | Day 1 → until CR |
| Idarubicin | 12 mg/m² IV | Days 2, 4, 6, 8 |
- Replace with AIDA
- Alternative: ATRA + daunorubicin + cytarabine (AML-like induction)
- Alternative in cardiac risk: ATRA + gemtuzumab ozogamicin (GO) ± ATO
Option 4 (NCCN 2026 - specific contraindication scenarios):
| Scenario | Recommended Induction |
|---|---|
| High-risk, no cardiac contraindication | ATRA + ATO + idarubicin (APOLLO or APML4) |
| Low ejection fraction (EF <50%) | ATRA + ATO + gemtuzumab ozogamicin (GO) |
| QTc prolongation (>500 ms, uncorrectable) | ATRA + GO, or ATRA + daunorubicin + cytarabine |
B2. END-OF-INDUCTION ASSESSMENT (HIGH-RISK)
- Bone marrow aspirate + biopsy at day 28 (or at count recovery)
- Confirm morphologic CR
- Consider LP (lumbar puncture) before consolidation - NCCN recommends this for high-risk patients (CNS APL rare but >2-3% in high-risk)
- PCR PML-RARA from marrow at end of induction
B3. CONSOLIDATION - HIGH-RISK APL
After APOLLO Protocol Induction:
| Cycle | ATO | ATRA |
|---|---|---|
| 1-4 | 0.15 mg/kg/day × 5 days/week × 4 weeks (then 4 weeks off) | 45 mg/m²/day × 2 weeks on / 2 weeks off per cycle |
After APML4 Induction:
- Consolidation 1: ATRA (days 1-15) + ATO 0.15 mg/kg/day (days 1-28)
- Consolidation 2: ATRA (days 1-15) + ATO (days 1-28)
- Then: Maintenance × 2 years (ATRA + 6-MP + MTX)
After AIDA Induction (chemotherapy-based):
| Consolidation Cycle | Drugs |
|---|---|
| C1 | ATRA 45 mg/m²/day × 15 days + idarubicin 5 mg/m²/day × 4 days |
| C2 | ATRA 45 mg/m²/day × 15 days + mitoxantrone 10 mg/m² × 3 days |
| C3 | ATRA 45 mg/m²/day × 15 days + idarubicin 12 mg/m² × 1 day |
| Maintenance | ATRA + 6-MP + MTX × 2 years |
B4. MAINTENANCE - HIGH-RISK (DEBATED)
- In the ATO era with APOLLO-type regimens: maintenance not routinely needed (molecular relapse <2% at 2 years)
- In AIDA-based regimens: 2 years maintenance is standard
- In APL15 trial and APML4: maintenance ATRA + 6-MP + MTX included for high-risk
Expert opinion (Chin & Tallman, Curr Opin Oncol 2025, PMID 41029961): The need for maintenance in high-risk patients treated with ATRA-ATO regimens remains under study. Current practice leans toward no maintenance after APOLLO-type regimens given very low relapse rates.
B5. EXPECTED OUTCOMES - HIGH-RISK APL
| Trial/Regimen | 2-year EFS | OS | Relapse |
|---|---|---|---|
| APOLLO (ATRA-ATO + 2-dose IDA) | 88% | Numerically superior | 1.6% |
| AIDA/ATRA-CHT (historical control in APOLLO) | 71% | Lower | 14% |
| APML4 (ATRA+ATO+IDA × 4) | ~85% | ~90% at 2 yr | ~5% |
| APL15 (ATRA-ATO alone, no chemo) | 85% | ~95% | ~5% |
PART C: MANAGEMENT OF DIFFERENTIATION SYNDROME (DS)
- Fever (unexplained)
- Weight gain >5 kg
- Peripheral edema
- Pleural or pericardial effusion
- Pulmonary infiltrates / hypoxia (SpO₂ <90%)
- Renal failure (Cr rising)
- Hypotension
| Severity | Features | Action |
|---|---|---|
| Mild | 2 criteria, no hypoxia | Dexamethasone 10 mg IV Q12h; continue ATRA/ATO |
| Moderate | 3+ criteria, no ICU | Dexamethasone 10 mg IV Q12h; hold ATRA (±ATO) temporarily |
| Severe | Respiratory failure / ICU admission / Renal failure | Hold both ATRA and ATO; Dexamethasone 10 mg Q12h; ICU support; restart only after full resolution |
- Continue dexamethasone minimum 3 days, until complete resolution, then taper
- If rising WBC: add hydroxyurea ± cytarabine for cytoreduction
- Furosemide for fluid overload
- Resume ATRA/ATO at full dose once DS resolves (even severe cases can be restarted)
PART D: RELAPSED APL
D1. Confirm Relapse
- Molecular relapse: Rising PCR (2 consecutive positive results from PML-RARA negative baseline) - treat immediately, don't wait for morphologic relapse
- Hematologic relapse: Reappearance of leukemic promyelocytes in blood/marrow
D2. Salvage Therapy
If prior therapy was ATRA-chemotherapy (AIDA-based):
| Regimen | CR2 Rate |
|---|---|
| ATO monotherapy (0.15 mg/kg/day) | ~80-90% |
| ATRA + ATO | ~85% |
| ATRA + ATO + GO | ~90% |
If prior therapy was ATRA-ATO (APL0406/APOLLO):
- ATRA + GO (gemtuzumab ozogamicin 9 mg/m² day 1, 15)
- ATRA + idarubicin-based chemotherapy + ATO
- Clinical trial enrollment strongly recommended
D3. Transplantation in Relapsed APL
| Modality | EFS | OS | NRM |
|---|---|---|---|
| Auto-HCT | 71% | 82% | 5% |
| Allo-HCT | 54% | 58% | 29% |
| Relapse rate | 24% | - | Auto |
| Relapse rate | 23% | - | Allo |
- In modern ATRA-ATO era: 5-year OS with salvage = 71%
- SCT may NOT be needed after first relapse-CR2 in the ATO era (outcomes similar with vs. without SCT, P=0.848)
- Reserve allo-HCT for: PCR-positive at HCT, second or later relapse, inability to achieve molecular CR
Molecular or hematologic relapse
↓
Start ATO ± ATRA ± GO salvage
↓
Achieve molecular CR2 (PCR negative)
↓
If PCR negative: Auto-HCT (preferred)
If PCR positive: Allo-HCT (GVL needed)
If unable to achieve CR2: Clinical trial / Allo-HCT
LANDMARK AND LATEST TRIALS - COMPLETE TIMELINE
THE LANDMARK TRIALS EVERY HEMATOLOGIST MUST KNOW
1. ATRA Discovery - Shanghai 1988 (Huang et al., Blood 1988)
- What: First clinical use of pharmacologic ATRA in 24 APL patients
- Result: CR rate 96% - unheard of at the time
- Impact: Transformed APL from a rapidly fatal disease to a curable one overnight
- Evidence level: Historical cohort; no RCT needed - effect size was enormous
2. European APL Group - Fenaux et al., Blood 1993 (n=101)
- What: Randomized: ATRA → chemo vs. ATRA + chemo concurrent vs. chemo alone
- Result: 2-year DFS: concurrent ATRA-chemo 79% > ATRA then chemo 62% > chemo 50%
- Impact: Established concurrent ATRA + chemotherapy as standard of care
3. AIDA Trial - GIMEMA/PETHEMA 1997
- What: ATRA + idarubicin (no cytarabine) induction + anthracycline consolidation
- Result: CR ~95%; 5-year OS ~80%
- Impact: AIDA became the global chemotherapy-based standard for ~15 years
- Legacy: Still used when ATO is contraindicated
4. ATO in Relapsed APL - Shen et al., Blood 1997 (China)
- What: Arsenic trioxide monotherapy in relapsed/refractory APL
- Result: CR rate 85% with ATO alone
- Impact: Proved ATO was the single most active agent in APL; launched the ATO revolution
5. APL0406 Trial - Lo-Coco et al., NEJM 2013 ⭐ THE LANDMARK
- Design: Phase III RCT, n=156, non-high-risk APL (WBC ≤10 × 10⁹/L)
- Arms: ATRA + ATO (no chemo) vs. ATRA + idarubicin-chemo
- Results:
| Outcome | ATRA-ATO | ATRA-CHT | P value |
|---|---|---|---|
| CR rate | 100% | 95% | 0.12 |
| 2-year EFS | 97% | 86% | 0.02 (superior) |
| 2-year OS | 99% | 91% | 0.02 |
| Hematologic toxicity | Less | More | Significant |
| Infections | Fewer | More | Significant |
- Impact: Established ATRA + ATO as the new standard of care - eliminated chemotherapy from non-high-risk APL
- No maintenance needed in ATRA-ATO arm
- This single trial changed practice worldwide
6. APL0406 Final Analysis - Platzbecker et al., JCO 2017
- Median follow-up 40.6 months; 276 patients
- 50-month EFS: 97.3% vs. 80% (P<0.001)
- 50-month CIR: 1.9% vs. 13.9% (P=0.0013)
- 50-month OS: 99.2% vs. 92.6% (P=0.0073)
- 2 therapy-related myeloid neoplasms in chemo arm, zero in ATRA-ATO arm
- Impact: Confirmed superiority increases over time; definitively eliminated chemo from standard-risk APL
7. AML17 Trial - Burnett et al., Lancet Oncol 2015 (UK AML Working Party)
- Design: Phase III RCT, n=235 non-high-risk APL
- Arms: ATRA + ATO (alternative schedule: 0.3 mg/kg days 1-5, then 0.25 mg/kg twice weekly) vs. ATRA + IDA-based chemo ± GO
- Results: Lower relapse, better survival with ATRA-ATO
- 2-year OS: 93% ATRA-ATO vs. 89% ATRA-chemo
- Impact: Validated APL0406 findings with a different ATO dosing schedule; confirmed global applicability
8. APL15 Trial - Wang et al., Blood Cancer J 2022 ⭐ EXTENDS TO HIGH-RISK
- Design: Phase III non-inferiority RCT; Chinese multi-center; n=128 all-risk APL
- Arms: ATRA-ATO alone (+ hydroxyurea for WBC control) vs. ATRA-ATO + chemotherapy
- Key question: Can chemotherapy be eliminated even in high-risk APL?
- Results (high-risk subgroup):
| Outcome | ATRA-ATO only | ATRA-ATO + CHT | P |
|---|---|---|---|
| CR rate | 97% | 97% | NS |
| 2-year DFS | 94% | 87% | 0.52 (non-inferior) |
| 2-year EFS | 85% | 78% | 0.44 (non-inferior) |
- Impact: First RCT to show chemotherapy may be unnecessary even in high-risk APL, using ATO + ATRA + hydroxyurea alone
9. APOLLO Trial - Platzbecker, Adès, Montesinos et al., JCO 2025 ⭐ LATEST LANDMARK
- Design: Phase III RCT; European multicenter; specifically in high-risk APL (WBC >10,000/μL); n=133
- ATRA-ATO arm: ATRA + ATO + idarubicin days 1 & 3 only → then 4 cycles ATRA-ATO consolidation (no maintenance)
- ATRA-CHT arm: Classic AIDA induction → anthracycline consolidation × 3 cycles → 2 years maintenance
- Primary endpoint: 2-year EFS
| Outcome | ATRA-ATO + 2-dose IDA | ATRA-CHT (AIDA) | P |
|---|---|---|---|
| 2-year EFS | 88% | 71% | 0.02 |
| CR rate | 93% | 90% | 0.654 |
| Molecular relapse | 1.5% | 12.3% | 0.014 |
| Serious adverse events | 32% | 68% | <0.01 |
| Neutropenia (induction) | 22% | 46% | 0.005 |
- CONCLUSION: ATRA + ATO + minimal idarubicin is superior to ATRA-AIDA in high-risk APL
- No maintenance therapy needed in ATRA-ATO arm
- This trial NOW extends the ATRA-ATO paradigm to ALL risk groups
10. AAML1331 (Children's Oncology Group) - Kutny et al., JAMA Oncol 2022
- Pediatric APL: ATRA + ATO equivalent to ATRA + chemotherapy in children
- Confirmed ATRA-ATO can safely replace chemotherapy in pediatric standard-risk APL
- Impact: Extended chemotherapy-free treatment to children
11. Meta-Analysis - Ahmad et al., BMC Cancer 2026
- 12 studies, GRADE framework
- ATRA + ATO vs. ATRA + CHT across all risk groups:
| Outcome | RR | 95% CI | Significance |
|---|---|---|---|
| CR rate | 1.04 | 1.02-1.06 | Significant |
| DFS | 1.22 | 1.11-1.34 | Significant |
| EFS | 1.25 | 1.20-1.29 | Significant |
| OS | 1.07 | 1.03-1.12 | Significant |
| QTc prolongation | 3.79 | 1.00-14.36 | P=0.05 (higher with ATO) |
- CONCLUSION: ATRA + ATO superior in all survival outcomes; close cardiac monitoring for QTc is mandatory
COMPLETE MANAGEMENT ALGORITHM (2026)
APL SUSPECTED → ATRA 45 mg/m²/d IMMEDIATELY + Coagulopathy support
↓
Confirm PML-RARA (FISH/PCR)
↓
RISK STRATIFY (WBC at diagnosis)
/ \
WBC ≤10,000/μL WBC >10,000/μL
(Standard Risk) (High Risk)
↓ ↓
ATRA + ATO Add cytoreduction ASAP:
(Lo-Coco protocol) - Hydroxyurea 0.5-1g Q6-8h
↓ - Dexamethasone 10 mg Q12h
Monitor WBC; - Watch for DS aggressively
add HU if rising ↓
↓ ┌──────────────────────────────────┐
↓ │ ATRA + ATO + IDA days 1&3 │
↓ │ (APOLLO - PREFERRED, 2025) │
↓ │ OR │
↓ │ ATRA + ATO + IDA days 2,4,6,8 │
↓ │ (APML4) │
↓ │ OR (if ATO contraindicated) │
↓ │ ATRA + AIDA │
↓ └──────────────────────────────────┘
↓ ↓
INDUCTION RESPONSE ASSESSMENT (Day 28-42 BM biopsy)
↓
Morphologic CR achieved?
↓ Yes
┌──────────────────────────┐
│ 4 cycles ATRA + ATO │
│ Consolidation │
│ (~28 weeks total) │
└──────────────────────────┘
↓
PCR PML-RARA after final cycle
↓
┌──────────────────────┐
│ PCR negative │ → CURE. Surveillance PCR q3mo × 2yr
└──────────────────────┘
┌──────────────────────┐
│ PCR positive │ → Molecular relapse protocol
└──────────────────────┘
↓
RELAPSE PATHWAY
↓
ATO ± ATRA ± GO salvage → CR2
↓
PCR negative: Auto-HCT (preferred)
PCR positive: Allo-HCT
Multiple relapse: Clinical trial
QUICK REFERENCE DRUG DOSING CARD
| Drug | Dose | Route | Indication |
|---|---|---|---|
| ATRA | 45 mg/m²/day ÷ 2 doses | PO | All risk, induction + consolidation |
| ATO (IV) | 0.15 mg/kg/day (cap 10 mg) | IV over 2h | All risk, induction + consolidation |
| ATO (oral) | 10 mg/day | PO | Equivalent to IV (emerging) |
| Idarubicin (APOLLO) | 12 mg/m² | IV | Days 1 & 3 (high risk) |
| Idarubicin (APML4) | 12 mg/m² | IV | Days 2,4,6,8 (high risk) |
| Hydroxyurea | 500-1000 mg Q6-8h | PO | WBC control (high risk induction) |
| Dexamethasone | 10 mg Q12h | IV/PO | DS prophylaxis/treatment |
| Gemtuzumab (GO) | 9 mg/m² D1, D15 | IV | Cardiac contraindication / relapse |
| 6-MP (maintenance) | 50-90 mg/m²/day | PO | After AIDA only |
| MTX (maintenance) | 5-15 mg/m²/week | PO | After AIDA only |
KEY CLINICAL PEARLS FROM WORLD-CLASS HEMATOLOGISTS
-
The biggest killer in APL is the first 48 hours - hemorrhagic death before ATRA is started. Every hour without ATRA is dangerous. Start empirically on clinical suspicion alone.
-
ATRA-ATO is now the paradigm for ALL risk groups (after APOLLO 2025) - chemotherapy's role is being reduced to 2 doses of idarubicin at most in high-risk, and zero doses in standard-risk.
-
Differentiation syndrome is a clinical diagnosis - don't wait for all criteria. Start dexamethasone early. Mortality drops from 10% to near zero with early treatment.
-
PCR-negativity after consolidation is the cure criterion - not just morphologic CR. A patient who is morphologically in CR but PCR-positive after final consolidation will relapse.
-
Oral ATO (10 mg/day) is bioequivalent to IV - game-changing for resource-limited settings and outpatient care. APL can become an outpatient-treated disease.
-
In the ATO era, SCT for relapsed APL may be optional - MDACC data (Sasaki 2024) show similar outcomes with or without transplant after first relapse if molecular CR is achieved with ATRA-ATO salvage.
-
FLT3-ITD mutation in APL - present in ~30-40% of high-risk/M3v APL. Not yet a treatment-changing finding (does not affect ATRA-ATO response), but flags higher-risk biology.
-
PLZF-RARA is ATRA-resistant - if the patient is not responding morphologically to ATRA, question the diagnosis and check for variant translocation.
- Harrison's Principles of Internal Medicine 22E (2025), p.877
- Goldman-Cecil Medicine, Table 168-3
- Lo-Coco F et al., NEJM 2013 - APL0406 initial (PMID 23841729)
- Platzbecker U et al., JCO 2017 - APL0406 final (PMID 27400939)
- Platzbecker U et al., JCO 2025 - APOLLO Trial (PMID 40825164)
- Wang HY et al., Blood Cancer J 2022 - APL15 Trial (PMID 36404343)
- Ahmad H et al., BMC Cancer 2026 - 2026 meta-analysis (PMID 41906112)
- Mohty R et al., Transplant Cell Ther 2024 - HCT in relapsed APL (PMID 38554737)
- Sasaki K et al., Clin Lymphoma Myeloma Leuk 2024 - Relapsed APL outcomes (PMID 38431521)
- Chin KK & Tallman MS, Curr Opin Oncol 2025 - Curative strategies high-risk APL (PMID 41029961)
- Alberta Health Services APL Guideline, revised October 2025
- NCCN AML Guidelines v3.2026
Write note on kimura disease all including from top to bottom
Kimura disease clinical features treatment management
Kimura disease pathology epidemiology diagnosis treatment 2024 2025 comprehensive review
PMID: 40549072
PMID: 41070115
https://pmc.ncbi.nlm.nih.gov/articles/PMC12185846
Kimura disease nephropathy renal involvement treatment
https://www.dovepress.com/kimura-disease-retrospective-analy…
Kimura disease dupilumab omalizumab biologic therapy
PMID: 37950550
KIMURA DISEASE - A Complete Clinical Note
1. DEFINITION
- Painless subcutaneous nodules predominantly in the head and neck region
- Peripheral blood eosinophilia
- Markedly elevated serum IgE
- Fitzpatrick's Dermatology, p.697-699
- Comprehensive Clinical Nephrology, 7th Edition, p.416
- K.J. Lee's Essential Otolaryngology
2. HISTORICAL BACKGROUND
| Year | Milestone |
|---|---|
| 1937 | First described by Kimm and Szeto (Chinese literature) as "eosinophilic hyperplastic lymphogranuloma" |
| 1948 | Formally named and characterized by Kimura et al. in Japanese literature |
| 1969 | Angiolymphoid hyperplasia with eosinophilia (ALHE) described by Wells and Whimster - initially thought to be the same disease; later proven to be a separate entity |
| 1980s | Renal involvement (nephrotic syndrome) recognized as a significant association |
| 2020s | Biologic therapies (dupilumab, mepolizumab, omalizumab) emerging as promising treatments for refractory disease |
3. EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Incidence | Rare - exact prevalence unknown; predominantly reported in East and Southeast Asia |
| Geography | Highest in Japan, China, Southeast Asia; sporadic in Europe, Middle East, USA |
| Sex | Strongly male predominant (M:F ratio ~6-9:1; 88.7% male in large Chinese series, Zhu et al. 2025) |
| Age | Mainly affects young to middle-aged adults; peak in 3rd-5th decade (mean age ~41 years in recent series) |
| Race | Predominantly Asian, but all races affected; not exclusively Asian |
| Median time to diagnosis | ~24 months from symptom onset (reflecting diagnostic delay) |
Notable: A retrospective series from the US Armed Forces Institute of Pathology found 7 whites, 6 African Americans, 6 Asians among 21 cases - illustrating that Kimura disease must be considered in any racial group.
4. ETIOLOGY AND PATHOGENESIS
4.1 Th2-Driven Immune Dysregulation (Most Accepted Theory)
- KD is driven by aberrant Th2 immune responses
- Th2 cytokines (IL-4, IL-5, IL-13) promote:
- IgE class switching → markedly elevated serum IgE
- Eosinophil recruitment and survival (IL-5) → tissue eosinophilia
- Mast cell activation → pruritus, allergic features
- The pathogenesis parallels atopic disease, explaining the frequent co-occurrence with asthma and allergic rhinitis
4.2 Proposed Triggers
- Allergic reaction/hypersensitivity - supported by elevated IgE and eosinophilia
- Parasitic infection - geographic distribution, eosinophilia; however, no consistent pathogen identified
- Autoimmune mechanism - salivary gland involvement, lymphoid hyperplasia, renal immune complex deposition
- Viral trigger - speculated but unproven
4.3 Molecular Pathways (Recent Evidence)
- PDGF-α and c-kit expression found in KD tissue → rationale for tyrosine kinase inhibitors (imatinib), though not yet used clinically
- IgG4-related disease overlap - 11.3% of KD patients have co-existing IgG4-RD (Zhu et al. 2025), suggesting overlapping fibroinflammatory mechanisms
- Type 2 inflammation pathway (IL-4/IL-5/IL-13/IgE axis) - supported by responses to biologic agents targeting these pathways
5. PATHOLOGY / HISTOPATHOLOGY
5.1 Gross Pathology
- Firm, poorly circumscribed nodules in subcutaneous tissue
- Often involves adjacent lymph nodes and salivary glands
- No capsule; infiltrative margins
5.2 Microscopic Features (Diagnostic)
| Feature | Description |
|---|---|
| Lymphoid follicles | Prominent lymphoid follicular hyperplasia with well-formed germinal centers (dominant feature) |
| Eosinophilic infiltration | Dense eosinophil infiltration in interfollicular areas and germinal centers |
| Eosinophilic abscesses | Aggregates of eosinophils forming microabscesses (characteristic of KD) |
| Eosinophilic folliculosis | Eosinophils infiltrating germinal centers |
| Vascular changes | Perivenular sclerosis, vascular proliferation (less prominent than ALHE) |
| Fibrosis | Dense fibrosis present (characteristic - helps distinguish from ALHE) |
| Mast cells | Present but fewer than ALHE |
| Architecture | Lymph node architecture maintained (helps exclude lymphoma) |
5.3 Immunohistochemistry
| Marker | Result |
|---|---|
| CD20 | Positive (B cells in follicles) |
| CD3 | Positive (T cells in interfollicular areas) |
| IgE | Positive on mast cells/eosinophils |
| S-100 | Negative (helps distinguish from Rosai-Dorfman) |
| CD34, CD31 | Vessels positive (endothelial markers) |
| Ki-67 | Low (benign; helps exclude lymphoma) |
| EBV | Negative |
6. CLINICAL FEATURES
6.1 Primary Presentation
- Painless subcutaneous nodules - most common presenting feature
- Location: head and neck (83%) - most commonly preauricular, retroauricular, submandibular, posterior neck regions
- Nodules: slow-growing, diffuse, poorly defined; median size ~3.0 cm
- Bilateral in 66% of cases (Zhu et al. 2025)
- Pruritus overlying nodules - present in ~52.8%; increases with age
6.2 Site-Specific Features
| Site | Features |
|---|---|
| Parotid gland | Unilateral (more common) or bilateral parotid swelling; presents like a parotid mass |
| Submandibular gland | Firm, non-tender swelling in submandibular region |
| Regional lymph nodes | Cervical lymphadenopathy, characteristically non-tender |
| Orbit/periorbital | Less common; can cause proptosis (reported in Asian patients) |
| Axillary/inguinal | Rare extracervical involvement |
| Limb lesions | Very rare; reported (case reports of arm involvement, Mulla et al. 2022) |
6.3 Systemic and Associated Features
| Feature | Frequency / Details |
|---|---|
| Peripheral eosinophilia | Nearly universal; mean eosinophil count ~2.09 × 10⁹/L; correlates with mass size and disease activity |
| Elevated serum IgE | Nearly universal; mean ~1069 IU/mL (normally <100 IU/mL); marker of disease activity |
| Nephrotic syndrome (renal involvement) | 10-20%; due to membranous nephropathy (MN), FSGS (tip lesion variant), or mesangial proliferative GN (MesPGN) |
| Asthma | 9.4% of cases (Zhu et al. 2025); shares Th2 immune mechanism |
| Allergic rhinitis | Common concurrent atopic condition |
| IgG4-related disease overlap | 11.3% (emerging association) |
| Thrombotic events | 9.4% - rare but important; brain embolism reported from KD-induced thrombi |
| Immune thrombocytopenia | Occasionally reported |
7. LABORATORY INVESTIGATIONS
7.1 Blood Tests
| Test | Finding | Significance |
|---|---|---|
| CBC with differential | Eosinophilia (often >10% of WBC; absolute count >0.5 × 10⁹/L) | Almost universal; correlates with mass size and disease activity |
| Serum IgE | Markedly elevated (often >1000 IU/mL) | Pathognomonic lab finding; disease activity marker |
| Serum eosinophil cationic protein (ECP) | Elevated | Parallels disease course; useful for monitoring |
| Total protein / albumin | Low if nephrotic syndrome | |
| BUN / Creatinine | Elevated if renal involvement | Screen all patients |
| Urinalysis | Proteinuria (nephrotic range if renal disease) | Mandatory screen |
| IgG subclasses (IgG4) | Elevated in overlap cases | Check if IgG4-RD suspected |
| ANA, ANCA | Negative (helps exclude vasculitis/SLE) | |
| ESR / CRP | Mildly elevated | Nonspecific |
7.2 Imaging
| Modality | Findings |
|---|---|
| Ultrasound (US) | Hypoechoic, homogeneous subcutaneous masses; helpful to characterize and guide biopsy |
| CT scan | Well-defined hyperdense soft tissue masses; lymph node enlargement; involvement of salivary glands; no necrosis or calcification |
| MRI | T1 iso/hypointense, T2 hyperintense masses; good for surgical planning; better soft tissue delineation |
| PET-CT | Variable FDG uptake; used mainly to exclude lymphoma; can show hypermetabolic nodes |
7.3 Tissue Biopsy (Mandatory for Diagnosis)
- Incisional biopsy is recommended (over needle biopsy for adequate tissue)
- Biopsy of the subcutaneous nodule and/or lymph node
- Light microscopy + immunohistochemistry required
- Diagnosis is histopathologic - there are no pathognomonic serologic tests
8. DIAGNOSIS
Diagnostic Criteria (No formal validated criteria, but commonly used features):
- Painless subcutaneous nodule(s) in head and neck
- Peripheral eosinophilia
- Elevated serum IgE
9. DIFFERENTIAL DIAGNOSIS
9.1 Most Important: Kimura Disease vs. ALHE
| Feature | Kimura Disease | ALHE (Epithelioid Hemangioma) |
|---|---|---|
| Age | 30-60 years | 20-50 years |
| Sex | Strongly male | Slight female predominance |
| Race | Predominantly Asian | All races equally |
| Lesion size | Larger (often >3 cm) | Small (<1 cm) |
| Depth | Deep subcutaneous | Superficial dermal |
| Location | Subcutaneous, lymph nodes, salivary glands | Dermal papules/nodules |
| Symptoms | Generally painless/asymptomatic | May be painful, pruritic, pulsatile |
| Lymph node involvement | Yes (prominent) | Rare |
| Dominant histology | Lymphoid follicular hyperplasia | Vascular proliferation with hobnail endothelial cells |
| Vascular hyperplasia | Less prominent | Prominent (defining feature) |
| Fibrosis | Prominent | Limited/absent |
| Eosinophils | More abundant (abscesses) | Variable (inconspicuous to numerous) |
| Mast cells | Fewer | More |
| Serum IgE | Markedly elevated | Normal |
| Serum eosinophilia | Present (prominent) | Present (mild) |
| Renal disease | Yes (10-20%) | No |
9.2 Broader Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Lymphoma (Hodgkin/NHL) | B symptoms (fever, night sweats, weight loss); abnormal LDH; no eosinophilia/IgE elevation; histology - abnormal lymphocyte morphology; Reed-Sternberg cells in HL; clonal B or T cell population |
| Castleman disease | Hyaline-vascular or plasma cell type; characteristic "lollipop" histology; no eosinophilic abscesses |
| IgG4-related disease | Storiform fibrosis, obliterative phlebitis, IgG4+ plasma cells; elevated serum IgG4; can overlap with KD |
| Langerhans cell histiocytosis (eosinophilic granuloma) | CD1a+, S-100+, Langerin+ (CD207) Langerhans cells; Birbeck granules on EM |
| Rosai-Dorfman disease | Emperipolesis (lymphocytes inside histiocytes); S-100+, CD68+; no eosinophilic abscesses |
| Parotid gland neoplasms | Firm parotid mass; imaging shows intraparotid lesion; biopsy required |
| Pyogenic granuloma | Vascular, bleeds easily; lobular capillary hemangioma histology |
| Kaposi sarcoma | HHV-8+; spindle cell proliferation; slit-like vascular spaces |
| Reactive lymphadenopathy (infectious) | Tender; associated infection/fever; resolves with antibiotics |
| Parasitic infestation | Eosinophilia + history of exposure; serologic testing positive |
| Benign lymphoepithelial lesion | Salivary gland; myoepithelial islands; associated with Sjögren's |
10. RENAL INVOLVEMENT IN KIMURA DISEASE
10.1 Glomerular Patterns
| Glomerular Disease | Frequency |
|---|---|
| Membranous nephropathy (MN) | Most common |
| Focal segmental glomerulosclerosis (FSGS) - tip lesion variant | Second most common |
| Mesangial proliferative GN (MesPGN) | Less common |
10.2 Clinical Presentation of Renal Disease
- Nephrotic syndrome (proteinuria >3.5g/day, hypoalbuminemia, edema, hyperlipidemia)
- Microscopic hematuria occasionally
- Renal function usually preserved initially but can decline
10.3 Pathogenesis of Renal Involvement
- Immune complex deposition (IgE-containing complexes) in glomeruli
- Eosinophil-mediated glomerular injury
- Th2 cytokine-driven mesangial proliferation
10.4 Investigation for Renal Involvement (All KD Patients)
- Urinalysis + microscopy (protein, casts)
- 24-hour urine protein (or protein/creatinine ratio)
- BUN, creatinine, albumin
- Renal ultrasound if proteinuria
- Renal biopsy if nephrotic range proteinuria
10.5 Management of Renal Disease
- Influences treatment choice for KD (see management section)
- Steroid therapy most effective when nephrotic syndrome is present
- Steroid-sparing agents for relapsing/steroid-dependent nephrotic syndrome
11. MANAGEMENT
11.1 Treatment Ladder
Asymptomatic / mild disease
↓
Observation (watchful waiting)
↓
Single/limited nodules without renal disease
↓
Surgery (first-line when feasible)
↓
Multiple/diffuse nodules / recurrence / renal involvement
↓
Systemic corticosteroids
↓
Refractory / steroid-dependent / recurrent
↓
Steroid-sparing immunosuppressants
↓
Refractory / severe / recurrent with atopic features
↓
Biologic therapy (dupilumab / mepolizumab / omalizumab)
OR Radiotherapy (for localized/unresectable disease)
11.2 Observation (Watchful Waiting)
- Appropriate for asymptomatic, small, stable lesions with no renal involvement
- Regular monitoring: blood count, IgE, urinalysis every 3-6 months
- No treatment needed if no progression
11.3 Surgery
- Modality of choice for localized, resectable disease
- Achieves histologic diagnosis + therapeutic excision simultaneously
- Most common initial treatment (62.3% in Zhu et al. 2025 series)
- Limitation: high recurrence rate - lesions recur in draining lymphatics and adjacent tissues
- Not curative for multifocal or diffuse disease
- Facial disfigurement is a concern with large cervicofacial lesions
- Photodynamic therapy has been used for postsurgical facial disfigurement (Abbas et al., case report)
11.4 Systemic Corticosteroids
| Parameter | Details |
|---|---|
| Drug | Prednisolone / prednisone |
| Dose | 0.5-1 mg/kg/day |
| Response | Good initial response - nodules shrink, eosinophilia improves, IgE decreases |
| Limitation | Relapse upon tapering is common - most patients require prolonged low-dose maintenance or steroid-sparing agents |
| Renal disease | Steroid therapy is the treatment of choice for nephrotic syndrome associated with KD |
| Maintenance | Low-dose prednisolone (5-10 mg/day) often continued long-term to prevent relapse |
Comprehensive Clinical Nephrology: "Steroid therapy is successful in most cases, although relapse upon tapering is common."
11.5 Steroid-Sparing / Immunosuppressive Agents
| Agent | Evidence | Notes |
|---|---|---|
| Cyclosporine A | Case series; established use | Effective for both nodules and renal disease; nephrotoxic long-term |
| Tacrolimus | Anecdotal reports | Alternative calcineurin inhibitor |
| Mycophenolate mofetil (MMF) | Anecdotal reports | Used especially for renal disease |
| Leflunomide | Case reports | Anecdotal; limited data |
| Tripterygium wilfordii (Chinese herb extract) | Anecdotal (Asian case series) | Anti-inflammatory; used in China |
| Vincristine | Rare case reports | Cytotoxic; last resort |
| Imatinib (tyrosine kinase inhibitor) | Theoretical (PDGF-α/c-kit expression in KD tissue) | Not yet used clinically; promising rationale |
11.6 Radiotherapy
| Parameter | Details |
|---|---|
| Indications | Unresectable disease; post-surgical recurrence; multiple/diffuse nodules; patient refusing surgery |
| Dose | Typically 24-30 Gy over 3-4 weeks |
| Response rate | ~90% response; durable remission in many cases |
| Advantage | Can treat large or diffuse fields; does not require repeated surgery |
| Disadvantage | Long-term risks (secondary malignancy, skin changes); not first-line in young patients |
| Renal disease | Less effective for nephrotic syndrome (steroids preferred for renal component) |
11.7 Biologic Therapies - THE EMERGING FRONTIER (2022-2025)
A. Dupilumab (IL-4Rα antagonist - blocks IL-4 and IL-13 signaling)
- Rationale: IL-4/IL-13 drive IgE class switching and Th2 responses in KD
- Multiple case reports (2022-2024) showing efficacy:
- Shang et al. (2023): Significant clinical response
- Battesti et al., Clin Exp Dermatol (2024): 2 dupilumab-responsive cases
- Luo et al., Int Immunopharmacol (2024): Dupilumab effective with literature review
- Yang et al., Front Immunol (2022): Response independent of IgE level - suggests mechanism beyond just IgE suppression
- Liu et al., QJM (2024): Efficacy and safety of dupilumab confirmed
- Works even in IgE-independent fashion, targeting the upstream Th2 pathway
- Growing evidence base - becoming the most studied biologic for KD
B. Mepolizumab (Anti-IL-5 - depletes eosinophils)
- Rationale: IL-5 is the principal eosinophil survival factor
- Zhu et al. (J Inflamm Res, 2025, PMID 41070115) - 3 mepolizumab-responsive cases:
- Lymph node shrinkage
- Pruritus reduction (VAS 8 → 2)
- Eosinophilia improved over time
- Corticosteroids successfully tapered off within 6 months
- Dose: 200 mg every 4 weeks (also 100 mg every 4 weeks used)
- Particularly useful when asthma coexists (KD + asthma = both benefit from IL-5 blockade)
- Serum IgE remained elevated despite clinical response (IgE not a surrogate marker of mepolizumab response)
C. Omalizumab (Anti-IgE)
- Rationale: Directly neutralizes free IgE; prevents IgE-mediated mast cell/basophil activation
- Ao et al. (J Dermatol, 2024, PMID 37950550) - 2 refractory cases responded to low-dose steroid + omalizumab; reviewed 13 biologic-treated KD cases
- Reduces IgE-mediated inflammation
- Less consistent response than dupilumab; IgE levels may remain elevated
D. Benralizumab (Anti-IL-5Rα)
- Rapidly depletes eosinophils by ADCC
- Limited case reports; promising based on mechanism
E. Rituximab (Anti-CD20 B-cell depletion)
- Reviewed in Ao et al. 2024 series
- Used in cases with B-cell-driven lymphoid hyperplasia component
- Less evidence than dupilumab/mepolizumab
Th2 immune dysregulation in KD:
↓
IL-4 / IL-13 pathway
→ IgE production
→ Mast cell activation ← Omalizumab blocks IgE
→ B cell class switching ← Dupilumab blocks IL-4Rα
+
IL-5 pathway
→ Eosinophil survival/migration ← Mepolizumab/Benralizumab block IL-5
11.8 Antihistamines
- Cetirizine and other antihistamines used for pruritus management
- Not disease-modifying - used adjunctively
- Effective symptomatic relief given the mast cell/IgE-driven itch
11.9 Cryotherapy
- Used occasionally for small superficial lesions
- Limited durability; rarely used as primary therapy
12. MANAGEMENT BY CLINICAL SCENARIO
| Scenario | Preferred Approach |
|---|---|
| Single small nodule, no renal disease | Surgical excision ± observation |
| Multiple nodules, surgically accessible | Surgical excision + corticosteroids if recurrence |
| Diffuse/unresectable disease | Corticosteroids ± radiotherapy |
| Renal involvement (nephrotic syndrome) | Corticosteroids (prednisolone 0.5-1 mg/kg) + cyclosporine if steroid-dependent |
| Recurrence after surgery | Radiotherapy OR corticosteroids |
| Steroid-dependent/refractory, atopic | Dupilumab (best current evidence) |
| Steroid-dependent + coexisting asthma | Mepolizumab (treats both conditions) |
| Very high IgE, refractory | Omalizumab (adjunctive to steroids) |
13. PROGNOSIS
| Feature | Data |
|---|---|
| Overall recurrence rate | ~60% regardless of treatment modality |
| Malignant transformation | Not reported - KD is a benign condition |
| Long-term survival | Normal; not a life-threatening disease per se |
| Main morbidity | Repeated recurrences; renal disease; disfigurement from large lesions or repeated surgery |
| Renal prognosis | Generally good with steroids; progressive renal failure rare but possible if nephrotic syndrome undertreated |
| Spontaneous remission | Reported in rare cases; not reliable |
Factors associated with recurrence:
- Large lesion size
- Bilateral disease
- Involvement of salivary glands
- Inadequate initial treatment
- Delay in diagnosis (median 24 months in current series)
14. MONITORING PLAN
| Timepoint | Tests |
|---|---|
| At diagnosis | CBC with diff, IgE, urinalysis, protein/creatinine ratio, BUN, creatinine, albumin |
| Every 3-6 months | CBC, IgE, eosinophil count (disease activity markers), urinalysis |
| When on steroids | Glucose, BP, bone density, ophthalmology (glaucoma/cataracts) |
| When on cyclosporine | Creatinine, BP (nephrotoxicity monitoring) |
| When on biologics | CBC, IgE, symptom assessment at each visit |
| Post-treatment | Annual CBC, IgE, urinalysis × 5 years minimum |
15. SUMMARY TABLE
| Domain | Key Points |
|---|---|
| Disease | Benign, chronic inflammatory disorder; unknown etiology |
| Mechanism | Th2 immune dysregulation → IL-4/5/13 + IgE overproduction + eosinophilia |
| Who | Young Asian males predominantly; M:F ~9:1 |
| Where | Head and neck (83%); subcutaneous + lymph nodes + salivary glands |
| Classic triad | Painless nodule + eosinophilia + elevated IgE |
| Critical DDx | ALHE (separate disease - vascular not lymphoid; no renal disease; superficial) |
| Renal risk | 10-20%; MN, FSGS, MesPGN; nephrotic syndrome |
| Diagnosis | Incisional biopsy - lymphoid follicular hyperplasia + eosinophilic abscesses + fibrosis |
| Surgery | First-line for localized disease; 60% recurrence |
| Steroids | First-line pharmacotherapy; especially with renal disease; relapse common on taper |
| Radiotherapy | 24-30 Gy; for unresectable/recurrent; ~90% response |
| Biologics (emerging) | Dupilumab (best evidence), mepolizumab (with asthma), omalizumab (high IgE) |
| Prognosis | Benign; 60% recurrence; normal life expectancy |
REFERENCES
- Fitzpatrick's Dermatology, 9th Edition, Chapter 40 - Kimura Disease, p.697-699
- Comprehensive Clinical Nephrology, 7th Edition - Kimura Disease, p.416
- Cummings Otolaryngology Head and Neck Surgery - Kimura Disease, Chapter 17
- K.J. Lee's Essential Otolaryngology - Kimura Disease, p.49
- Lagerstrom IT et al., Head Neck Pathol, 2025 - Comprehensive systematic review of KD (PMID 40549072)
- Zhu W et al., J Inflamm Res, 2025 - 53-case retrospective analysis + mepolizumab cases (PMID 41070115)
- Ao S et al., J Dermatol, 2024 - Anti-IgE (omalizumab) + biologic review in KD (PMID 37950550)
- Yang B et al., Front Immunol, 2022 - Dupilumab in KD independent of IgE (PMID 36591252)
- Zhang G et al., BMC Surg, 2020 - Clinical analysis of 24 KD cases from China (PMID 31898499)
- Alberta Health Services / Medscape - Kimura disease treatment protocols (2024-2025)
Refractory itp treatment latest and trials
"immune thrombocytopenia" AND refractory AND treatment
refractory ITP treatment 2024 2025 fostamatinib rilzabrutinib BTK inhibitor TPO agonist ASH guidelines latest trials
"immune thrombocytopenia" AND ("fostamatinib" OR "rilzabrutinib" OR "ianalumab")
https://pmc.ncbi.nlm.nih.gov/articles/PMC11469945
PMID: 40090011
PMID: 41363800
PMID: 38856778
refractory ITP ianalumab VAYHIT2 NEJM 2026 phase 3 results eltrombopag
"immune thrombocytopenia" AND ("rituximab" OR "splenectomy" OR "mycophenolate") AND refractory
PMID: 37735554
"immune thrombocytopenia" AND ("efgartigimod" OR "daratumumab" OR "complement")
PMID: 37778358
PMID: 35417637
Refractory ITP - Complete Expert Hematology Note (2026)
1. DEFINITION OF REFRACTORY ITP
| Term | Definition |
|---|---|
| Refractory ITP (traditional) | Failure to achieve platelet count ≥30 × 10⁹/L (or clinical response) after splenectomy AND after at least one second-line therapy |
| Refractory ITP (practical/ASH) | Persistent or chronic ITP that has failed 2 or more lines of therapy with no sustained response |
| Relapsed/Refractory | ITP that initially responded but relapsed AND did not respond to re-challenge or additional therapies |
| Chronic ITP | Duration >12 months; includes cases unresponsive to multiple therapies |
30-40% of ITP patients develop relapsed/refractory disease after first-line treatment (Washington Manual of Medical Therapeutics). Refractory ITP represents a significant unmet need.
2. PATHOGENESIS (Why ITP Becomes Refractory)
┌─────────────────────────────┐
│ Immune Dysregulation │
└─────────────────────────────┘
│
┌────────────────────────┼────────────────────────┐
▼ ▼ ▼
B-cell Activation T-cell Dysregulation Innate Immunity
→ Autoantibodies → Loss of Treg → Macrophage FcγR
(anti-GPIIb/IIIa, → Th1 > Th2 shift platelet destruction
anti-GPIb/IX) → Direct NK killing
│ │ │
▼ ▼ ▼
IgG-coated platelets Impaired tolerance Spleen/liver clearance
→ Splenic destruction → Cytotoxic T cells → Reduced megakaryopoiesis
│ destroy platelets
▼
FcRn recycling keeps autoantibody levels high
- Expanded autoantibody-secreting long-lived plasma cells (not cleared by rituximab)
- Persistent T-cell–mediated platelet destruction even without antibodies
- Complement activation contributing to platelet lysis
- Impaired megakaryopoiesis (insufficient thrombopoiesis even with normal TPO)
3. TREATMENT OVERVIEW - THE HIERARCHY
First-line (not refractory - background)
- Corticosteroids (dexamethasone 40 mg/day × 4 days, or prednisone 1 mg/kg/day)
- IVIG 1 g/kg × 1-2 doses (for acute bleeding / rapid rise needed)
- Anti-D immunoglobulin (Rh-positive, non-splenectomized only)
Second-line (standard - when steroids fail/relapse)
- TPO receptor agonists (TPO-RAs) - romiplostim, eltrombopag, avatrombopag
- Rituximab - anti-CD20
- Splenectomy
Third-line / Refractory
- Fostamatinib (SYK inhibitor - approved)
- Rilzabrutinib (BTK inhibitor - Phase 3 positive, under regulatory review 2025)
- Efgartigimod (FcRn inhibitor - Phase 3 positive, approved in some indications)
- Ianalumab + eltrombopag (Phase 3 positive, NEJM 2026)
- Immunosuppressives (cyclosporine, mycophenolate, azathioprine, danazol)
- Splenectomy (if not yet done)
- Combination therapies
4. STANDARD SECOND-LINE THERAPIES (Backbone before "refractory" label)
4.1 TPO Receptor Agonists (TPO-RAs)
| Agent | Dose | Route | Response Rate |
|---|---|---|---|
| Romiplostim (Nplate) | 1-10 μg/kg/week (titrate to platelet ≥50 × 10⁹/L) | SC weekly | ~85-90% initial response |
| Eltrombopag (Promacta/Revolade) | 25-75 mg/day (fasting; adjust for East Asian patients) | Oral daily | ~70-80% |
| Avatrombopag (Doptelet) | 20 mg/day, titrate to 40 mg/day | Oral daily | ~65-75% |
- Start 5-7 days to first response; weekly adjustments by 1 μg/kg (romiplostim)
- 90%+ achieve platelet response in the short term
- ~30% achieve sustained treatment-free response after extended use (durable disease modification seen)
- Adverse effects: thromboembolic events (0-9%), bone marrow reticulin (monitor), rebound thrombocytopenia on stopping
- Eltrombopag: food interaction (take fasting 2h before/4h after dairy, antacids, calcium)
- ASH 2025 draft guidelines: TPO-RA is the preferred second-line agent (strong recommendation, moderate certainty)
4.2 Rituximab
| Parameter | Details |
|---|---|
| Dose | 375 mg/m² IV weekly × 4 weeks (standard) OR 100 mg IV × 4 doses (low-dose - similar efficacy, less toxicity) |
| Initial response rate | ~60% |
| Durable remission (platelet >100 × 10⁹/L at 12 months) | ~25% (Washington Manual) |
| Sustained treatment-free response | 20-40% at 2 years; ~15-20% at 5 years |
| Time to response | 4-8 weeks |
| Advantages | Finite course; potential durable cure; no daily medication needed if successful |
| Risks | Infusion reactions; immunosuppression; hepatitis B reactivation (screen before use); PML (rare) |
| ASH 2025 | Conditional recommendation (lower certainty than TPO-RA); preferred in patients who want to avoid chronic medication |
4.3 Splenectomy
| Parameter | Details |
|---|---|
| Response rate | 66-72% durable response (meta-analyses) |
| Complete remission (platelet >150 × 10⁹/L) | ~60-70% |
| Timing | Generally deferred until ITP duration >12 months (many will remit) |
| Advantage | Definitive; medication-free; highest single-modality durable response |
| Disadvantage | Surgical risk; lifelong infection risk; requires vaccines; ~30-40% failure; splenules |
| Pre-operative vaccines | Mandatory: Pneumococcal (PCV13 + PPSV23), Meningococcal (MenACWY + MenB), Haemophilus influenzae type B (HiB); administer ≥2 weeks before surgery |
| Post-splenectomy | Lifelong penicillin prophylaxis in selected high-risk patients |
| Predictor of response | Platelet >150,000/mm³ by POD3 or >500,000/mm³ by POD10 |
| Laparoscopic vs open | Laparoscopic preferred (faster recovery, lower morbidity) |
| Sabiston Surgery: | 2019 meta-analysis: 1-month response rate - splenectomy 86.7% > TPO-RA 65.7% > rituximab 62.1% |
5. REFRACTORY ITP TREATMENT - APPROVED AGENTS
5.1 Fostamatinib (Tavalisse) - FDA Approved 2018
- SYK is critical in FcγR-mediated macrophage phagocytosis of IgG-opsonized platelets
- Blocking SYK reduces platelet destruction without immunosuppression
| Parameter | Data |
|---|---|
| Approved indication | Chronic ITP in adults who have had insufficient response to a previous treatment |
| Dose | 100 mg twice daily; increase to 150 mg BID after 4 weeks if platelet <50 × 10⁹/L |
| Pivotal trials | FIT-1 (PMID 29183881) and FIT-2 (PMID 29183880) - two Phase 3 RCTs |
| Stable response rate (≥50 × 10⁹/L) | ~18% stable response vs. 6% placebo |
| Any platelet response | ~43% achieved ≥50 × 10⁹/L at any timepoint |
| Patient population | Median 3 prior therapies; heavily pretreated |
| Time to response | Median ~15 days in responders |
- Stable response by week 24: OR 0.80 (95% CI 0.72-0.88) - superior to placebo
- Platelet ≥50,000 at week 12: OR 0.80; at week 24: OR 0.82
- Effective even in patients with platelet baseline <15,000/μL
- NNT = 10 (clinically meaningful)
| Side Effect | Relative Risk vs Placebo |
|---|---|
| Diarrhea | RR 2.32 (95% CI 1.11-4.84) |
| Hypertension | RR 2.33 (1.00-5.43) |
| Abnormal LFTs | RR 4.18 (1.00-17.48) |
| Nausea | Not significantly different |
| Rash | Not significantly different |
6. REFRACTORY ITP - LATEST TRIALS AND EMERGING AGENTS (2022-2026)
6.1 RILZABRUTINIB (BTK Inhibitor) - THE BREAKTHROUGH AGENT 2025
- BTK is expressed in B cells AND macrophages
- Dual mechanism:
- Reduces autoantibody production (B-cell receptor signaling blockade)
- Reduces FcγR-mediated platelet phagocytosis by macrophages
- Reversible covalent binding = avoids off-target cardiac/bleeding effects of irreversible BTK inhibitors (ibrutinib)
Phase 1/2 Trial (Kuter et al., NEJM 2022, PMID 35417637)
- n=60 heavily pre-treated adults (median 4 prior therapies, median platelet 15 × 10⁹/L, median disease 6.3 years)
- Dose: 400 mg BID established as optimal
- Platelet response (≥50 × 10³/μL × 2 consecutive): 40%
- Median time to first platelet ≥50 × 10³/μL: 11.5 days (very rapid)
- All treatment-related adverse events grade 1-2; no grade 2+ bleeding or thrombosis
- Conclusion: Active, safe, rapid onset - established 400 mg BID for Phase 3
LUNA 3 Trial - Phase 3 RCT (Kuter et al., Blood 2025, PMID 40090011) ⭐ LANDMARK
- Design: Randomized, double-blind, placebo-controlled, 24-week, multicenter Phase 3
- n=202 adults with persistent/chronic ITP
- Population: Median age 47, 63% female, 7.7-year median ITP duration, 28% prior splenectomy, median 4 prior therapies
- Rilzabrutinib: 400 mg BID (n=133) vs. Placebo (n=69)
| Outcome | Rilzabrutinib | Placebo | P value |
|---|---|---|---|
| Primary: Durable platelet response (≥50 × 10⁹/L for ≥8/12 last weeks, no rescue) | 23% (31/133) | 0% | <0.0001 |
| Platelet response ≥50 (any time, first 12 weeks) | 64% | 32% | Significant |
| Rescue therapy reduction | 52% less | - | P=0.0007 |
| Bleeding score improvement (week 25) | Improved | - | P=0.0006 |
| Physical fatigue improvement | Sustained wk 13-25 | - | P=0.0003 |
| Median time to first platelet response | 15 days | N/A | - |
- Adverse events: predominantly grade 1-2; one serious grade 3 peripheral embolism (multiple risk factors); one death from unrelated pneumonia
- No significant cardiac arrhythmias, hepatic toxicity, or increased major bleeding (unlike irreversible BTK inhibitors)
- ASH 2024 presentation; full publication Blood June 2025
- FDA target action date: August 29, 2025 - regulatory review ongoing
- Conclusion: First BTK inhibitor to show positive Phase 3 results in ITP; first-in-class oral agent with dual mechanism
6.2 EFGARTIGIMOD (FcRn Inhibitor) - ADVANCE IV (Lancet 2023)
- FcRn normally recycles IgG antibodies to prevent their degradation
- Efgartigimod blocks FcRn → accelerates IgG degradation → reduces all IgG subclasses including anti-platelet autoantibodies
ADVANCE IV Trial (Broome et al., Lancet 2023, PMID 37778358)
- Phase 3, multicenter, double-blind, RCT; n=131
- Population: Chronic/persistent ITP; mean 10.6 years since diagnosis; 67% had ≥3 prior ITP treatments; heavily pretreated
- Dose: Efgartigimod 10 mg/kg IV → flexible weekly/every 2 weeks based on platelet count
- Primary endpoint (chronic population): Sustained platelet ≥50 × 10⁹/L for ≥4 of last 6 weeks
| Outcome | Efgartigimod | Placebo | P |
|---|---|---|---|
| Sustained platelet response (primary) | 22% (17/78) | 5% (2/40) | 0.032 |
| Weeks of disease control (median) | 2.0 weeks | 0 weeks | P=0.0009 |
- Well tolerated; most AEs grade 1-2; headache ~16%, no increased serious infections
- SC formulation (efgartigimod PH20 = subcutaneous) also under study; more convenient
- Conclusion: Positive Phase 3; modest but significant response in a very refractory population; IgG-reduction mechanism is broad
- Note: Response rate lower than other agents because population was heavily pretreated (mean 10+ years disease)
6.3 IANALUMAB + ELTROMBOPAG - VAYHIT2 (NEJM April 2026) ⭐ NEWEST LANDMARK
- BAFF-R (B-cell activating factor receptor) is essential for B-cell survival and activation
- Ianalumab depletes B cells via:
- Antibody-dependent cellular cytotoxicity (ADCC)
- BAFF-R signaling blockade → B-cell apoptosis
- Finite course (only 4 monthly infusions) → potential for sustained disease modification after treatment completion
VAYHIT2 Trial (Cuker et al., NEJM 2026, PMID 41363800) - Published April 2026
- Phase 3, multicenter, double-blind, RCT, n=152
- Population: Adults with primary ITP who failed/relapsed after first-line corticosteroids; platelet <30 × 10⁹/L at entry
- Design: 1:1:1 randomization to:
- Ianalumab 9 mg/kg monthly × 4 months + eltrombopag
- Ianalumab 3 mg/kg monthly × 4 months + eltrombopag
- Placebo monthly × 4 months + eltrombopag
- Eltrombopag given in all arms, then tapered and stopped by week 24
| Outcome | Ianalumab 9 mg/kg | Ianalumab 3 mg/kg | Placebo | P |
|---|---|---|---|---|
| Primary: Freedom from treatment failure at 12 months | 54% | 51% | 30% | 0.04 / 0.045 |
| HR treatment failure vs placebo | 0.55 | 0.58 | - | Significant |
| Stable response at 6 months (2nd endpoint) | 62% | - | 39% | 0.045 |
| Serious adverse events | 16% | 6% | 4% | - |
- Published in NEJM April 2026 - the most recent landmark ITP trial
- Key innovation: Short-course biologic (4 doses only) that may modify disease course; allows eltrombopag tapering and stopping
- Higher SAE rate with 9 mg/kg; 3 mg/kg may be preferred safety profile
- ASH 2025 LBA-2 presentation - featured as late-breaking abstract
- Conclusion: Ianalumab + eltrombopag offers a time-limited treatment that modifies disease course in second-line ITP, extending time to treatment failure significantly beyond a TPO-RA alone
6.4 RECOMBINANT HUMAN TPO (rhTPO) - Chinese RCT Data
Liu et al., Platelets 2023 (PMID 36597010)
- Multicenter RCT of different dosing schedules of rhTPO in relapsed/refractory ITP
- rhTPO 300 IU/kg/day × 14 days vs. alternative schedules
- Significant platelet response; shorter time to response with intensive dosing
- Used widely in China; not yet approved in Western countries
6.5 AGENTS IN ONGOING TRIALS
| Agent | Class | Target | Phase | Status |
|---|---|---|---|---|
| Mezagitamab | Anti-CD38 | Plasma cells | Phase 2 | Active - depletes long-lived plasma cells that are rituximab-resistant |
| Daratumumab | Anti-CD38 | Plasma cells | Phase 2 | Case series positive; formal trials ongoing |
| Sutimlimab | Anti-C1s | Complement | Phase 2 | Classical complement pathway inhibition |
| Iptacopan | Factor B inhibitor | Complement | Phase 2 | Alternative pathway inhibition |
| HMPL-523 | SYK inhibitor | FcγR signaling | Phase 3 (China) | NCT05029635 |
| Subcutaneous efgartigimod | FcRn inhibitor | IgG recycling | Phase 3 | SC formulation being studied for convenience |
7. CONVENTIONAL IMMUNOSUPPRESSIVES FOR REFRACTORY ITP
| Agent | Dose | Response Rate | Notes |
|---|---|---|---|
| Cyclosporine A | 2.5-5 mg/kg/day in 2 divided doses | 20-40% | Monitor BP, renal function, drug levels; useful with renal disease or steroid-sparing |
| Mycophenolate mofetil (MMF) | 1-1.5g twice daily | 25-40% | Slower onset (2-3 months); well tolerated; favored in young women (avoid in pregnancy) |
| Azathioprine | 1-2.5 mg/kg/day | 20-40% | Test TPMT activity before starting; 3-6 months for full effect |
| Danazol | 200 mg 2-4× daily | 30-40% | Androgen effects (virilization, liver); useful in elderly/males; reduces FcγR expression |
| Dapsone | 75-100 mg/day | ~40% | Check G6PD before use; hemolysis risk; convenient oral agent |
| Vinca alkaloids | Vincristine 1-2 mg IV, vinblastine 6-10 mg IV weekly | Short-term rescue | Reserved for emergency platelet rise; neuropathy risk with vincristine |
| Cyclophosphamide | 1-2 mg/kg/day or pulse IV | 20-30% | Used in severe refractory; bladder toxicity, hemorrhagic cystitis; fertility impact |
8. COMBINATION THERAPY FOR REFRACTORY ITP
| Combination | Rationale | Evidence |
|---|---|---|
| TPO-RA + rituximab | Raise platelets fast (TPO-RA) + potential durable response (rituximab) | Case series; reasonable practice |
| TPO-RA + fostamatinib | Stimulate production + reduce destruction | Small series; logical combination |
| Ianalumab + eltrombopag | VAYHIT2 - proven Phase 3 combination | NEJM 2026 evidence base |
| Rituximab + dexamethasone (R-Dex) | Higher initial CR rate | Zaja et al., NEJM 2010: CR 63% vs. 36% dexamethasone alone at 6 months |
| Fostamatinib + TPO-RA | Complementary mechanisms | Under study |
| IVIG + TPO-RA (bridging) | Acute bleeding management while TPO-RA takes effect | Standard practice |
9. SPLENIC EMBOLIZATION (Alternative to Splenectomy)
- Partial splenic embolization as alternative/adjunct to splenectomy
- Reduces splenic platelet destruction without surgical risk
- Short-term response comparable to surgery in non-surgical candidates
- Complication rate: Fever, pain (common); infarction, abscess (uncommon)
- Role in refractory ITP still being defined
10. EMERGENCY MANAGEMENT OF REFRACTORY ITP BLEEDING
| Intervention | Dose | Time to Effect | Notes |
|---|---|---|---|
| IVIG | 1 g/kg × 1-2 days | 24-48 hours | First choice for acute rise |
| IV methylprednisolone | 1 g/day × 3 days | 12-24 hours | Rapid steroid pulse |
| Platelet transfusion | 1-2 apheresis units | Immediate (short-lived) | For life-threatening bleeding; use with IVIG for synergy |
| Anti-D (if Rh+, non-splenectomized) | 75 mcg/kg IV | 24-48 hours | Avoid in Hgb <10 (hemolysis risk) |
| rhTPO (China) | 300 IU/kg/day SC | 4-7 days | Available in China |
| Aminocaproic acid / tranexamic acid | TXA 1g Q8h | Immediate | Antifibrinolytic; mucosal bleeding |
| rFVIIa (NovoSeven) | 90 mcg/kg | Rapid | For intracranial hemorrhage; very short-lived platelet rise |
| Emergency splenectomy | - | Hours | If all else fails with life-threatening bleed |
11. ASH 2025 UPDATED DRAFT GUIDELINES - KEY RECOMMENDATIONS
| Question | Recommendation | Strength |
|---|---|---|
| Second-line after corticosteroids | Thrombopoietic agent (TPO-RA) preferred | Strong recommendation, moderate certainty |
| Alternative second-line | Rituximab | Conditional recommendation, low certainty |
| Rituximab preference scenario | Patients who value avoiding chronic daily medication | - |
| BTK inhibitor (rilzabrutinib) | Listed as option alongside fostamatinib | Following LUNA3 data |
| FcRn inhibitor (efgartigimod) | Emerging option for chronic disease | - |
| Thrombotic risk | TPO-RA caution with APS or high thrombotic risk | Consider switch or alternative |
| Maintenance therapy | Goal = safe platelet count with minimum therapy burden | - |
12. COMPLETE MANAGEMENT ALGORITHM (2026)
ITP Diagnosed
↓
TREATMENT INDICATED?
(Platelets <30 × 10⁹/L OR bleeding symptoms)
↓ Yes
FIRST LINE:
Dexamethasone 40 mg × 4 days ± IVIG
↓
Response?
├── Yes → Monitor; manage relapse
└── No / Relapse → SECOND LINE
↓
SECOND LINE:
┌──────────────────────────────────┐
│ TPO-RA (preferred, ASH 2025) │ ← romiplostim / eltrombopag / avatrombopag
│ OR Rituximab (if want finite Rx) │ ← 375 mg/m² × 4 wks
│ OR Splenectomy (if >12 months) │ ← 66-72% durable response
└──────────────────────────────────┘
↓
Response?
├── Yes → Maintain; attempt TPO-RA tapering
└── No / Relapse → REFRACTORY PROTOCOL
↓
REFRACTORY ITP (≥2 lines failed):
┌─────────────────────────────────────────────────────┐
│ APPROVED: │
│ Fostamatinib 100→150 mg BID (SYK inhibitor) │
│ Rilzabrutinib 400 mg BID* (BTK inhibitor) │
│ Efgartigimod IV (FcRn inhibitor) │
│ │
│ COMBINATION (NEJM 2026): │
│ Ianalumab + eltrombopag (if 2nd-line relapse) │
│ │
│ CONVENTIONAL: │
│ Cyclosporine / MMF / Azathioprine / Danazol/Dapsone│
│ │
│ SPLENECTOMY (if not yet done) │
└─────────────────────────────────────────────────────┘
↓
Still refractory?
→ Clinical trial (anti-CD38, complement inhibitors)
→ Combination therapy
→ Palliative/supportive (target platelets >20-30 for safety)
13. LANDMARK AND LATEST TRIALS - TIMELINE
| Year | Trial | Agent | Result | Impact |
|---|---|---|---|---|
| 2003 | Stasi et al. | Rituximab 375 mg/m² × 4 | ~25% durable response | Rituximab enters ITP practice |
| 2008 | Kuter et al., NEJM | Romiplostim | 88% platelet response vs 14% placebo | First TPO-RA approved |
| 2009 | Cheng et al., Lancet | Eltrombopag | Superior to placebo, sustained response | Second TPO-RA; oral option |
| 2010 | Zaja et al., NEJM | R-Dex (rituximab + dex) | CR 63% vs. 36% at 6 months | Combination improves over dex alone |
| 2018 | FIT-1 & FIT-2 | Fostamatinib | Stable response 18% vs 6%; any response 43% | First SYK inhibitor FDA approved for refractory ITP |
| 2021 | Cines et al. | Avatrombopag | Non-inferior to eltrombopag | Third oral TPO-RA option |
| 2022 | Kuter et al., NEJM | Rilzabrutinib Phase 1/2 | 40% response; rapid onset (11.5 days); all AEs grade 1-2 | BTK inhibitor enters ITP trials |
| 2023 | Broome et al., Lancet | Efgartigimod (ADVANCE IV) | 22% sustained response vs 5% placebo | First FcRn inhibitor in ITP; new mechanism |
| 2024 | Tungjitviboonkun et al. | Fostamatinib meta-analysis | NNT=10; confirms efficacy; profiles AEs | Highest level evidence for fostamatinib |
| 2025 (June) | Kuter et al., Blood | Rilzabrutinib LUNA3 Phase 3 | Durable response 23% vs 0% (P<0.0001); rapid 15-day onset; 52% less rescue therapy | First positive Phase 3 BTK inhibitor trial in ITP; FDA review August 2025 |
| 2026 (April) | Cuker et al., NEJM | Ianalumab + eltrombopag (VAYHIT2) | Freedom from treatment failure 54% vs 30% at 12 months (P=0.04); stable response 62% vs 39% | Newest NEJM landmark; short-course B-cell depletion modifies ITP disease course |
14. QUICK COMPARISON TABLE - REFRACTORY ITP AGENTS
| Agent | Class | Route | Durable Response | Key Toxicity | Best For |
|---|---|---|---|---|---|
| Fostamatinib | SYK inhibitor | Oral BID | ~18% stable | HTN, diarrhea, ↑LFTs | Approved, well-tolerated oral option |
| Rilzabrutinib | BTK inhibitor | Oral BID | 23% durable | Grade 1-2 only | Rapidly approved; multiple mechanisms |
| Efgartigimod | FcRn inhibitor | IV weekly/biweekly | 22% sustained | Minimal | Antibody-mediated ITP; long-term disease |
| Ianalumab + ETB | Anti-BAFF-R + TPO-RA | IV monthly × 4 + oral | 54% treatment-free | SAE 16% (9 mg) | 2nd-line relapse; finite course option |
| Romiplostim | TPO-RA | SC weekly | ~30% off-treatment | Thrombosis, reticulin | Ongoing platelet support |
| Eltrombopag | TPO-RA | Oral daily | ~25-30% off-treatment | Thrombosis, hepatotoxicity | Oral daily; most widely used TPO-RA |
| Rituximab | Anti-CD20 | IV × 4 weeks | ~25% at 1 year | Immunosuppression | Finite course; disease modification |
| Splenectomy | Surgery | Procedure | ~66-72% | Surgical + infectious | Best single durable response |
| Cyclosporine | Immunosuppressant | Oral BID | 20-40% | Nephrotoxicity, HTN | Steroid-sparing; renal disease |
| Danazol | Androgen | Oral | 30-40% | Virilization, LFT | Elderly/males; long-term |
REFERENCES
- Washington Manual of Medical Therapeutics - ITP Treatment, p.758
- Sabiston Textbook of Surgery - ITP, second-line therapy, p.1473
- Kuter DJ et al., NEJM 2022 - Rilzabrutinib Phase 1/2 (PMID 35417637)
- Kuter DJ et al., Blood 2025 - LUNA3 Phase 3 rilzabrutinib (PMID 40090011)
- Cuker A et al., NEJM 2026 - VAYHIT2 ianalumab + eltrombopag (PMID 41363800)
- Broome CM et al., Lancet 2023 - ADVANCE IV efgartigimod (PMID 37778358)
- Tungjitviboonkun S et al., Ann Hematol 2024 - Fostamatinib meta-analysis (PMID 38856778)
- Al-Samkari H & Neufeld EJ, Br J Haematol 2023 - Novel therapeutics for refractory ITP (PMID 37735554)
- Egbaria A et al., Br J Haematol 2024 - Splenic embolization meta-analysis (PMID 38544461)
- Ghanima W et al., Hematology ASH Educ Program 2024 - ITP management algorithm (PMID 39643995)
- ASH 2025 Updated Draft Guidelines on Adult ITP (public comment December 2025)
- Sanofi Press Release ASH 2024 - LUNA3 Phase 3 primary results; rilzabrutinib FDA target action date August 29, 2025
Treatment of multiple myeloma and all trials landmark and recent
"multiple myeloma" AND treatment AND ("daratumumab" OR "isatuximab" OR "carfilzomib" OR "elotuzumab")
multiple myeloma treatment 2025 2026 landmark trials GRIFFIN CASSIOPEIA MAIA IMROZ teclistamab bispecific antibody CAR-T latest
PMID: 38084760
PMID: 41363801
PMID: 36762851
"multiple myeloma" AND ("CAR-T" OR "ciltacabtagene" OR "idecabtagene") AND ("relapsed" OR "refractory")
PMID: 37272512
PMID: 38832972
PMID: 39652675
PMID: 39910273
PMID: 40459097
"multiple myeloma" AND ("IMROZ" OR "isatuximab" OR "BENEFIT" OR "IMROZ") AND newly diagnosed
PMID: 38828933
PMID: 38828951
multiple myeloma 2025 2026 treatment MajesTEC-9 teclistamab CARTITUDE-4 MIDAS MRD guided therapy APOLLO smoldering myeloma daratumumab
PMID: 40016302
PMID: 38830994
"multiple myeloma" AND "maintenance" AND ("lenalidomide" OR "ixazomib" OR "bortezomib")
Multiple Myeloma - Complete Treatment Note
All Trials: Landmark Through June 2026
1. TREATMENT FRAMEWORK OVERVIEW
- Transplant eligibility (transplant-eligible / transplant-ineligible)
- Disease stage (newly diagnosed / relapsed-refractory)
- Risk status (standard vs. high-risk cytogenetics)
Drug Classes in Use
| Class | Examples |
|---|---|
| Proteasome inhibitors (PI) | Bortezomib (V), Carfilzomib (K), Ixazomib (Ix) |
| Immunomodulatory drugs (IMiDs) | Thalidomide (T), Lenalidomide (R/Len), Pomalidomide (P) |
| Anti-CD38 monoclonal antibodies | Daratumumab (Dara/D), Isatuximab (Isa) |
| Anti-SLAMF7 antibody | Elotuzumab (Elo) |
| Anti-BCMA ADC | Belantamab mafodotin (Belamaf) |
| BCMA bispecific antibody | Teclistamab (Tec), Elranatamab |
| GPRC5D bispecific antibody | Talquetamab |
| BCMA CAR-T cells | Idecabtagene vicleucel (ide-cel), Ciltacabtagene autoleucel (cilta-cel) |
| Alkylators | Melphalan (M), Cyclophosphamide |
| Corticosteroids | Dexamethasone (d), Prednisone |
| Steroids + others | Venetoclax (for t(11;14)) |
2. SMOLDERING MULTIPLE MYELOMA (SMM)
Definition
High-risk SMM Definition (IMWG 2020)
Treatment of High-Risk SMM
- Phase 3 RCT; n=390; median follow-up 65.2 months
- Subcutaneous daratumumab monotherapy vs. active monitoring for 36 months (39 cycles)
- Primary endpoint: PFS (time to active myeloma or death)
| Outcome | Daratumumab | Active Monitoring | HR | P |
|---|---|---|---|---|
| 5-year PFS | 63.1% | 40.8% | 0.49 | <0.001 |
| 5-year OS | 93.0% | 86.9% | 0.52 | Significant |
| Deaths | 7.7% | 13.3% | - | - |
- Most common grade 3-4 AE: hypertension 5.7% vs 4.6%
- Impact: FDA approved SC daratumumab for high-risk SMM in November 2025 - first ever approved treatment for SMM
- Practice shift: Young patients with high-risk SMM can now be treated to delay/prevent active myeloma
3. NEWLY DIAGNOSED MULTIPLE MYELOMA (NDMM) - TRANSPLANT ELIGIBLE
3.1 INDUCTION (Pre-ASCT)
GRIFFIN Trial (Blood 2020) - Transplant Eligible, US
- Phase 2 RCT: D-VRd vs. VRd in transplant-eligible NDMM
- stringCR rate: 62% D-VRd vs. 27% VRd
- Established quadruplet as superior; paved way for Phase 3
CASSIOPEIA Trial (Moreau et al., Lancet 2019) - Transplant Eligible, European
- Phase 3 RCT: Dara-VTd (daratumumab + bortezomib + thalidomide + dexamethasone) vs. VTd
- sCR rate: 29% Dara-VTd vs. 20% VTd (P<0.0001)
- Established daratumumab quadruplet benefit in Europe
PERSEUS Trial (Sonneveld et al., NEJM 2024, PMID 38084760) ⭐ LANDMARK
- Phase 3 RCT; n=709 transplant-eligible NDMM
- Dara-VRd (induction + consolidation + lenalidomide maintenance) vs. VRd + lenalidomide maintenance
- Daratumumab SC throughout
| Outcome | D-VRd | VRd | HR | P |
|---|---|---|---|---|
| 48-month PFS | 84.3% | 67.7% | 0.42 | <0.001 |
| CR or better | 87.9% | 70.1% | - | <0.001 |
| MRD negative | 75.2% | 47.5% | - | <0.001 |
- Impact: D-VRd is NOW the preferred induction for transplant-eligible NDMM (NCCN 2024-2026)
GMMG-HD7 Trial (Mai et al., JCO 2025, PMID 39652594)
- Transplant-eligible NDMM: Isatuximab-VRd vs. VRd induction
- MRD negativity significantly improved with Isa-VRd
- Supports isatuximab quadruplet as European alternative
3.2 AUTOLOGOUS STEM CELL TRANSPLANTATION (ASCT)
- High-dose melphalan (MEL200, 200 mg/m²) + ASCT remains the consolidation standard for eligible patients
- ASCT continues to improve depth of response and PFS even in the CD38 antibody era
- Patient selection: Age typically ≤70 years, adequate organ function, ECOG 0-2
- IFM 2009 (Attal et al., NEJM 2017): ASCT superior to no ASCT even with VRd - ASCT still extends PFS
- MIDAS Trial (Perrot et al., NEJM July 2025, PMID 40459097): MRD-guided consolidation - MRD-negative patients can skip ASCT without loss of deep remission (see below)
MIDAS Trial - MRD-Guided Therapy (Perrot et al., NEJM 2025) ⭐ PARADIGM-SHIFTING
- Phase 3; n=718 transplant-eligible NDMM; induction = Isa-KRd
- After induction, stratified by MRD status:
- ASCT group: ASCT + 2 cycles Isa-KRd consolidation
- Isa-KRd group: 6 cycles Isa-KRd (no ASCT)
- MRD-negative at 10⁻⁶ pre-maintenance: 86% (ASCT) vs. 84% (Isa-KRd) — NOT significantly different (P=0.64)
-
Tandem ASCT vs. single ASCT + Isa-KRd
-
MRD-negative at 10⁻⁶ pre-maintenance: 32% vs. 40% — NOT significantly different (P=0.31)
-
Conclusion: MRD-negative patients after modern quadruplet induction can safely avoid ASCT without sacrificing remission depth — the first evidence that ASCT may become optional in MRD-guided strategies
-
Impact: Will fundamentally change how we approach ASCT selection in the future
3.3 POST-ASCT MAINTENANCE
- Lenalidomide 10 mg/day (days 1-21 of 28-day cycle) until progression
- Reduces relapse risk by ~50%; OS benefit demonstrated
- Bortezomib maintenance (for high-risk cytogenetics: del17p, t(4;14)): 1.3 mg/m² SC every 2 weeks
- Daratumumab maintenance post-ASCT: Under study (AURIGA trial - showing superior MRD negativity rates with Dara maintenance)
- Isatuximab maintenance: Being investigated
4. NEWLY DIAGNOSED MULTIPLE MYELOMA - TRANSPLANT INELIGIBLE
4.1 GOLD STANDARD: Daratumumab + Lenalidomide + Dexamethasone (D-Rd)
MAIA Trial (Facon et al., Lancet 2019 + NEJM 2021 + Leukemia 2025)
- Phase 3 RCT; n=737; transplant-ineligible NDMM
- D-Rd vs. Rd until progression
| Outcome | D-Rd | Rd | HR | P |
|---|---|---|---|---|
| Median PFS | 61.9 months | 34.4 months | 0.55 | <0.0001 |
| Median OS | Not reached | 65.5 months | 0.66 | 0.0003 |
| 60-month OS | 66.6% | 53.6% | - | - |
| CR or better | 51.1% | 30.1% | - | <0.0001 |
| MRD negativity | 32.1% | 11.1% | - | <0.0001 |
- Impact: D-Rd is the standard of care for transplant-ineligible NDMM; OS benefit confirmed at 5+ years
4.2 QUADRUPLET FOR TRANSPLANT-INELIGIBLE: D-VRd
CEPHEUS Trial (Usmani et al., Nat Med 2025, PMID 39910273)
- Phase 3 RCT; n=395; transplant-ineligible or transplant-deferred NDMM
- D-VRd (8 cycles) → D-Rd until progression vs. VRd (8 cycles) → Rd until progression
- Primary endpoint: MRD-negativity rate at 10⁻⁵
| Outcome | D-VRd | VRd | P |
|---|---|---|---|
| MRD negativity at 10⁻⁵ | 60.9% | 39.4% | <0.0001 |
| CR or better | 81.2% | 61.6% | <0.0001 |
| Sustained MRD negativity ≥12 months | 48.7% | 26.3% | <0.0001 |
| PFS (HR) | 43% lower risk | - | P=0.0005 |
- Conclusion: D-VRd is a new standard of care for transplant-ineligible/deferred NDMM
4.3 ISATUXIMAB-BASED QUADRUPLETS
IMROZ Trial (Facon et al., NEJM Oct 2024, PMID 38832972)
- Phase 3 RCT; n=446; transplant-ineligible NDMM (ages 18-80)
- Isa-VRd vs. VRd alone (3:2 randomization)
- Median follow-up 59.7 months (longest follow-up in any NDMM quadruplet trial)
| Outcome | Isa-VRd | VRd | HR | P |
|---|---|---|---|---|
| 60-month PFS | 63.2% | 45.2% | 0.60 | <0.001 |
| CR or better | 74.7% | 64.1% | - | 0.01 |
| MRD negative + CR | 55.5% | 40.9% | - | 0.003 |
- Impact: Longest-follow-up quadruplet trial; confirmed sustained PFS benefit at 5 years
BENEFIT Trial (Leleu et al., Nat Med 2024, PMID 38830994)
- Phase 3 RCT; n=270; transplant-ineligible NDMM (ages 65-79)
- Isa-VRd vs. Isa-Rd (adding bortezomib to isatuximab-Rd backbone)
- Primary endpoint: 18-month MRD negativity at 10⁻⁵
| Outcome | Isa-VRd | Isa-Rd | P |
|---|---|---|---|
| 18-month MRD neg (10⁻⁵) | 53% | 26% | <0.0001 |
| CR or better at 18 months | 58% | 33% | <0.0001 |
- Conclusion: Adding bortezomib to isatuximab-Rd (making Isa-VRd) significantly improves MRD outcomes even over Isa-Rd
5. RELAPSED/REFRACTORY MULTIPLE MYELOMA (RRMM)
5.1 FIRST RELAPSE (1-3 prior lines)
Standard Regimens at First Relapse
| Regimen | Indication | Key Trial |
|---|---|---|
| Dara-VRd or Dara-Rd | If not Dara-exposed frontline | - |
| KRd (carfilzomib + lenalidomide + dex) | Standard risk | ASPIRE trial |
| Dara-Rd or Dara-Vd | Dara-naive | CASTOR, POLLUX trials |
| Isa-Kd | Lenalidomide-refractory | IKEMA trial |
| Elotuzumab-Pd or KPd | Post-lenalidomide | ELOQUENT-3 |
5.2 CAR-T CELL THERAPY MOVING EARLIER
CARTITUDE-4 (San-Miguel et al., NEJM 2023, PMID 37272512) ⭐ LANDMARK
- Phase 3 RCT; n=419; lenalidomide-refractory NDMM (1-3 prior therapies)
- Cilta-cel (single infusion) vs. standard care (physician's choice: DPd or DVd)
| Outcome | Cilta-cel | Standard | HR | P |
|---|---|---|---|---|
| Median PFS | Not reached | 11.8 months | 0.26 | <0.001 |
| 12-month PFS | 75.9% | 48.6% | - | - |
| CR or better | 73.1% | 21.8% | - | - |
| MRD negative | 60.6% | 15.6% | - | - |
| CRS (any grade) | 76.1% (1.1% gr3-4) | - | - | - |
| Peripheral neuropathy | 2.8% | - | - | - |
| Cranial nerve palsy | 9.1% (unique to cilta-cel) | - | - | - |
- Impact: Cilta-cel FDA approved as early as second-line therapy in lenalidomide-refractory disease (April 2024)
- Update data (30-month PFS rate for those alive + progression-free at 1 year = 93%) - extraordinary durability
KarMMa-3 (Rodriguez-Otero et al., NEJM 2023, PMID 36762851)
- Phase 3 RCT; n=386; triple-class exposed RRMM (2-4 prior regimens, refractory to last line)
- Ide-cel (150-450 × 10⁶ CAR+ T cells) vs. 5 standard regimens
- 66% triple-class refractory; 95% daratumumab-refractory
| Outcome | Ide-cel | Standard | HR | P |
|---|---|---|---|---|
| Median PFS | 13.3 months | 4.4 months | 0.49 | <0.001 |
| Overall response | 71% | 42% | - | <0.001 |
| CR or better | 39% | 5% | - | - |
| CRS any grade | 88% (5% gr3+) | - | - | - |
| Neurotoxicity | 15% (3% gr3+) | - | - | - |
- Impact: Ide-cel FDA approved in triple-class exposed RRMM after 2-4 prior lines
5.3 BISPECIFIC ANTIBODIES
MajesTEC-3 Trial (Costa et al., NEJM 2026, PMID 41363801) ⭐ NEWEST LANDMARK - NEJM Feb 2026
- Phase 3 RCT; n=587; RRMM with 1-3 prior lines
- Teclistamab (anti-BCMA × anti-CD3) + Daratumumab vs. DPd or DVd (standard)
| Outcome | Tec-Dara | DPd/DVd | HR | P |
|---|---|---|---|---|
| 36-month PFS | 83.4% | 29.7% | 0.17 | <0.001 |
| CR or better | 81.8% | 32.1% | - | <0.001 |
| MRD negative (10⁻⁵) | 58.4% | 17.1% | - | <0.001 |
| Overall response | 89.0% | 75.3% | - | <0.001 |
| Serious AEs | 70.7% | 62.4% | - | - |
| Death from AEs | 7.1% | 5.9% | - | - |
- The most remarkable PFS data seen in early relapsed myeloma: 83% at 3 years vs. 30% standard
- "This is as good as any treatment we have seen in myeloma" - Dr. Luciano Costa, ASH 2025
- Presented ASH December 2025; Published NEJM February 2026; ASCO 2026
- FDA approval imminent / under review 2026
- Requires step-up dosing to mitigate CRS; ongoing infection risk due to immunosuppression
MajesTEC-9 Trial (ASCO 2026, published NEJM)
- Phase 3 RCT; n=593; RRMM at first relapse
- Teclistamab monotherapy vs. PVd or Kd (standard)
- Significant improvement in PFS, OS, MRD negativity
- Established teclistamab monotherapy as a new standard in first relapse (anti-CD38 + lenalidomide refractory population)
Other Approved Bispecifics:
- Elranatamab (BCMA × CD3): FDA approved 2023 in ≥4 prior lines; phase 3 ongoing
- Talquetamab (GPRC5D × CD3): FDA approved 2023; unique target (no overlap with BCMA)
5.4 BELANTAMAB MAFODOTIN (BELAMAF) - ANTI-BCMA ADC
DREAMM-7 (Hungria et al., NEJM 2024, PMID 38828933)
- Phase 3 RCT; n=494; RRMM after ≥1 prior line
- BVd (belantamab + bortezomib + dex) vs. DVd (daratumumab + bortezomib + dex)
| Outcome | BVd | DVd | HR | P |
|---|---|---|---|---|
| Median PFS | 36.6 months | 13.4 months | 0.41 | <0.001 |
| 18-month OS | 84% | 73% | - | - |
| CR + MRD negative | 25% | 10% | - | - |
| Ocular events | 79% | 29% | - | - |
| Grade 3-4 AEs | 95% | 78% | - | - |
- Ocular toxicity (keratopathy) is the key limiting toxicity; managed with dose modifications and ophthalmic monitoring
- BVd superior to DVd - but ocular toxicity requires specialist ophthalmology co-management
DREAMM-8 (Dimopoulos et al., NEJM 2024, PMID 38828951)
- Phase 3 RCT; n=302; lenalidomide-exposed RRMM
- BPd (belantamab + pomalidomide + dex) vs. PVd
| Outcome | BPd | PVd | HR | P |
|---|---|---|---|---|
| 12-month PFS | 71% | 51% | 0.52 | <0.001 |
| CR or better | 40% | 16% | - | - |
| Ocular events | 89% (43% gr3-4) | 30% | - | - |
- Belamaf was previously withdrawn but DREAMM-7 & 8 results led to FDA re-approval in 2024
6. TRIPLE-CLASS/HEAVILY PRETREATED RRMM (≥3-4 prior lines)
Standard Approved Options
| Regimen | Key Data |
|---|---|
| Teclistamab (Tecvayli) | MajesTEC-1: ORR 63%, sCR 39% in penta-refractory patients |
| Elranatamab (Elrexfio) | MAGNETISMM-3: ORR 61% in BCMA-naive, ≥4 prior lines |
| Talquetamab (Talvey) | MonumenTAL-1: ORR 73% (GPRC5D target; useful after BCMA failure) |
| Ide-cel (Abecma) | KarMMa-3: After 2-4 lines |
| Cilta-cel (Carvykti) | CARTITUDE-1/4: 2+ lines lenalidomide-refractory |
| Belantamab mafodotin | DREAMM-7/8: 2+ lines |
| Selinexor + dexamethasone | STORM trial: penta-refractory; XPO1 inhibitor |
| Isatuximab + Pd | ICARIA-MM; carfilzomib-based in lenalidomide-refractory |
| Venetoclax + bortezomib + dex | t(11;14) myeloma ONLY (BCL-2 high) |
| Panobinostat + bortezomib + dex | PANORAMA-1; HDAC inhibitor; penta-refractory |
CAR-T vs. Bispecific Antibody: 2026 Sequencing
| Feature | CAR-T (Cilta-cel/Ide-cel) | Bispecific (Tec/Elra/Tal) |
|---|---|---|
| Availability | Center-dependent; manufacturing 4-8 weeks | Off-the-shelf; immediate |
| Administration | Single infusion | Ongoing weekly/biweekly infusions |
| Efficacy | Potentially higher CR rates; longer PFS | Slightly lower but rapid response |
| CRS | 75-90% (mostly grade 1-2) | 50-70% (mostly grade 1-2) |
| Neurotoxicity | ICANS + cilta-cel specific (cranial nerve, movement) | Less severe |
| Infection | Prolonged immunosuppression post-CAR-T | Ongoing during treatment |
| Cost | Higher per course | Lower upfront, accumulates with duration |
| Preference | When cure is the goal; younger patients with access | Patients needing immediate treatment; elderly |
7. COMPLETE TRIAL TIMELINE - LANDMARK TO LATEST
ERA 1: Chemotherapy Foundation (1962-1996)
| Year | Trial/Drug | Key Finding |
|---|---|---|
| 1962 | Melphalan + prednisone (MP) | First effective myeloma therapy |
| 1986 | VAD (vincristine/doxorubicin/dex) | Faster response; pre-ASCT |
| 1996 | First ASCT trials | ASCT doubles PFS vs. conventional chemo |
ERA 2: IMiDs and Novel Agents (2003-2010)
| Trial | Year | Regimen | Result | Impact |
|---|---|---|---|---|
| APEX | 2005 | Bortezomib (V) vs. dex | ORR 43% vs. 18%; OS benefit | First PI approved |
| IFM/HOVON | 2005 | Thalidomide maintenance | PFS benefit post-ASCT | Maintenance concept established |
| VISTA | 2008 | VMP vs. MP | 35% OS improvement | First-line PI without ASCT |
| MM-009/010 | 2006-7 | Lenalidomide + dex vs. dex | ORR 60% vs. 20% in RRMM | Lenalidomide approved |
ERA 3: Triplets and Maintenance (2010-2017)
| Trial | Year | Regimen | Result | Impact |
|---|---|---|---|---|
| ELOQUENT-2 | 2015 | Elo-Rd vs. Rd (RRMM) | PFS benefit | Anti-SLAMF7 approved |
| SWOG S0777 | 2017 | VRd vs. Rd (NDMM) | 45 vs 43% sCR; PFS & OS improved | VRd became standard NDMM |
| ASPIRE | 2015 | KRd vs. Rd (1st relapse) | Median PFS 26 vs. 17 months | Carfilzomib triplet approved |
| POLLUX | 2016 | Dara-Rd vs. Rd (RRMM) | HR 0.37 PFS | Daratumumab + Rd approved |
| CASTOR | 2016 | Dara-Vd vs. Vd (RRMM) | HR 0.39 PFS | Daratumumab + Vd approved |
| IKEMA | 2021 | Isa-Kd vs. Kd (1-3 prior lines) | HR 0.53 PFS | Isatuximab + Kd approved |
| IFM 2009 | 2017 | ASCT vs. no ASCT (VRd era) | ASCT still extends PFS | ASCT remains standard |
| Maintenance trials | 2012 | Lenalidomide post-ASCT | OS benefit | Len maintenance standard |
ERA 4: Anti-CD38 Quadruplets and Frontline Transformation (2019-2024)
| Trial | Year | Regimen | Result | Impact |
|---|---|---|---|---|
| MAIA | 2019/2025 | D-Rd vs. Rd (TI NDMM) | Median PFS 61.9 vs. 34.4 mo; OS benefit | D-Rd standard for TI-NDMM |
| CASSIOPEIA | 2019 | Dara-VTd vs. VTd (TE NDMM) | sCR 29% vs 20% | European quadruplet established |
| GRIFFIN | 2020 | D-VRd vs. VRd (TE NDMM) | CR 62% vs 27% | Foundation for PERSEUS |
| ANDROMEDA | 2021 | Dara-VCd vs. VCd (AL amyloid) | - | Anti-CD38 in AL amyloid |
| KarMMa-3 | 2023 | Ide-cel vs. standard (2-4 lines) | PFS 13.3 vs. 4.4 months | Ide-cel Phase 3 approved |
| CARTITUDE-4 | 2023 | Cilta-cel vs. standard (1-3 lines) | HR 0.26; 12-mo PFS 76% vs. 49% | Cilta-cel earlier lines |
| IMROZ | 2024 | Isa-VRd vs. VRd (TI NDMM) | 5-yr PFS 63% vs. 45% | 5-year quadruplet data |
| PERSEUS | 2024 | D-VRd vs. VRd (TE NDMM) | 4-yr PFS 84% vs. 68% | D-VRd standard TE-NDMM |
| DREAMM-7 | 2024 | BVd vs. DVd | Median PFS 36.6 vs. 13.4 months | Belamaf re-approved |
| DREAMM-8 | 2024 | BPd vs. PVd (len-exposed) | 12-mo PFS 71% vs. 51% | ADC in len-refractory |
| BENEFIT | 2024 | Isa-VRd vs. Isa-Rd (TI) | MRD neg 53% vs. 26% | Quadruplet > triplet even with Isa |
ERA 5: Immunotherapy Revolution and MRD-Guided Therapy (2025-2026)
| Trial | Year | Regimen | Result | Impact |
|---|---|---|---|---|
| CEPHEUS | 2025 | D-VRd vs. VRd (TI/deferred) | MRD neg 61% vs. 39%; HR 0.57 | D-VRd now standard for TI/deferred |
| MAIA long-term | 2025 | D-Rd vs. Rd (5-year update) | OS HR 0.66; median OS not reached | Confirms D-Rd OS benefit at 5 years |
| AQUILA | 2025 | Daratumumab vs. monitoring (high-risk SMM) | 5-yr PFS 63% vs. 41%; OS benefit | First FDA-approved therapy for SMM (Nov 2025) |
| MIDAS | 2025 | MRD-guided ASCT vs. no ASCT | MRD-neg patients: ASCT = no ASCT | ASCT may be skippable in MRD-neg after quadruplet induction |
| MajesTEC-3 | 2025/2026 | Tec + Dara vs. DPd/DVd (1-3 lines) | 3-yr PFS 83% vs. 30%; HR 0.17 | Bispecific + CD38 antibody redefines 2nd-line RRMM |
| MajesTEC-9 | 2026 | Teclistamab vs. PVd/Kd (1st relapse) | PFS, OS both superior | Teclistamab monotherapy at first relapse |
8. DRUG DOSING QUICK REFERENCE
Frontline (Transplant-Eligible) - D-VRd (PERSEUS)
| Drug | Dose | Schedule |
|---|---|---|
| Daratumumab SC | 1800 mg SC | Wkly × 8, q2w × 8, then q4w |
| Bortezomib | 1.3 mg/m² SC | Days 1, 8, 15 q21d |
| Lenalidomide | 25 mg PO | Days 1-14 q21d |
| Dexamethasone | 40 mg PO/IV | Days 1, 8, 15, 22 |
Frontline (Transplant-Ineligible) - D-Rd (MAIA)
| Drug | Dose | Schedule |
|---|---|---|
| Daratumumab SC | 1800 mg SC | Wkly × 8, q2w × 16 wks, then q4w |
| Lenalidomide | 25 mg PO (days 1-21) | 28-day cycle |
| Dexamethasone | 40 mg PO | Days 1, 8, 15, 22 |
Relapsed - Teclistamab (Step-up dosing)
| Step | Dose | Day |
|---|---|---|
| Step 1 (priming) | 0.06 mg/kg SC | Day 1 |
| Step 2 | 0.3 mg/kg SC | Day 4 |
| Step 3 (full dose) | 1.5 mg/kg SC | Day 7, then weekly |
9. MAINTENANCE THERAPY SUMMARY
| Setting | Preferred Maintenance | Duration | Evidence |
|---|---|---|---|
| Post-ASCT, standard risk | Lenalidomide 10 mg/day | Until progression | Multiple RCTs |
| Post-ASCT, high-risk (del17p, t(4;14)) | Lenalidomide + bortezomib OR bortezomib alone | 2 years bortezomib | IFM/DFCI data |
| Transplant-ineligible | Lenalidomide (within D-Rd) | Until progression | MAIA |
| Post-D-VRd induction | Lenalidomide ± daratumumab | Until progression | PERSEUS; AURIGA |
| MRD-negative post-quadruplet | Lenalidomide maintenance (ASCT optional) | MIDAS supports this | NEJM 2025 |
10. HIGH-RISK MYELOMA: SPECIAL CONSIDERATIONS
| Principle | Approach |
|---|---|
| Quadruplet induction mandatory | D-VRd or Isa-VRd (add PI to overcome high-risk) |
| ASCT (if eligible) | Still recommended even in MRD-negative (MIDAS subgroup analysis) |
| Bortezomib-based maintenance | Add bortezomib to lenalidomide for del17p |
| Venetoclax | ONLY for t(11;14) (BCL-2 overexpression); BELLINI/CANOVA data |
| CAR-T early | Consider earlier lines than standard-risk |
| Tandem ASCT | Some data for del17p; being replaced by immunotherapy combinations |
11. SUMMARY TABLE - STANDARD OF CARE BY SETTING (2026)
| Setting | Preferred Regimen | Evidence Base |
|---|---|---|
| High-risk smoldering MM | Subcutaneous daratumumab × 36 months | AQUILA (NEJM 2025) - FDA approved Nov 2025 |
| NDMM, transplant-eligible (induction) | D-VRd (dara + VRd) × 4-6 cycles | PERSEUS (NEJM 2024) |
| NDMM, transplant-eligible (consolidation) | High-dose melphalan + ASCT (or Isa-KRd if MRD-negative) | IFM 2009; MIDAS (NEJM 2025) |
| NDMM, transplant-eligible (maintenance) | Lenalidomide ± daratumumab | CALGB; AURIGA |
| NDMM, transplant-ineligible (fit) | D-VRd → D-Rd maintenance | CEPHEUS (Nat Med 2025) |
| NDMM, transplant-ineligible (frail) | D-Rd | MAIA |
| RRMM, 1st relapse (len-refractory) | Cilta-cel OR Teclistamab + Dara | CARTITUDE-4; MajesTEC-3 (NEJM 2026) |
| RRMM, 1st relapse (Dara-naive) | Isa-Kd, or KRd, or Dara-based triplet | IKEMA, ASPIRE |
| RRMM, 2-4 prior lines | Ide-cel, Cilta-cel, Teclistamab, Elranatamab | KarMMa-3, CARTITUDE-4, MajesTEC-1 |
| Penta-refractory RRMM | Talquetamab, CAR-T, Selinexor, Venetoclax (t(11;14)) | MonumenTAL-1, STORM |
| t(11;14) myeloma | Venetoclax-based combinations | CANOVA trial |
REFERENCES
- Goldman-Cecil Medicine, Chapter on Multiple Myeloma (GRIFFIN, MAIA, CASSIOPEIA references)
- Sonneveld P et al., NEJM 2024 - PERSEUS trial D-VRd TE-NDMM (PMID 38084760)
- Facon T et al., NEJM 2024 - IMROZ trial Isa-VRd TI-NDMM (PMID 38832972)
- Facon T et al., Leukemia 2025 - MAIA 5-year update (PMID 40016302)
- Usmani SZ et al., Nat Med 2025 - CEPHEUS trial D-VRd TI/deferred NDMM (PMID 39910273)
- Leleu X et al., Nat Med 2024 - BENEFIT trial Isa-VRd vs Isa-Rd (PMID 38830994)
- San-Miguel J et al., NEJM 2023 - CARTITUDE-4 cilta-cel (PMID 37272512)
- Rodriguez-Otero P et al., NEJM 2023 - KarMMa-3 ide-cel (PMID 36762851)
- Costa LJ et al., NEJM 2026 - MajesTEC-3 teclistamab + dara (PMID 41363801)
- Hungria V et al., NEJM 2024 - DREAMM-7 BVd vs DVd (PMID 38828933)
- Dimopoulos MA et al., NEJM 2024 - DREAMM-8 BPd vs PVd (PMID 38828951)
- Dimopoulos MA et al., NEJM 2025 - AQUILA daratumumab in SMM (PMID 39652675)
- Perrot A et al., NEJM 2025 - MIDAS MRD-guided therapy (PMID 40459097)
- MajesTEC-9 Phase 3 trial - ASCO 2026 / NEJM 2026 (teclistamab vs PVd/Kd at first relapse)
All the things from introduction classification clinical features and diagnosis of multiple myeloma
Multiple Myeloma - Introduction, Classification, Clinical Features & Diagnosis
1. INTRODUCTION AND DEFINITION
- Clonal bone marrow plasma cells ≥10% (or biopsy-proven plasmacytoma)
- M-protein in serum or urine (except in non-secretory myeloma)
- At least one myeloma-defining event (MDE) - either CRAB criteria or SLiM biomarkers
- Goldman-Cecil Medicine, Chapter 173
2. EPIDEMIOLOGY
-
Annual incidence: ~4 per 100,000 in the US; approximately 35,000 new cases/year
-
Peak age of onset: 65-70 years; median age at diagnosis ~70 years
-
Male predominance (M:F ~1.4:1)
-
Higher incidence in people of African descent - approximately 2× the incidence seen in Whites; also earlier age of onset
-
MGUS prevalence by age (Mayo Clinic data):
- Age 50-59: 1.2% (total population)
- Age 70-79: 3.4%
- Age 80+: 4.6%
- African-Americans have significantly higher MGUS prevalence at all ages
-
Robbins Pathology (Cotran), Chapter 13; Goldman-Cecil Medicine, p.1977
3. THE PLASMA CELL DYSCRASIA SPECTRUM (CLASSIFICATION)
Normal Plasma Cells → MGUS → Smoldering MM → Active MM → Plasma Cell Leukemia
3.1 Full Classification Table (IMWG Diagnostic Criteria)
| Disorder | Diagnostic Criteria |
|---|---|
| Non-IgM MGUS | M-protein <3 g/dL AND bone marrow plasma cells <10% AND NO CRAB/SLiM criteria |
| IgM MGUS | IgM <3 g/dL AND BM lymphoplasmacytic infiltration <10% AND NO symptoms |
| Light chain MGUS | Abnormal FLC ratio (<0.26 or >1.65) AND increased involved light chain AND no heavy chain expression AND no end-organ damage |
| Smoldering MM (SMM) | Both: (1) M-protein ≥3 g/dL, OR urine M-protein ≥500 mg/24h, OR BMPC 10-60%; AND (2) No myeloma-defining events |
| Active Multiple Myeloma | Clonal BMPC ≥10% AND at least one myeloma-defining event (CRAB or SLiM) |
| Solitary Plasmacytoma | Single biopsy-proven clonal plasma cell tumor (bone or soft tissue) with BMPC <10% |
| Plasma Cell Leukemia | >20% plasma cells in peripheral blood OR >2000 plasma cells/µL |
| AL Amyloidosis | Clonal plasma cells secreting light chains that deposit as amyloid fibrils |
- Goldman-Cecil Medicine, Table 173-2
3.2 Myeloma-Defining Events (MDE)
- C - hyperCalcemia: serum calcium >2.75 mmol/L (>11 mg/dL) OR >1 mg/dL above upper limit of normal
- R - Renal insufficiency: creatinine >177 µmol/L (>2 mg/dL) OR creatinine clearance <40 mL/min
- A - Anemia: Hgb <100 g/L (10 g/dL) OR >20 g/L below normal
- B - Bone lesions: one or more osteolytic lesions on skeletal survey, CT, or PET/CT
- SiXty percent: clonal bone marrow plasma cells ≥60%
- Light chain ratio: involved/uninvolved sFLC ratio ≥100
- MRI: >1 focal marrow lesion ≥5 mm on MRI
3.3 WHO/ICC 2022 Cytogenetic-Based Classification
- MM with CCND family translocation - t(11;14) and t(6;14) - cyclin D1/D3
- MM with NSD2 translocation - t(4;14) - NSD2/FGFR3
- MM with MAF family translocation - t(14;16) and t(14;20)
- MM with hyperdiploidy - trisomies of odd chromosomes (3, 5, 7, 9, 11, 15, 19, 21)
- MM, NOS
- Quick Compendium of Clinical Pathology, section 4.3.7.3
4. PATHOGENESIS
4.1 Cell of Origin
4.2 Oncogenesis: Two Pathways
-
IgH translocations (~40%): Chromosomal translocations involving the IgH locus (14q32) juxtaposing oncogenes near the IgH enhancer. Key partners:
- t(11;14): cyclin D1 - most common; standard-risk
- t(4;14): NSD2/FGFR3 - high-risk
- t(14;16): c-MAF - high-risk
- t(14;20): MAFB - high-risk
- t(6;14): cyclin D3 - standard-risk
-
Hyperdiploidy (~40%): Trisomies of odd-numbered chromosomes; generally standard-risk; associated with lower IgH translocation frequency
-
Both (~15%); Other (~5%)
- RAS mutations (KRAS, NRAS) - most common acquired mutation
- MYC rearrangements - associated with aggressive/extramedullary disease
- del(17p) - TP53 deletion; high-risk; associated with poor prognosis
- del(1p) - CDKN2C
- amp(1q) - CKS1B; high-risk; adverse outcome
4.3 Role of the Bone Marrow Microenvironment
- IL-6 (most important growth/survival cytokine): produced by tumor cells AND marrow stromal cells; high IL-6 = poor prognosis
- VEGF: promotes angiogenesis in marrow
- Direct stromal contact: VLA-4 integrin on myeloma cells binds VCAM-1 on stromal cells → NF-κB activation → survival
- NF-κB pathway: Frequently mutated in myeloma; promotes anti-apoptotic signals (Bcl-2, Bcl-XL)
4.4 Bone Disease Mechanism
- ↑ RANKL (receptor activator of NF-κB ligand) on osteoblasts and possibly plasma cells
- ↓ Osteoprotegerin (OPG) - RANKL decoy receptor
- ↑ MIP-1α (CCL3) - chemokine augmenting osteoclast formation
- ↑ IL-1β, IL-6, IL-3
- ↑ DKK1 (Dickkopf-1) - Wnt pathway inhibitor
- ↑ IL-3, IL-7
- Goldman-Cecil Medicine, p.1977-1978; Robbins & Cotran Pathology, p.568-569
5. MORPHOLOGY AND HISTOPATHOLOGY
5.1 Bone Marrow Aspirate
- Eccentric nucleus (clock-face/cartwheel chromatin)
- Perinuclear clearing (Hof) due to prominent Golgi apparatus
- Basophilic cytoplasm (high RNA content for Ig synthesis)
- Plasmablasts: large, vesicular nucleus, prominent single nucleolus - aggressive
- Flame cells: fiery red cytoplasm
- Mott cells: multiple grapelike cytoplasmic droplets (Russell bodies)
- Russell bodies: cytoplasmic globular inclusions of precipitated Ig
- Dutcher bodies: intranuclear Ig inclusions
- Multinucleated forms: bizarre giant plasma cells
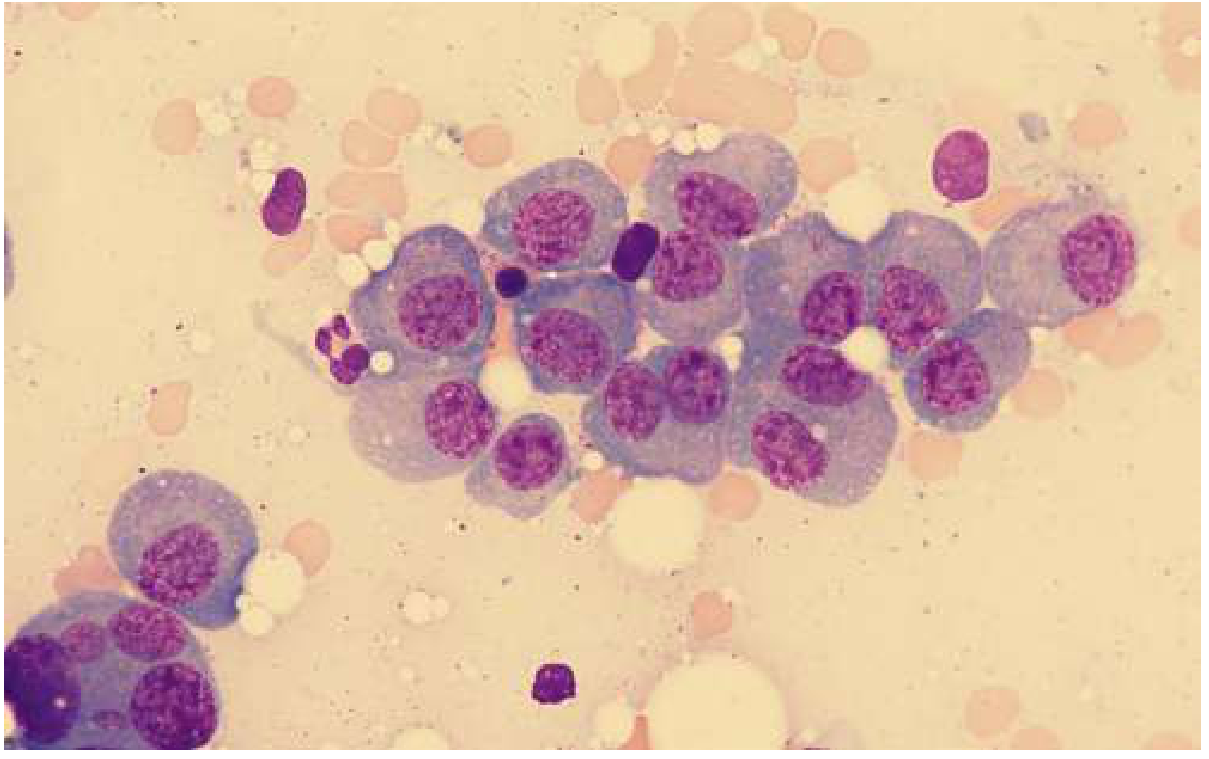
5.2 Plasma Cell Percentage
- In 96% of myeloma, clonal plasma cells are ≥10% of nucleated BM cells
- In 4%, BM plasma cells may be <10% even with frank myeloma (focal disease) - repeat biopsy or lesion biopsy may be needed
- Diagnosis requires ≥10% clonal plasma cells, not just >10% plasma cells (exclude reactive plasmacytosis)
5.3 Bone Disease - Radiological Appearance
- Robbins & Cotran Pathology, p.569-570
6. CLINICAL FEATURES
6.1 Presenting Symptoms
- Bone pain in back or chest at diagnosis: >66% of patients
- Pathologic fractures (especially vertebral compression fractures)
- Height loss of several inches due to vertebral collapse
- Cord compression in up to 10% (thoracic > lumbosacral > cervical)
- Present in >70% at diagnosis
- Normocytic, normochromic
- Mechanism: marrow replacement by plasma cells, renal failure, direct inhibition of erythropoiesis by myeloma cytokines
- Presents as: weakness, fatigue, exertional dyspnea
- Renal insufficiency (creatinine >2 mg/dL) in ~20% at diagnosis
- Main mechanisms:
- Light chain cast nephropathy (myeloma kidney) - most common: free light chains precipitate in distal/collecting tubules forming large waxy laminated casts; severity correlates with urinary light chain load
- Hypercalcemia - leads to vasoconstriction, nephrogenic diabetes insipidus, reduced GFR
- AL amyloidosis (~10%): nephrotic syndrome + renal failure
- Light chain deposition disease: diffuse glomerular and tubular deposition
- Fanconi syndrome: proximal tubular dysfunction → glycosuria, phosphaturia, aminoaciduria
- Monoclonal gammopathy-associated proliferative GN
- Present in 15-20% at diagnosis
- Source: osteoclast-mediated bone destruction
- Symptoms: confusion, weakness, lethargy, constipation, polyuria, nausea, polydipsia ("stones, bones, groans, thrones, and psychiatric overtones")
- Recurrent bacterial infections (encapsulated organisms: Streptococcus pneumoniae, H. influenzae, Klebsiella)
- Mechanism: immunoparesis - suppression of normal immunoglobulin synthesis, neutropenia from marrow infiltration, impaired antibody responses
- Leading cause of death in myeloma (along with renal failure)
- Radiculopathy (thoracic > lumbosacral): most common neurological complication; vertebral collapse or plasmacytoma compressing nerve roots
- Spinal cord compression: emergency; occurs in ~10%
- Peripheral neuropathy: usually from AL amyloidosis; rarely direct myeloma neuropathy; also from bortezomib (treatment-related)
- Intracranial plasmacytomas: extensions of skull lesions
- CNS involvement: rare; very poor prognosis
- Hypercalcemia-related encephalopathy: confusion, lethargy, coma
- Visual disturbances (fundal changes: "sausage-link" retinal veins)
- Neurological symptoms
- Bleeding tendency
- Increased risk of deep vein thrombosis (especially with lenalidomide or thalidomide treatment)
- Occasionally: acquired factor inhibitors, platelet dysfunction from M-protein coating
- Hepatic infiltration
- Pleural effusions, ascites
- Multiple extramedullary plasmacytomas - sign of aggressive biology
- Plasma cell leukemia: >2×10⁹/L plasma cells in peripheral blood; very poor prognosis
6.2 Physical Examination Findings
| Finding | Frequency | Comment |
|---|---|---|
| Pallor | Most frequent | From anemia |
| Bone tenderness | Common | Vertebral, rib tenderness on palpation |
| Palpable liver | ~5% | Advanced/extramedullary disease |
| Palpable spleen | ~1% | Rare |
| Radiculopathy signs | Variable | Cord compression until proven otherwise |
| Peripheral neuropathy | Less common | Usually amyloid-related |
| Purpura | Occasionally | Hyperviscosity or platelet dysfunction |
-
Rouleaux formation: red blood cells stacked in linear arrays like coins - due to high immunoglobulin levels coating RBCs; characteristic but not specific (also seen in SLE, early HIV)
-
Normocytic normochromic anemia
-
Rarely: circulating plasma cells (plasma cell leukemia)
-
Goldman-Cecil Medicine, p.1979-1980; Robbins & Cotran Pathology, p.570
7. LABORATORY INVESTIGATION
7.1 Workup at Diagnosis
| Test | Purpose | Findings |
|---|---|---|
| CBC with differential | Anemia, cytopenia | Normocytic normochromic anemia; thrombocytopenia (marrow failure) |
| Peripheral blood smear | Morphology | Rouleaux formation; occasional circulating plasma cells |
| Serum chemistry (BMP) | CRAB criteria | ↑Creatinine, ↑Calcium, ↑Uric acid |
| Serum LDH | Staging (R-ISS) | ↑ in aggressive disease |
| Serum albumin | Staging (ISS) | Often ↓ |
| Serum β2-microglobulin (β2M) | Staging | ↑ correlates with tumor burden |
| Serum protein electrophoresis (SPEP) | M-protein detection | M-spike (monoclonal band) in ~80% of myeloma |
| Serum immunofixation electrophoresis (IFE) | Characterize M-protein | More sensitive than SPEP; determines heavy chain isotype (IgG, IgA, IgD, IgE) and light chain type (κ or λ) |
| Serum free light chains (sFLC) | Diagnosis + monitoring | κ/λ ratio normally 0.26-1.65; ratio >100 = SLiM criterion; essential for light-chain-only MM and nonsecretory MM |
| Test | Purpose |
|---|---|
| 24-hour urine protein electrophoresis (UPEP) | Detects Bence Jones protein (free light chains in urine) |
| Urine immunofixation | Characterizes urinary M-protein type |
| Test | Purpose |
|---|---|
| Bone marrow aspiration + biopsy (iliac crest) | Morphology, % plasma cells, clonality |
| Immunohistochemistry (IHC) | CD138, CD38, κ/λ restriction |
| Flow cytometry | CD38+, CD138+, CD45-, CD56+, CD19-; κ or λ restricted |
| Cytogenetics/FISH | Risk stratification (del17p, t(4;14), t(14;16), t(11;14), gain1q) |
| Modality | Role |
|---|---|
| Low-dose whole-body CT | Preferred for detecting lytic lesions (replaced skeletal survey) |
| PET/CT | Best for metabolically active disease; monitors treatment response; detects extramedullary disease |
| MRI (whole-body or spine) | Superior for BM infiltration pattern; spinal cord involvement; SMM/plasmacytoma workup |
| Skeletal survey (plain films) | Now largely replaced; historical standard |
| Bone scan (technetium) | NOT recommended - myeloma lesions are cold (purely lytic, no reactive new bone) |
7.2 Protein Electrophoresis Explained
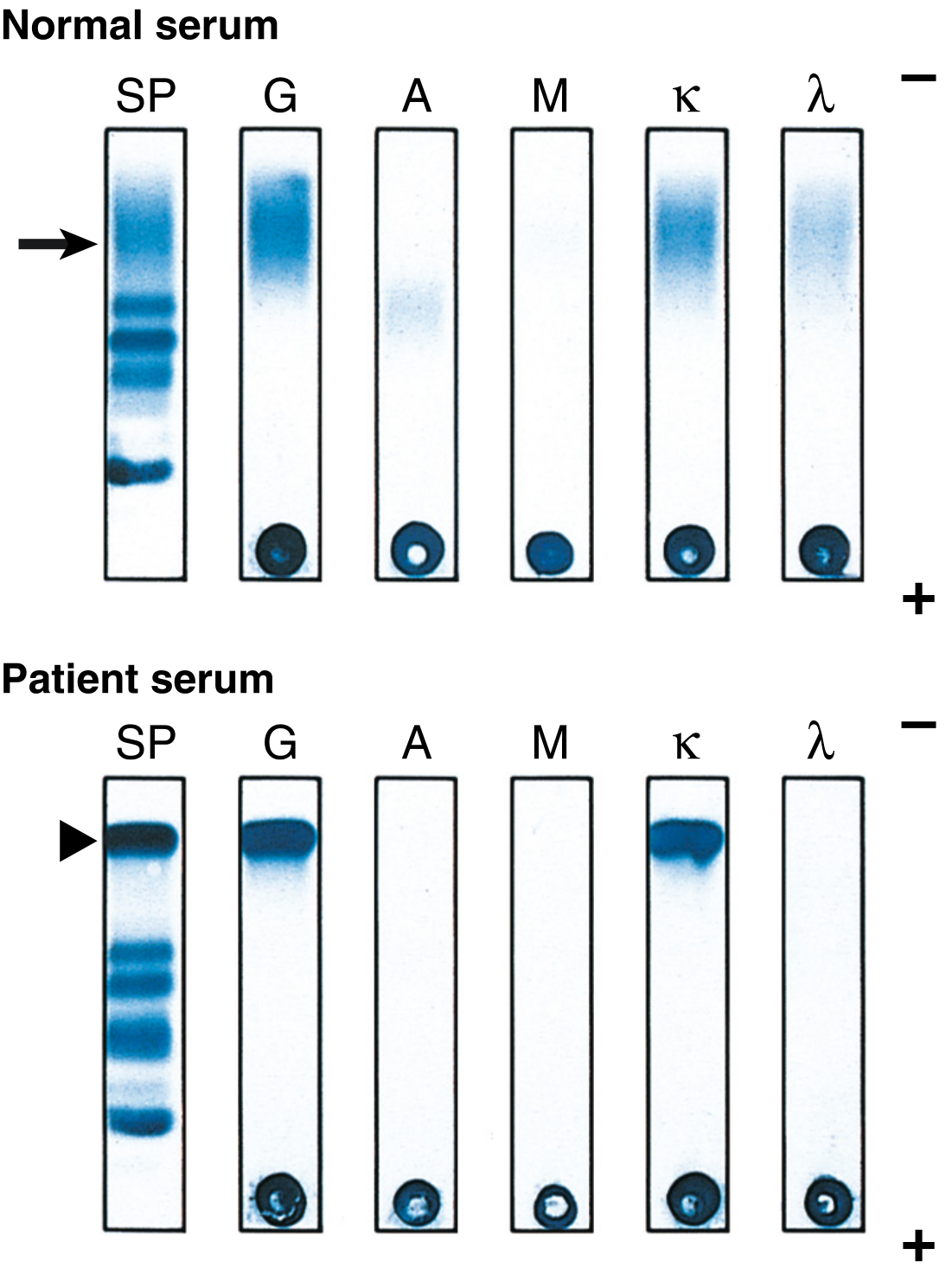
- Adding SPEP + serum IFE + serum FLC detects M-protein in nearly all cases of MM
- ~80% detected on SPEP alone
- ~2% of cases are non-secretory myeloma (no M-protein on SPEP/IFE/sFLC) - diagnosis by BM biopsy only
7.3 Immunophenotype by Flow Cytometry
- CD138+ (syndecan-1) - most specific marker
- CD38+ (strong) - the target for daratumumab and isatuximab
- CD45- (negative; distinguishes from normal plasma cells which are CD45+)
- CD56+ (aberrant expression; not on normal plasma cells)
- CD19- (negative; normal plasma cells are CD19-dim, myeloma cells CD19 absent)
- CD20+ in only ~20%
- Light chain restricted: either κ+ or λ+
-
4:1 → clonal κ population
- <1:2 → clonal λ population
7.4 Imaging in Multiple Myeloma
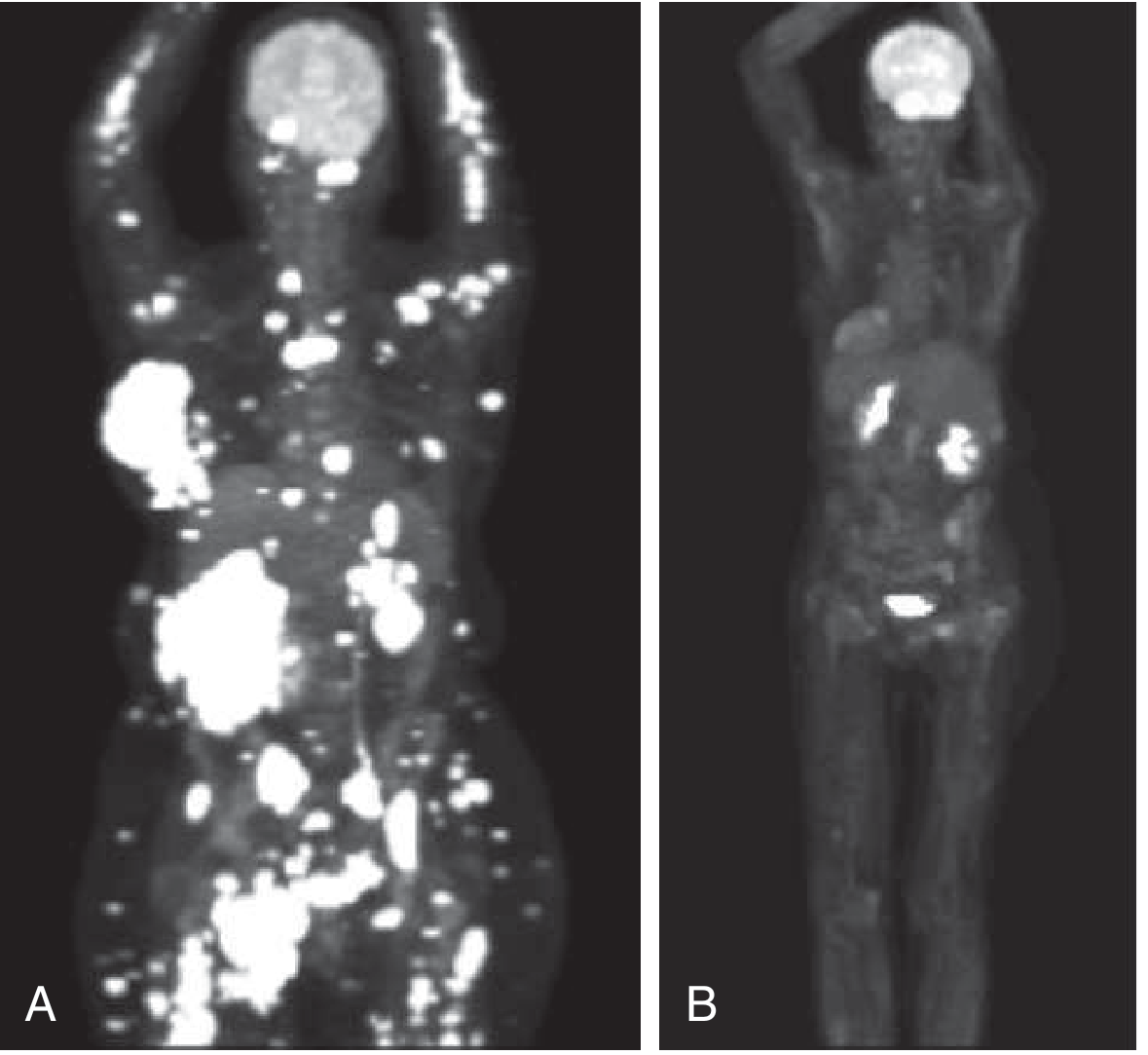
- Goldman-Cecil Medicine, p.1978-1979
8. STAGING
8.1 International Staging System (ISS) - Original
| Stage | Criteria | Median OS |
|---|---|---|
| I | β2M <3.5 mg/L AND Albumin ≥3.5 g/dL | 62 months |
| II | Neither Stage I nor Stage III | 44 months |
| III | β2M ≥5.5 mg/L | 29 months |
8.2 Revised ISS (R-ISS) - Current Standard
| Stage | Criteria | 5-year OS |
|---|---|---|
| R-ISS I | ISS Stage I AND normal LDH AND no high-risk cytogenetics | 82% |
| R-ISS II | Neither R-ISS I nor R-ISS III | 62% |
| R-ISS III | ISS Stage III AND (high-risk cytogenetics OR elevated LDH) | 40% |
- Goldman-Cecil Medicine, Table 173-4
8.3 Cytogenetic Risk Stratification
| Risk Category | Cytogenetic Abnormalities | Implication |
|---|---|---|
| High-risk | t(4;14), t(14;16), t(14;20), del(17p), amp(1q), del(1p), p53 mutation, plasmablastic morphology | Shortened PFS/OS; requires intensive quadruplet therapy; bortezomib maintenance |
| Standard-risk | t(11;14), t(6;14), hyperdiploidy (trisomies) | Better prognosis; typical treatment algorithms |
9. DIAGNOSTIC CRITERIA SUMMARY (IMWG 2014)
| MDE Type | Definition |
|---|---|
| CRAB - Hypercalcemia | Serum Ca >11 mg/dL OR >1 mg/dL above ULN |
| CRAB - Renal | Creatinine >2 mg/dL OR CrCl <40 mL/min (attributable to myeloma) |
| CRAB - Anemia | Hgb <10 g/dL OR >2 g/dL below normal |
| CRAB - Bone | ≥1 osteolytic lesion on imaging |
| SLiM - 60% | Clonal BMPC ≥60% |
| SLiM - Light chain | Involved/uninvolved sFLC ratio ≥100 |
| SLiM - MRI | >1 focal marrow lesion ≥5 mm on MRI |
Differential Diagnosis of Multiple Myeloma
| Condition | Key distinguishing feature |
|---|---|
| MGUS | M-protein <3 g/dL, BMPC <10%, NO CRAB/SLiM |
| Smoldering MM | M-protein ≥3 g/dL OR BMPC 10-60%, NO CRAB/SLiM |
| Solitary plasmacytoma | Single lesion, BMPC <10%, NO disseminated disease |
| Waldenstrom macroglobulinemia | IgM paraprotein + lymphoplasmacytic lymphoma + hyperviscosity (NOT typically lytic bone disease) |
| AL amyloidosis | Clonal plasma cells + amyloid deposits; may co-exist with MM |
| Metastatic carcinoma to bone | Sclerotic (prostate, breast) or lytic (lung, kidney) lesions; positive bone scan; primary tumor identified |
| Reactive plasmacytosis | Polyclonal, <20% plasma cells, κ/λ ratio normal; secondary to infections, autoimmune disease |
| POEMS syndrome | Polyneuropathy + Organomegaly + Endocrinopathy + M-protein + Skin changes; sclerotic lesions; lambda light chain predominance |
10. RISK STRATIFICATION FOR MGUS PROGRESSION
- M-protein ≥1.5 g/dL
- Non-IgG subtype
- Abnormal sFLC ratio
| Risk Group | # Factors | 20-year progression risk | Risk accounting for competing mortality |
|---|---|---|---|
| Low risk | 0 | 5% | 2% |
| Low-intermediate | 1 | 21% | 10% |
| High-intermediate | 2 | 37% | 18% |
| High risk | 3 | 58% | 27% |
- 10% per year for first 5 years
- 5% per year for next 5 years
- 1-2% per year thereafter
- Risk approaches active myeloma within 2 years
- Now FDA-approved for treatment (daratumumab, AQUILA trial - November 2025)