
IMG20260621081621.jpg
60 yr old female known SHTN came with dyspnea for 1 day and pedal edema for 1 week
Reading File
Searching the Web
ECG left ventricular hypertrophy strain pattern bradycardia heart failure hypertension
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"hypertensive heart disease" AND "heart failure" AND ECG
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have everything needed for a complete, authoritative analysis. Here is the full interpretation:
ECG Analysis & Clinical Interpretation
Patient Summary
60-year-old female | Known systemic hypertension (SHTN) | Dyspnea x 1 day | Pedal edema x 1 week
ECG Findings (Systematic Read)
| Parameter | Finding |
|---|---|
| Rate | 47 bpm (machine-confirmed: "AUTO PRINT... 47bpm") |
| Rhythm | Regular - sinus bradycardia (Rhy II strip confirms P before each QRS) |
| Axis | Left axis deviation (positive in I, negative in III/aVF) |
| P waves | Present, preceding each QRS |
| PR interval | Normal |
| QRS duration | Normal (narrow) |
| Voltage | Deep S in V1/V2 + Tall R in V5/V6 = markedly increased precordial voltage |
| ST-T changes | Downsloping ST depression + asymmetric T-wave inversion in lateral leads (V5, V6, I, aVL) |
| QTc | Borderline prolonged given bradycardia |
Primary ECG Diagnosis
Left Ventricular Hypertrophy (LVH) with Strain Pattern
This ECG is a textbook example. The Goldman-Cecil Medicine textbook describes an almost identical pattern (ECG image above) in a hypertensive patient:
"Note the striking S wave amplitude in the right precordial leads and R wave amplitude in the left precordial leads. Repolarization abnormalities are present in the left precordial leads, as well as the limb leads. Sinus bradycardia (50 beats per minute) is present as well."
- Goldman-Cecil Medicine, ECG Fig 24 (hypertensive LVH)
Voltage Criteria likely met:
- Sokolow-Lyon: S(V1) + R(V5 or V6) - if ≥35 mm, confirms LVH
- Cornell Criterion: S(V3) + R(aVL) - if >20 mm in women, confirms LVH (lower threshold for females)
Strain Pattern (the downsloping ST depression + asymmetric T-wave inversion in V5-V6/lateral leads):
- Defined as ST-segment depression with asymmetric T-wave inversion opposite the QRS axis in lateral leads
- This is the strongest ECG marker of adverse cardiovascular prognosis in hypertensive patients
- Associated with myocardial fibrosis, increased interstitial fibrosis, and diastolic dysfunction
The textbook confirmation from Bailey & Love's:
"There is left ventricular hypertrophy with tall R waves in the lateral leads and ST depression with inverted T waves - ('strain pattern')."
Clinical Correlation & Diagnosis
Most Likely Diagnosis: Acute Decompensated Heart Failure with Preserved Ejection Fraction (HFpEF) secondary to Hypertensive Heart Disease
The triad is complete:
- Known systemic hypertension (decades of pressure overload → LVH)
- ECG: LVH + strain pattern (advanced hypertensive heart disease)
- Clinical presentation: dyspnea (acute onset = pulmonary congestion) + pedal edema (peripheral congestion = 1 week)
The sinus bradycardia at 47 bpm may reflect:
- Antihypertensive medication effect (beta-blockers, diltiazem, verapamil)
- Heightened vagal tone in the setting of heart failure
- Intrinsic sinus node dysfunction
Pathophysiology
Chronic hypertension → pressure overload → concentric LV hypertrophy → diastolic dysfunction (impaired relaxation + reduced compliance) → elevated LV filling pressures → pulmonary venous hypertension → dyspnea + pulmonary edema + systemic venous hypertension → pedal edema.
Immediate Workup Needed
| Investigation | Purpose |
|---|---|
| Echocardiography | Confirm LVH, assess LVEF (HFpEF vs HFrEF), diastolic parameters (E/e'), LA size |
| BNP / NT-proBNP | Confirm heart failure, severity, and guide diuresis |
| Chest X-ray | Cardiomegaly, pulmonary vascular congestion, pleural effusion |
| Renal function + electrolytes | Before diuresis; cardiorenal syndrome assessment |
| CBC | Rule out anemia as precipitant |
| Thyroid function | Hypothyroidism can cause bradycardia + heart failure |
| Troponin | Rule out ACS as precipitant |
| Review medications | Check for beta-blockers/rate-slowing agents causing bradycardia at 47 bpm |
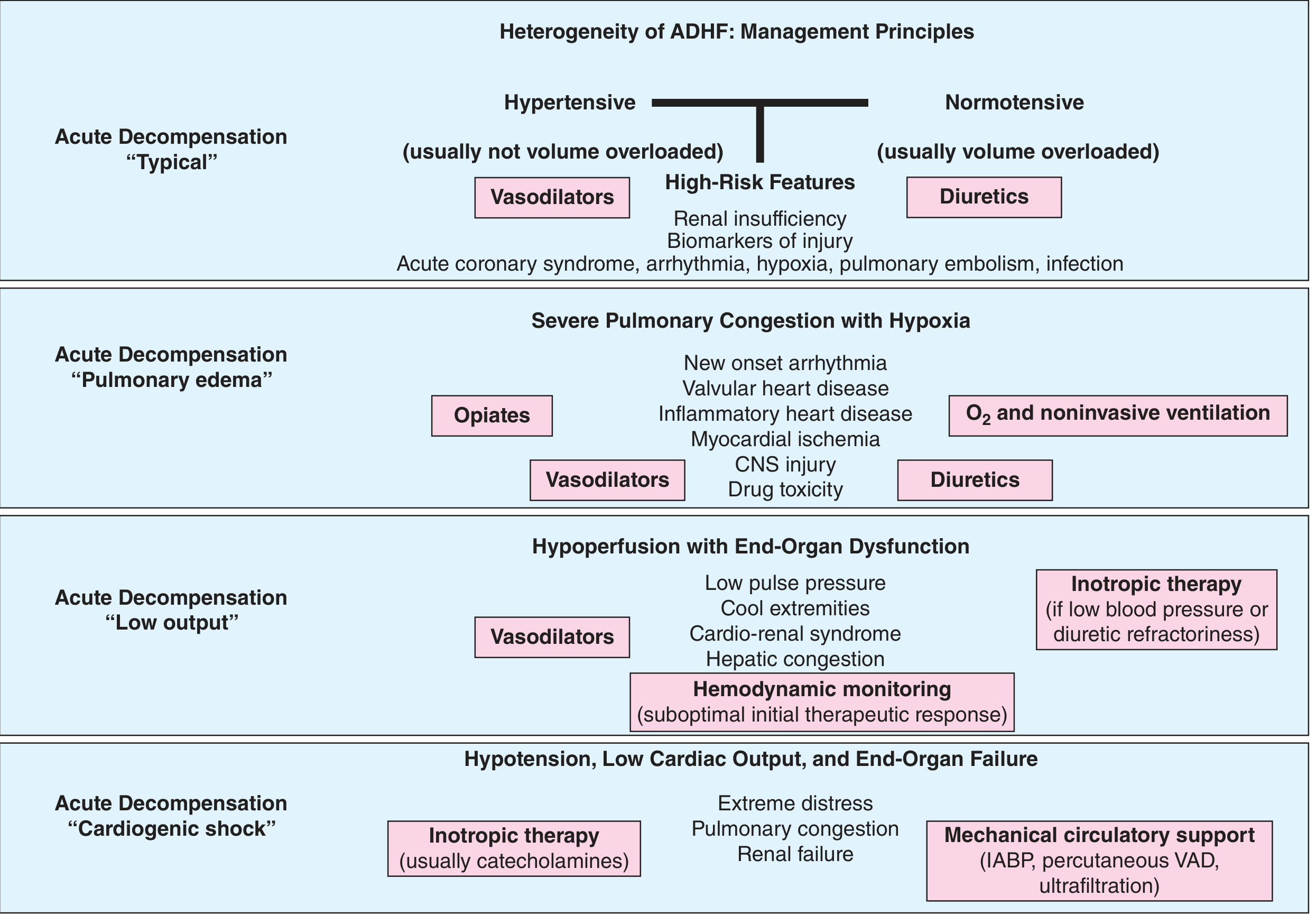
Management (per Harrison's 22E + ADHF flowchart)
This patient fits the "Hypertensive ADHF - Typical" phenotype (from the Harrison's ADHF management diagram above):
Acute Phase:
- Oxygen - target SpO2 >94%; consider non-invasive ventilation (CPAP/BiPAP) if severe
- IV Furosemide - for decongestion (volume overload → pulmonary and peripheral edema); start 40-80 mg IV
- IV Vasodilators (e.g., nitrates) - if BP is elevated; reduces preload and afterload rapidly
- Hold/review bradycardia-causing medications - if on beta-blockers, consider dose reduction given HR of 47 bpm
- Monitor closely - Urine output, electrolytes, renal function
"Aggressive control of blood pressure to guideline-recommended targets and relief of volume overload with diuretics are critical to symptom relief."
- Harrison's Principles of Internal Medicine, 22nd Edition
"Excessive decrease in preload with diuretics and vasodilators may lead to underfilling the ventricle and subsequent azotemia, hypotension, and syncope."
Chronic Phase (after stabilization):
- ACE inhibitor or ARB - for blood pressure control and LVH regression
- Spironolactone/eplerenone - consider for HFpEF + hypertension
- Sacubitril-valsartan - FDA-approved across EF spectrum; benefit greatest in lower EF/women subgroup
- SGLT2 inhibitor (empagliflozin/dapagliflozin) - proven benefit in HFpEF (EMPEROR-Preserved, DELIVER trials)
- Strict BP control (target <130/80 mmHg)
Summary
| ECG Diagnosis | LVH with lateral strain pattern + sinus bradycardia (47 bpm) |
| Clinical Diagnosis | Acute decompensated HFpEF due to hypertensive heart disease |
| Key Risk | ECG strain pattern = strongest predictor of cardiovascular morbidity/mortality in hypertension |
| Immediate Priority | Echo + BNP + CXR → IV diuresis + BP control + review rate-slowing medications |
Sources: Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E; Bailey & Love's Surgery 28E; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.