What is heterophoria and heterotropia squint
Reading File
Finding Sources
Finding Sources
Searching the Web
heterophoria vs heterotropia squint classification types
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from Kanski's Clinical Ophthalmology and Bradley & Daroff's Neurology. Let me compile the full answer.
Heterophoria and Heterotropia (Squint / Strabismus)
Both terms describe misalignment of the visual axes, but they differ fundamentally in whether the deviation is latent or manifest.
The Core Distinction
| Feature | Heterophoria | Heterotropia |
|---|---|---|
| Other name | Latent squint / phoria | Manifest squint / tropia |
| Visibility | Hidden - only detected when fusion is disrupted | Visible at all times (or intermittently) |
| Fusion status | Kept in check by the fusion reflex | Fusion has broken down |
| Binocular single vision | Maintained normally | Lost (or partially maintained in small deviations) |
As Kanski's puts it: "Heterophoria ('phoria') implies a tendency of the eyes to deviate when fusion is blocked (latent squint). Slight phoria is present in most normal individuals and is overcome by the fusion reflex." - Kanski's Clinical Ophthalmology, 10th ed.
HETEROPHORIA (Latent Squint)
Definition
A tendency for the eyes to deviate from perfect alignment that is kept latent (hidden) by the active fusional mechanism. When fusion is disrupted - by covering one eye, fatigue, illness, alcohol, or certain drugs (anticonvulsants, sedatives) - the eye drifts to reveal the underlying deviation.
Orthophoria = perfect ocular balance with no tendency to deviate (rare in absolute form; most people have trace phoria).
Types by Direction
| Type | Deviation |
|---|---|
| Esophoria | Latent inward (convergent) deviation |
| Exophoria | Latent outward (divergent) deviation |
| Hyperphoria | Latent upward deviation |
| Hypophoria | Latent downward deviation |
| Cyclophoria | Latent torsional deviation |
Clinical Subtypes (by distance)
- Convergence excess - esophoria greater at near
- Convergence weakness - esophoria greater at distance
- Divergence weakness - exophoria greater at distance
- Divergence excess - exophoria greater at near
- Mixed - equal at near and distance
When Does It Become a Problem?
Heterophoria is normally well-compensated. It becomes symptomatic (decompensating phoria) when fusional amplitudes are insufficient, causing asthenopia (eye strain, headache, blurring) and possibly diplopia, especially under stress or poor health. It can also decompensate into a frank heterotropia.
Tests to Detect Heterophoria
- Cover-uncover test (uncover component detects phoria)
- Alternate cover test (dissociates fusion; reveals total deviation)
- Maddox rod test - dissociates images for subjective measurement
- Maddox wing - measures heterophoria specifically at near (1/3 m)
- Prism bar cover test - quantifies the angle
Treatment
- Correct any significant refractive error
- Orthoptic exercises (especially for convergence weakness exophoria)
- Prisms - Fresnel prisms temporarily, then incorporated into spectacles (maximum ~10-12 prism dioptres split between both eyes)
- Surgery - for larger deviations unresponsive to other measures
HETEROTROPIA (Manifest Squint / Strabismus)
Definition
A manifest deviation in which the visual axes do not intersect at the fixation point. The images from the two eyes are misaligned. As stated in Kanski's: "Heterotropia ('tropia') implies a manifest deviation in which the visual axes do not intersect at the point of fixation."
Types by Direction
| Type | Deviation |
|---|---|
| Esotropia | Convergent squint (eye turns inward) |
| Exotropia | Divergent squint (eye turns outward) |
| Hypertropia | Eye displaced upward |
| Hypotropia | Eye displaced downward |
| Cyclotropia | Torsional manifest deviation |
Major Classification: Concomitant vs. Incomitant
1. Concomitant (Comitant) Strabismus
- The angle of deviation is the same in all directions of gaze
- Usually no underlying neurological or muscular cause
- Typically develops in childhood
- Examples: infantile esotropia, accommodative esotropia
2. Incomitant (Paralytic/Non-comitant) Strabismus
- The angle of deviation varies with the direction of gaze
- Caused by weakness or restriction of one or more extraocular muscles
- Examples: cranial nerve palsies (CN III, IV, VI), thyroid eye disease, Duane syndrome
By Frequency
- Constant - deviation present at all times
- Intermittent - deviation present only sometimes (some binocularity retained; exotropia is commonly intermittent)
By Eye Fixing
- Unilateral (monocular) - the same eye always deviates; risk of amblyopia is high
- Alternating - either eye may deviate; amblyopia less likely because both foveae are used
Consequences of Heterotropia
- Diplopia - double vision from misaligned visual axes
- Esotropia = uncrossed (homonymous) diplopia
- Exotropia = crossed (heteronymous) diplopia
- Suppression - cortical suppression of the deviating eye's image to avoid diplopia
- Central suppression: foveal image suppressed (avoids confusion)
- Peripheral suppression: peripheral image suppressed (avoids diplopia)
- Amblyopia - if constant unilateral suppression persists before visual maturity (~6 years), the deviating eye fails to develop normal visual acuity permanently ("lazy eye")
- Anomalous Retinal Correspondence (ARC) - non-corresponding retinal points acquire a shared visual direction; allows some rudimentary binocular vision in small-angle squints (microtropia)
Summary Diagram
SQUINT (Strabismus)
├── HETEROPHORIA (Latent)
│ ├── Esophoria (inward tendency)
│ ├── Exophoria (outward tendency)
│ ├── Hyperphoria / Hypophoria (vertical)
│ └── Cyclophoria (torsional)
│
└── HETEROTROPIA (Manifest)
├── By direction: Esotropia / Exotropia / Hyper / Hypo
├── Concomitant (angle same in all gazes)
└── Incomitant (angle varies with gaze direction)
├── Paralytic (e.g. CN palsy)
└── Restrictive (e.g. thyroid eye disease)
Key clinical pearl: A heterophoria can decompensate into a heterotropia under physiological stress (fatigue, illness, drugs). In children, new-onset tropia must always prompt refraction and fundus examination to exclude underlying pathology before attributing it to a simple motor imbalance.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Ch. 18; Bradley and Daroff's Neurology in Clinical Practice, Ch. 18
What is diploplia and types Explain about it to mr
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have everything needed for a thorough, well-structured explanation. Let me compile the answer now.
Diplopia (Double Vision) - A Complete Explanation
What is Diplopia?
Diplopia is the perception of two images of a single object simultaneously - in simple terms, seeing double. It occurs when the visual axes of the two eyes are misaligned so that the same object projects its image onto non-corresponding points on the two retinas, causing the brain to perceive two separate images.
As Adams and Victor's Neurology states: "The term binocular diplopia refers to the symptom of double vision caused by a misalignment of the visual axes of the two eyes. It is only present when both eyes are open and can see. Covering one eye obliterates double vision that stems from misalignment of the eyes."
The Two Fundamental Types
The most important first step in any patient with diplopia is to ask: "Does the double vision go away when you close either eye?"
1. Monocular Diplopia
- Definition: Double vision that persists even when one eye is closed - the affected eye alone sees two images
- Cause: A problem intrinsic to the eye itself, not an alignment problem
- Common causes:
- Corneal irregularities (keratoconus, pterygium, astigmatism)
- Cataract (lens opacities split the image)
- Uncorrected refractive error
- Foveal traction or retinal disease
- Occasionally: malingering or psychiatric/functional disorder
- Key point: Monocular diplopia is almost never a neurological emergency. It is a local ocular problem.
2. Binocular Diplopia
- Definition: Double vision that is present only with both eyes open and disappears immediately when either eye is covered
- Cause: Misalignment of the visual axes (ocular motor problem)
- Key point: Binocular diplopia always demands investigation - it can signal serious neurological, vascular, or systemic disease
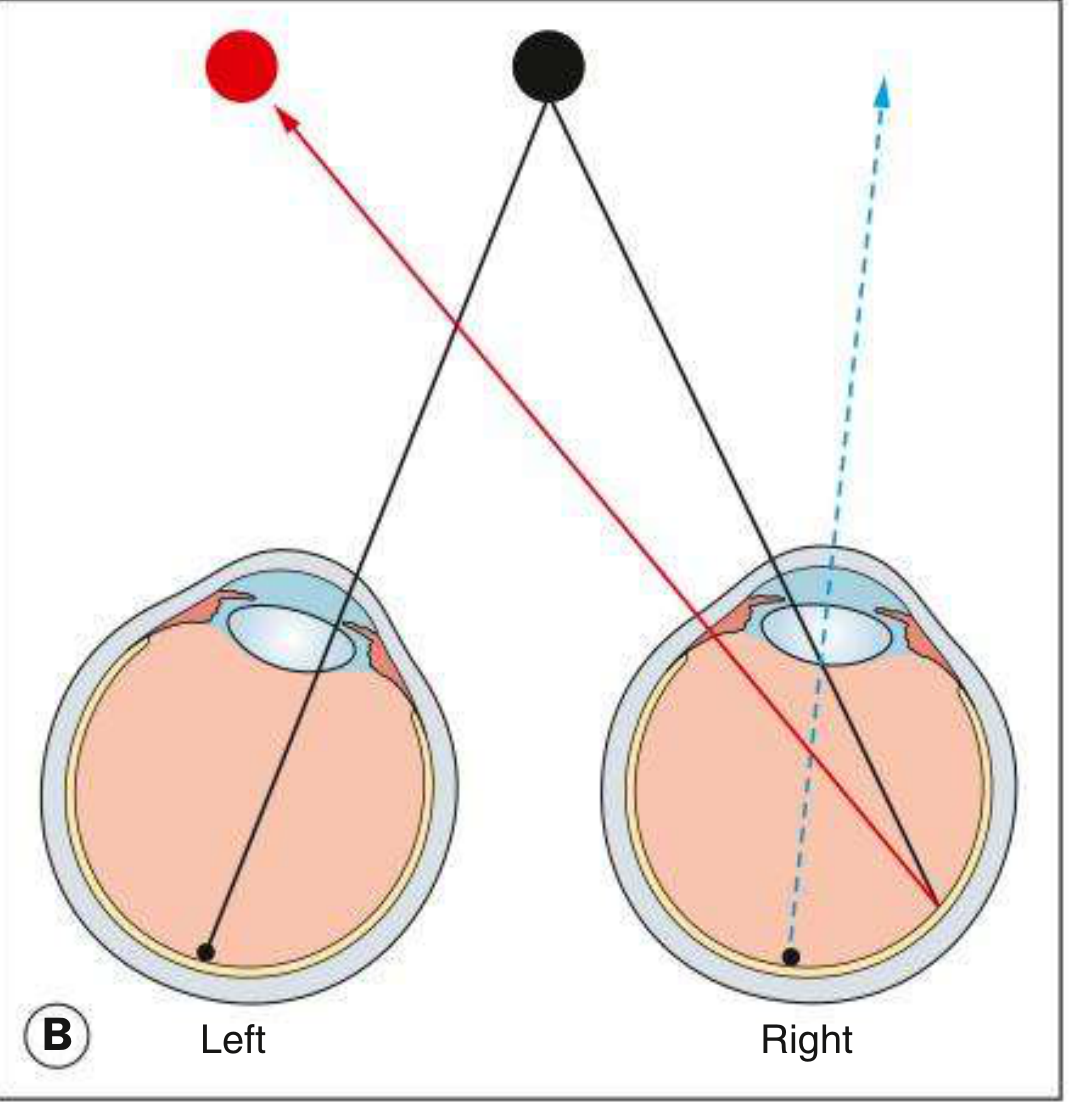
Heteronymous (crossed) diplopia in right exotropia - Kanski's Clinical Ophthalmology, 10th ed.
Classification of Binocular Diplopia
A. By Direction of Image Separation
| Type | Description | Seen In |
|---|---|---|
| Horizontal diplopia | Two images side by side | Esotropia, exotropia (CN VI or medial rectus palsy) |
| Vertical diplopia | One image above the other | Hypertropia, CN IV palsy, skew deviation |
| Torsional (oblique) diplopia | Images tilted relative to each other | CN IV palsy (trochlear nerve), oblique muscle problems |
| Mixed | Combination of horizontal + vertical | CN III palsy, orbital disease |
B. By Position of the False Image
| Type | Squint Present | Image Position |
|---|---|---|
| Homonymous (uncrossed) diplopia | Esotropia (eye turns in) | False image is on the same side as the squinting eye |
| Heteronymous (crossed) diplopia | Exotropia (eye turns out) | False image is on the opposite side to the squinting eye |
Memory trick: In esotropia (inward turn), the deviating eye's image is projected outward - so it appears on the same side. In exotropia (outward turn), the image is projected inward - appearing on the opposite side.
C. By Cause (Most Clinically Important Classification)
1. Neurogenic Diplopia (Cranial Nerve Palsies)
The most common cause of binocular diplopia requiring urgent workup.
| Nerve | Muscle Affected | Pattern of Diplopia | Other Signs |
|---|---|---|---|
| CN III (Oculomotor) | All except LR and SO | Diplopia in all directions except lateral gaze to same side; eye is "down and out" | Ptosis, dilated pupil (if compressive) |
| CN IV (Trochlear) | Superior oblique | Vertical + torsional diplopia; worse on looking down and inward | Head tilt away from affected side (compensatory) |
| CN VI (Abducens) | Lateral rectus | Horizontal diplopia; worse on looking to the affected side; esotropia | Most common isolated cranial nerve palsy |
2. Neuromuscular Junction Diplopia
- Myasthenia Gravis - the classic cause of painless, variable, fatigable diplopia. Not confined to a single nerve distribution. Pupils always normal. Worsens with sustained activity, improves with rest.
- Botulism - can mimic ocular myasthenia
3. Restrictive (Mechanical) Diplopia
Caused by physical restriction of globe movement, not nerve weakness:
- Thyroid eye disease (Graves') - fibrosis of inferior and medial recti; commonest cause is restriction of elevation (inferior rectus fibrosis)
- Orbital blowout fracture - inferior rectus or inferior oblique entrapment; vertical diplopia with upward gaze limitation
- Orbital pseudotumor / myositis - painful diplopia with proptosis
- Orbital tumors / abscesses
4. Supranuclear / Central Diplopia
Problems in the brainstem pathways:
- Internuclear ophthalmoplegia (INO) - lesion of the medial longitudinal fasciculus (MLF); impaired adduction of one eye with nystagmus in the abducting eye; classic in multiple sclerosis
- Skew deviation - vertical misalignment from brainstem or cerebellar lesions
- Alcohol or anticonvulsant toxicity - can cause transient diplopia by disrupting conjugate gaze
Key Clinical Assessment
Step 1 - Cover Test
Cover one eye: if diplopia disappears = binocular. If persists = monocular.
Step 2 - Direction of maximum diplopia
Ask: "In which direction of gaze is the double vision worst?" The weak muscle acts in the direction where the gap between images is greatest.
Step 3 - Identifying the false image
The image furthest from the midline (most peripheral) always belongs to the abnormal eye. As Neuroanatomy through Clinical Cases explains: "When an extraocular muscle is not working properly, the image further from the midline toward the direction of attempted gaze is always the one seen by the abnormal eye."
Step 4 - Red Glass Test
A red glass is placed over one eye (usually right). The patient looks at a white light and reports the position of the red vs. white images in 9 positions of gaze. This helps identify which muscle is weak.
Step 5 - Head posture
Patients often adopt a compensatory head posture to minimize diplopia (e.g., head tilt in CN IV palsy, face turn in CN VI palsy).
Quick Summary Diagram
DIPLOPIA (Double Vision)
│
├── MONOCULAR (one eye closed = still double)
│ └── Cause: cornea, lens, retina, refractive error
│ → NOT a neurological emergency
│
└── BINOCULAR (one eye closed = resolves)
└── Cause: ocular misalignment
│
├── By direction: Horizontal / Vertical / Torsional / Mixed
│
├── By image position: Homonymous / Heteronymous
│
└── By cause:
├── Neurogenic (CN III, IV, VI palsy)
├── Neuromuscular (Myasthenia gravis, Botulism)
├── Restrictive (Thyroid, Fracture, Tumor)
└── Central (INO, skew deviation, toxins)
Clinical pearl from Harrison's: "The first point to clarify is whether diplopia persists in either eye after the opposite eye is covered. If it does, the diagnosis is monocular diplopia... Diplopia alleviated by covering one eye is binocular diplopia and is caused by disruption of ocular alignment."
Sources: Adams and Victor's Principles of Neurology, 12th ed.; Harrison's Principles of Internal Medicine, 22nd ed.; Kanski's Clinical Ophthalmology, 10th ed.; Rosen's Emergency Medicine; Neuroanatomy through Clinical Cases, 3rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.