Inguinal canal
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have all the information needed to write a comprehensive answer. Let me compile this:
Inguinal Canal
Overview
The inguinal canal is a slit-like oblique passage in the lower anterior abdominal wall, approximately 4-6 cm long in adults, running downward and medially just above and parallel to the lower half of the inguinal ligament. It begins at the deep (internal) inguinal ring and ends at the superficial (external) inguinal ring.
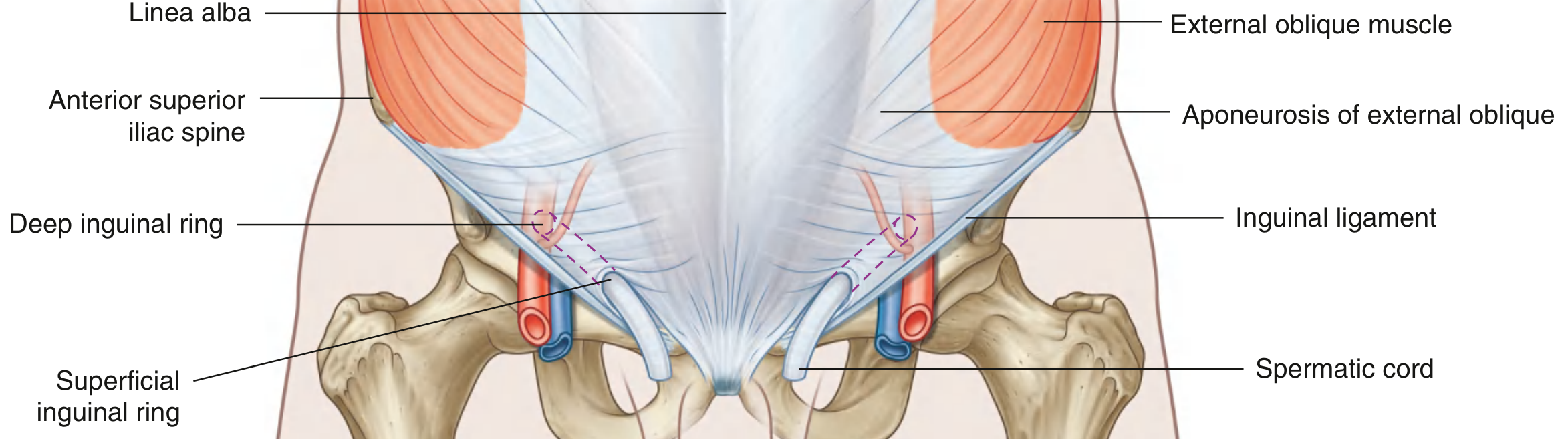
Fig. 4.42 - Inguinal Canal (Gray's Anatomy for Students)
Openings
Deep (Internal) Inguinal Ring
- Located midway between the anterior superior iliac spine (ASIS) and the pubic symphysis, just above the inguinal ligament
- Lies immediately lateral to the inferior epigastric vessels - this relationship is key for distinguishing hernia types
- Not a simple defect in the transversalis fascia, but rather the beginning of a tubular evagination of transversalis fascia - this evagination becomes the internal spermatic fascia around the spermatic cord (or around the round ligament in women)
Superficial (External) Inguinal Ring
- Located superior to the pubic tubercle, at the end of the canal
- A triangular opening in the aponeurosis of the external oblique muscle
- Apex points superolaterally; base is formed by the pubic crest
- Medial crus attaches to the pubic symphysis; lateral crus attaches to the pubic tubercle
- The two crura are held together by intercrural fibers at the apex, preventing further widening
- The evagination of the external oblique aponeurosis over the spermatic cord here becomes the external spermatic fascia
Walls
| Wall | Formed By |
|---|---|
| Anterior wall | Aponeurosis of external oblique (entire length); reinforced laterally by lower fibers of internal oblique (over the deep ring) |
| Posterior wall | Transversalis fascia (entire length); reinforced medially by the conjoint tendon (inguinal falx) in its medial one-third |
| Roof (superior wall) | Arching fibers of transversus abdominis and internal oblique muscles |
| Floor (inferior wall) | Medial half of the inguinal ligament (rolled-under free margin of external oblique aponeurosis); lacunar ligament reinforces the medial part |
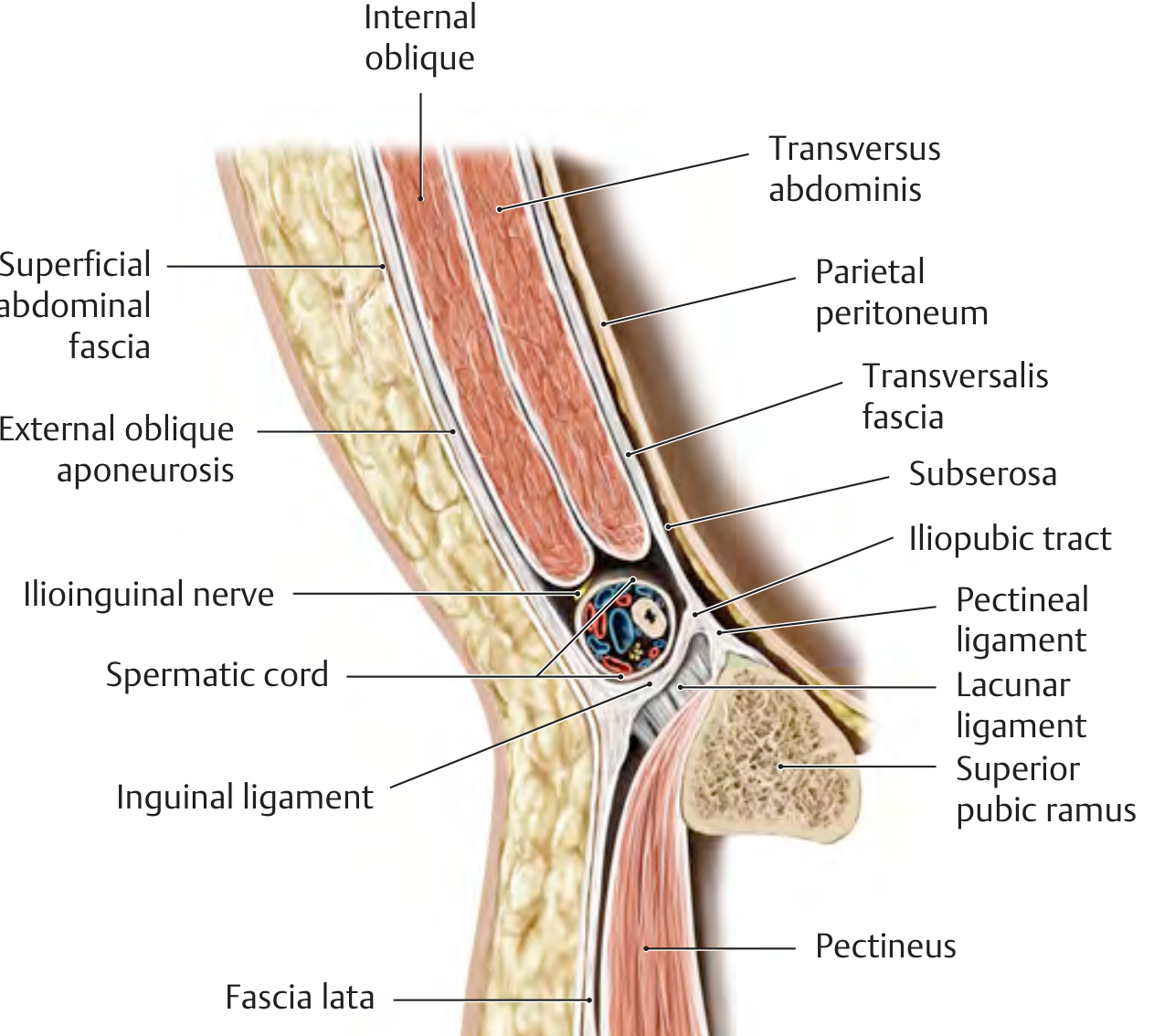
Sagittal cross-section through the inguinal canal - THIEME Atlas of Anatomy
Contents
In Males
- Spermatic cord - containing:
- Vas deferens (ductus deferens)
- Testicular artery
- Pampiniform plexus of veins
- Testicular and cremasteric lymphatics
- Autonomic nerve fibers
- Ilioinguinal nerve (L1) - runs on the surface of the spermatic cord, exits through the superficial ring
- Genital branch of the genitofemoral nerve (L1/L2) - runs within the cremasteric fascia, supplies the cremaster muscle and scrotal skin
In Females
- Round ligament of the uterus (ends in the labia majora)
- Genital branch of the genitofemoral nerve - accompanies the round ligament
- Ilioinguinal nerve - also traverses part of the canal
Layers of the Spermatic Cord (from outside in)
The spermatic cord acquires three fascial coverings as it passes through the inguinal canal, each derived from a different abdominal wall layer:
| Layer | Derived From |
|---|---|
| External spermatic fascia | Aponeurosis of external oblique |
| Cremasteric fascia + cremaster muscle | Internal oblique + transversus abdominis |
| Internal spermatic fascia | Transversalis fascia |
Clinical Significance
Cremasteric Reflex
Stroking the medial thigh (sensory: ilioinguinal nerve, L1) causes contraction of the cremaster muscle (motor: genital branch of genitofemoral nerve, L1/L2), elevating the testis. Absence of this reflex suggests L1 spinal cord pathology, and it can also be absent in testicular torsion.
Inguinal Hernias
The inguinal canal is the most common site of herniation in the body.
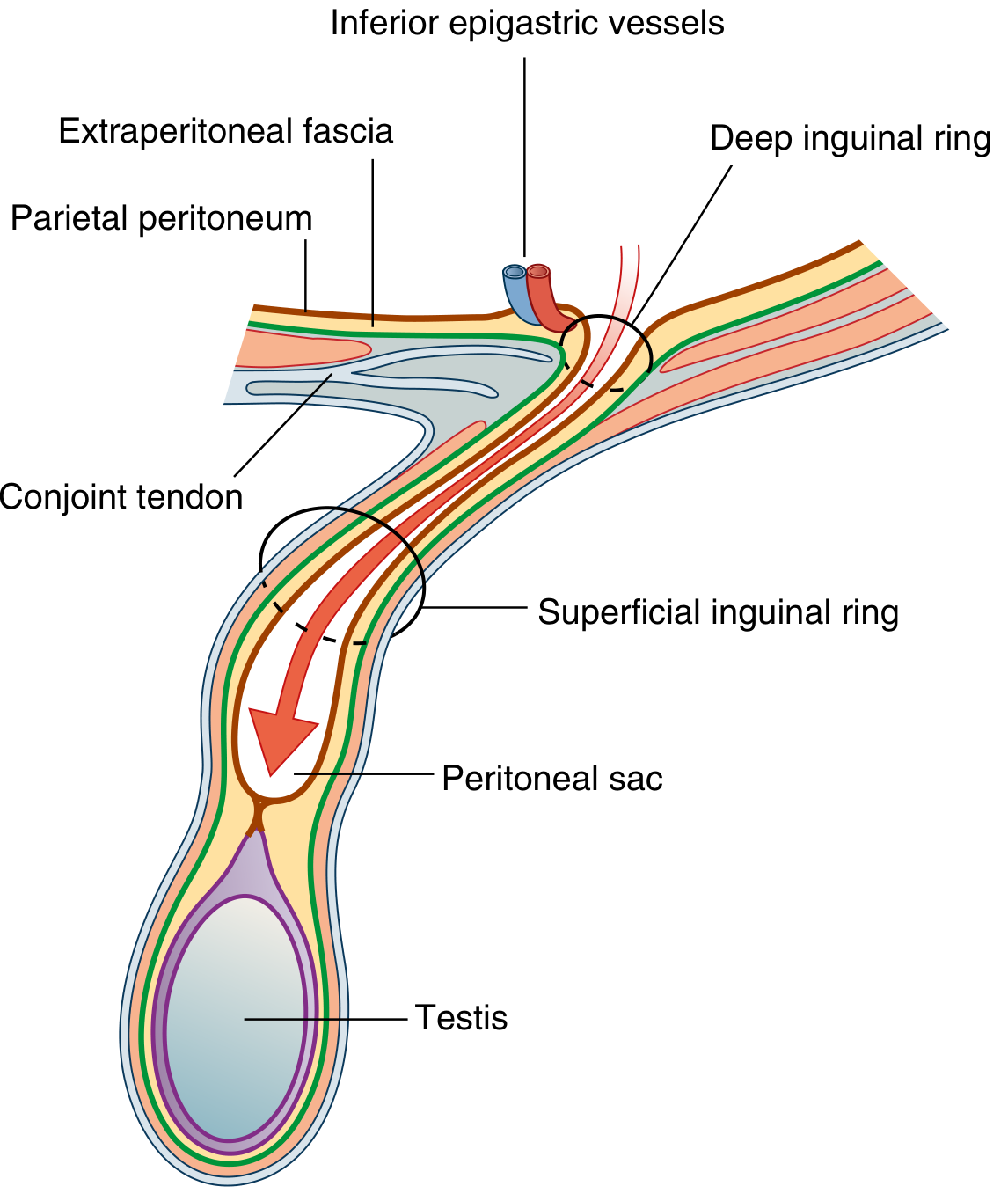
Indirect inguinal hernia - peritoneal sac following the path of the spermatic cord (Gray's Anatomy for Students)
Indirect Inguinal Hernia
- Most common type; more common in men
- Enters the inguinal canal through the deep inguinal ring - lateral to the inferior epigastric vessels
- Due to persistence of the processus vaginalis (congenital basis)
- The sac passes obliquely through the canal and can descend all the way to the scrotum (scrotal hernia) or labia majora
- Acquires all three coverings of the spermatic cord as it passes through
Direct Inguinal Hernia
- Always acquired; typically in older men with weakened abdominal muscles
- Bulges directly through the posterior wall of the canal, medial to the inferior epigastric vessels
- Passes through Hesselbach's triangle (inguinal triangle), bounded by:
- Laterally: inferior epigastric artery
- Medially: lateral border of rectus abdominis
- Inferiorly: inguinal ligament
- Does not traverse the full length of the inguinal canal; may still exit through the superficial ring
Key Distinction - Indirect vs. Direct
The relationship of the hernia neck to the inferior epigastric vessels is the key distinguishing feature:
- Indirect: lateral to the vessels (comes through the deep ring)
- Direct: medial to the vessels (comes through the posterior wall)
Embryological Note
The inguinal canal forms during fetal development as the testis descends from the posterior abdominal wall to the scrotum, pulling a peritoneal sleeve (the processus vaginalis) with it. This sleeve normally obliterates after birth; failure to do so is the anatomical basis of indirect inguinal hernias in neonates and children. The gubernaculum - a ligamentous mesenchymal condensation - guides this descent.
Sources:
- Gray's Anatomy for Students, pp. 352-359
- Bailey and Love's Short Practice of Surgery (28th ed.), p. 1087
- General Anatomy and Musculoskeletal System (THIEME Atlas of Anatomy), p. 231
Create a detailed anatomy reference PDF on the inguinal canal
Reading File
Running Command
Running Command
Running Command
Writing File
Running Command
Editing File
Editing File
Running Command
Editing File
Editing File
Editing File
Running Command
Running Command
Your PDF is ready:
Inguinal Canal Anatomy Reference
PDF Document · PDF
Here's what's included across the 11 pages:
| Section | Content |
|---|---|
| Cover page | Styled title page with design and source credits |
| Table of contents | Numbered, linked to all 11 sections |
| 1. Overview | Definition, dimensions, orientation, key-facts callout box |
| 2. Openings | Deep ring (location, structure, muscular guard) + superficial ring (crura, intercrural fibres) - with 2 labelled diagrams |
| 3. Walls | All four walls in a comparison table + mnemonic callout box + sagittal cross-section image |
| 4. Contents | Detailed table for male contents (structure/function/origin); female contents; lymphatic drainage clinical note |
| 5. Spermatic cord layers | Three-layer table with derivation + mnemonic "Every Cremaster Is Important" |
| 6. Neurovascular relations | Nerve table (ilioinguinal, genitofemoral, iliohypogastric) + inferior epigastric vessel landmarks |
| 7. Inguinal hernias | Indirect vs. direct with diagrams; full comparison table (8 features) |
| 8. Hesselbach's triangle | Boundaries table + laparoscopic view image + "RIL" mnemonic |
| 9. Cremasteric reflex | Arc components table; torsion clinical pearl |
| 10. Embryology | Step-by-step testicular descent; processus vaginalis outcomes table |
| 11. Clinical summary | High-yield 14-point table; all mnemonics in coloured callout boxes |
This is a shared conversation. Sign in to Orris to start your own chat.