From now for topic follow the below structure 1. Introduction 2. History (if relevant) 3. Anatomy 4. Etiology 5. Mechanism (if applicable) 6. Pathology 7. Clinical Features 8. Investigation 9. Radiograph 10. CT 11. MRI 12. Classification 13. Treatment A. Non-operative B. Operative 14. Recent Advances Additional features:include diagram and flow chart
Got it! I'll follow that structured format for every topic going forward, covering all 14 sections with diagrams and flowcharts included. Just tell me the first topic you'd like covered and I'll get started.
Common peroneal nerve
Reading File
Finding Sources
Searching the Web
common peroneal nerve anatomy injury classification treatment
Searching PubMed
"common peroneal nerve" injury treatment
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Generating Image
Generating Image
Loading Image
I now have all the information needed. Let me compile the comprehensive structured response.
Common Peroneal Nerve
1. Introduction
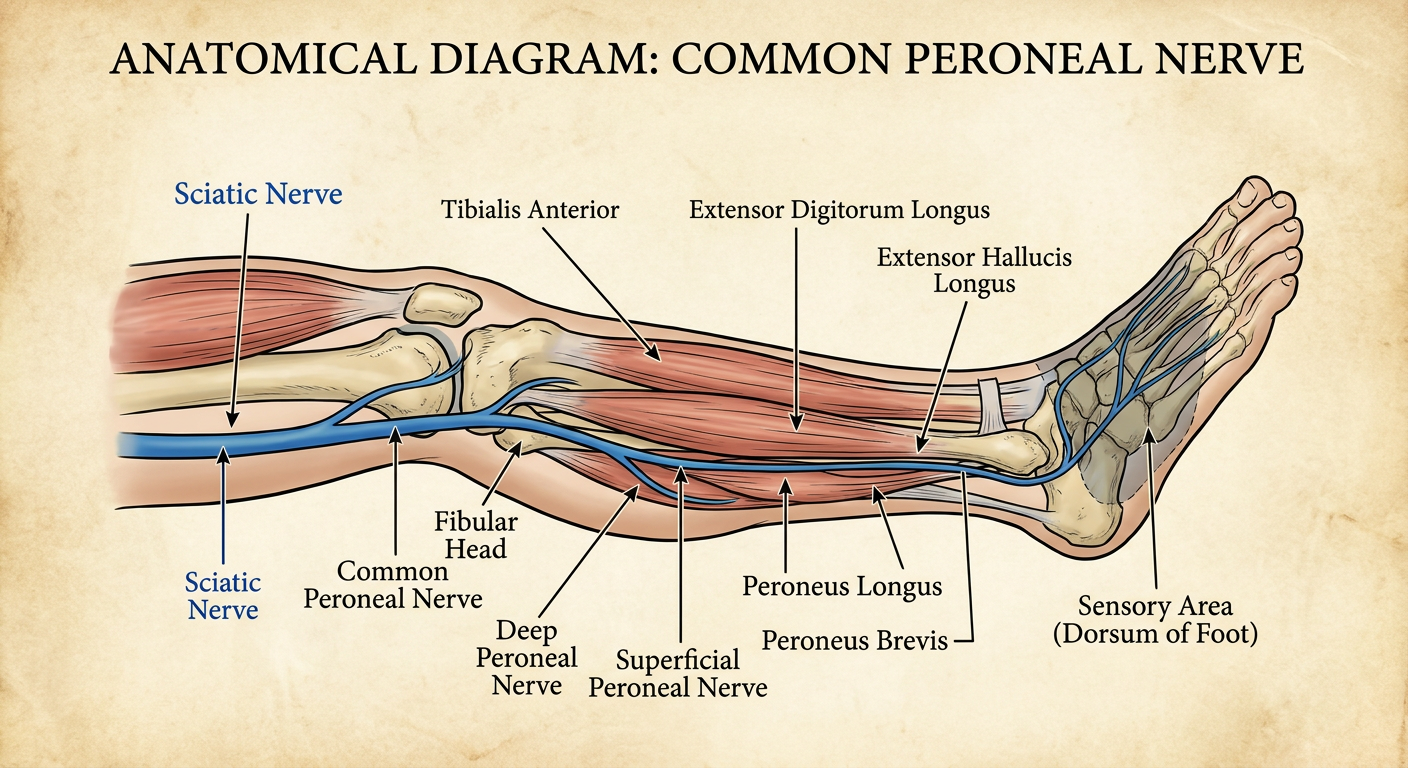
The common peroneal nerve (CPN), also called the common fibular nerve, is the lateral terminal division of the sciatic nerve. It is the most commonly injured peripheral nerve in the lower extremity, accounting for its vulnerability to both traumatic and compressive injuries. Damage produces the characteristic clinical syndrome of foot drop - inability to dorsiflex the foot - along with variable sensory loss over the anterolateral leg and dorsum of the foot. Understanding its anatomy is the key to understanding why it is so prone to injury and how to manage the sequelae.
2. History
- The peroneal nerve and foot drop have been recognised since antiquity, with the term "peroneal" derived from the Greek perone (fibula).
- Sir Herbert Seddon (1942) and Sir Sydney Sunderland (1951) developed the nerve injury classification systems still used today.
- The condition was historically recognised in occupational settings (strawberry pickers, textile workers) and in soldiers after prolonged crouching (trench palsy).
- "Punter's palsy" - peroneal injury from ankle inversion while kicking - was described in American football literature.
- The concept of intraneural ganglia from the superior tibiofibular joint as an underappreciated cause was clarified in modern imaging studies.
3. Anatomy
Origin and Root Value
- Root values: L4, L5, S1, S2
- Arises as the lateral division of the sciatic nerve, separating from it in the posterolateral aspect of the popliteal fossa (or higher in the thigh in cases of early bifurcation)
Course
| Segment | Relations |
|---|---|
| Popliteal fossa | Lies in a fat plane between lateral head of gastrocnemius and biceps femoris |
| Around fibular head | Turns around the biceps femoris tendon and fibular head - most vulnerable point |
| Fibular tunnel | Passes under a fibrous arch at the origin of peroneus longus muscle |
| Proximal leg | Divides into 3 branches |
Branches
- Superficial peroneal nerve - innervates peroneus longus and brevis (ankle eversion); sensory to anterolateral distal leg and dorsum of foot (except 1st web space)
- Deep peroneal nerve - innervates tibialis anterior, extensor digitorum longus, extensor hallucis longus, extensor digitorum brevis (ankle dorsiflexion, toe extension); sensory to 1st dorsal web space
- Recurrent articular nerve - sensory to knee joint
- Lateral sural cutaneous nerve - sensory to upper lateral leg
Motor Innervation Summary
| Muscle | Action | Branch |
|---|---|---|
| Tibialis anterior | Dorsiflexion + inversion | Deep peroneal |
| Extensor digitorum longus | Toe extension, dorsiflexion | Deep peroneal |
| Extensor hallucis longus | Big toe extension | Deep peroneal |
| Extensor digitorum brevis | Toe extension | Deep peroneal |
| Peroneus longus | Eversion, plantarflexion | Superficial peroneal |
| Peroneus brevis | Eversion | Superficial peroneal |
Anatomical Diagram
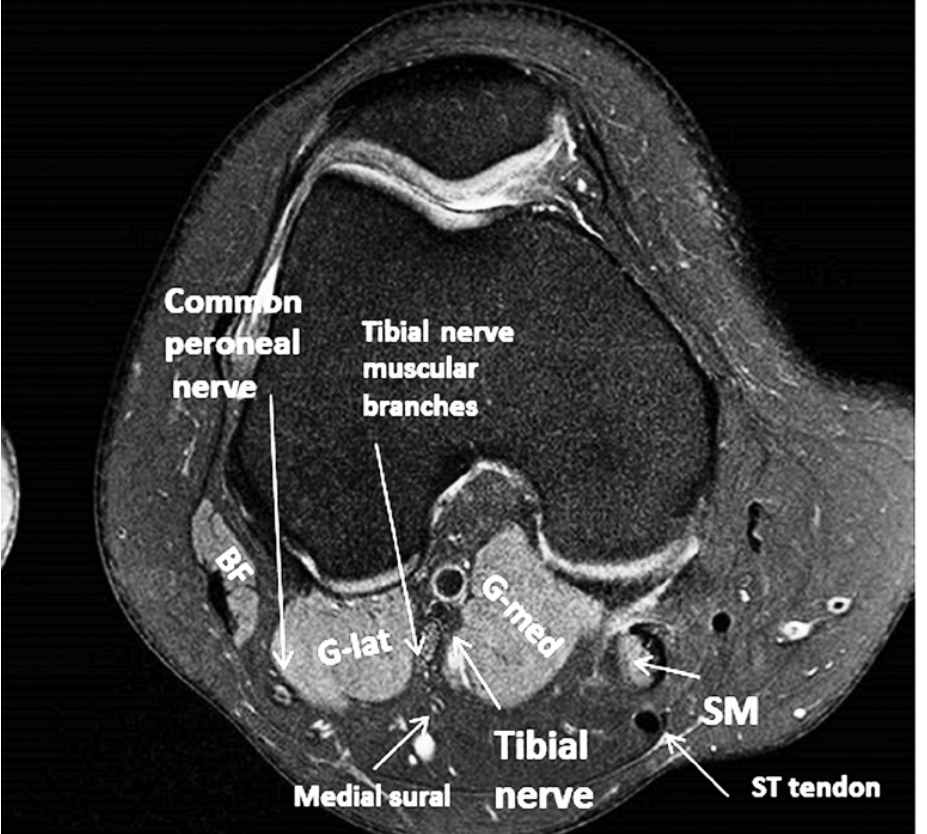
MRI Anatomy - Axial View at Knee (Distal Popliteal Fossa)
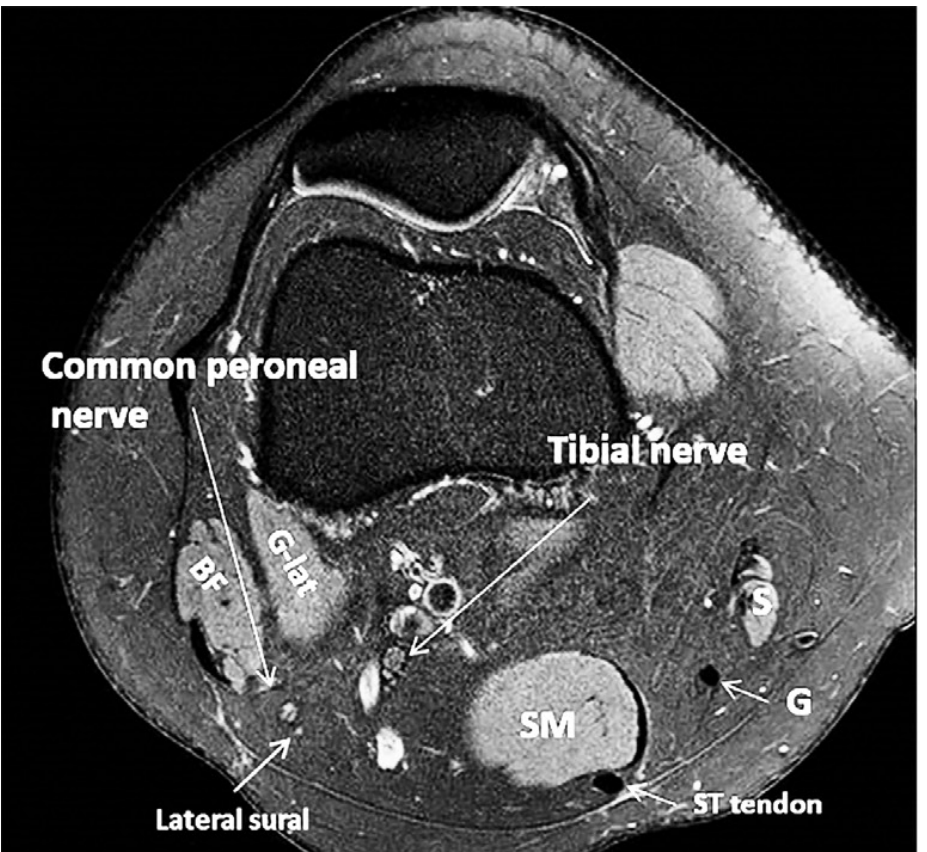
Fig: Axial MRI at the popliteal fossa. The common peroneal nerve lies lateral between the biceps femoris (BF) and lateral gastrocnemius (G-lat). Tibial nerve is medial. - Imaging Anatomy, Vol. 3
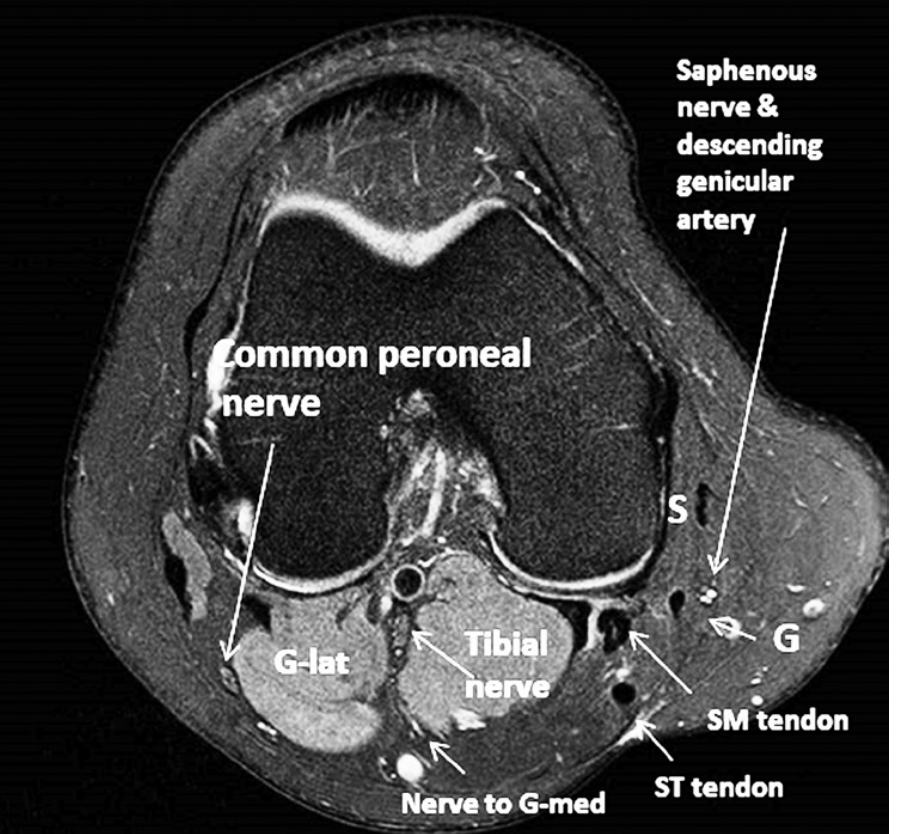
Fig: Axial MRI at the level of the distal popliteal fossa showing the common peroneal nerve and tibial nerve with surrounding structures. - Imaging Anatomy, Vol. 3
Why Is the CPN So Vulnerable?
Six anatomical factors contribute:
- Superficial course around the fibular neck - no deep muscle coverage
- Tethered proximally by the biceps femoris tendon and distally by the peroneus longus arch
- Limited excursion - the nerve has restricted ability to move away from the fibular head
- Bony prominence - the fibular head acts as a pulley, concentrating mechanical stress
- Early proximal bifurcation in some individuals increases the exposure length
- Fascicular arrangement - the deep peroneal fascicles lie on the deep surface at the fibular neck, pressed directly against bone
4. Etiology
Traumatic
| Cause | Notes |
|---|---|
| Knee dislocation / multiligament injury | CPN injured in up to 44% of posterolateral corner injuries |
| Fracture of fibular head/neck | ~50% of fibular head fractures have associated CPN injury |
| Direct blow to lateral knee | Classic "car bumper" injury |
| Knee arthroplasty (TKA) | Especially with valgus correction; lithotomy position |
| Laceration / penetrating trauma | Wartime, iatrogenic |
Compressive / Positional
| Cause | Notes |
|---|---|
| Habitual leg crossing | Most common compressive cause |
| Prolonged squatting | Strawberry pickers, yoga (yoga foot drop) |
| Tight plaster cast | Pressure at fibular neck |
| Obstetric stirrups / lithotomy position | Bilateral palsy during prolonged labour (pushing palsy) |
| Prolonged bed rest / immobility | Weight loss + emaciation exacerbates risk |
| Tight knee boots | External compression |
Space-Occupying Lesions
- Baker cyst extending into retropopliteal space
- Intraneural ganglion (from superior tibiofibular joint - an underrecognised but treatable cause)
- Ganglion cyst, lipoma, osteochondroma at fibular head
- Hematoma, aneurysm
Medical/Systemic
- Diabetic neuropathy - lower ischaemic threshold predisposes to entrapment
- Vasculitis - nerve infarct
- Leprosy
- Anorexia nervosa / cancer / AIDS - emaciation removes protective fat padding
Iatrogenic
- Postoperative positioning (lateral decubitus, lithotomy)
- Orthopaedic operations (high tibial osteotomy, TKA)
- Poorly applied casts, bandages, or splints
5. Mechanism
General Mechanisms
1. Compression/Entrapment
The nerve is pressed between the fibular head and overlying soft tissues. Sustained pressure causes local ischaemia → segmental demyelination → neurapraxia. If sustained, progresses to axonal injury.
2. Traction / Stretch
Forced plantarflexion-inversion of the ankle (e.g., punter's palsy, knee dislocation) stretches the nerve around its fibular tether. Traction injury more commonly produces axonotmesis or neurotmesis than pure compression.
3. Direct Laceration
Complete or partial nerve transection. Requires surgical intervention.
4. Intraneural Ganglion Mechanism
Disruption of the superior tibiofibular joint capsule allows synovial fluid to dissect along the articular branch of the CPN retrogradely into the main nerve trunk, creating a cystic expansion with intraneural compression.
5. Ischaemia
Compartment syndrome of the anterior/lateral compartment → ischaemic neuropathy affecting the deep peroneal nerve particularly.
6. Pathology
Wallerian Degeneration
Distal to a complete axonal injury, the axon and myelin sheath undergo Wallerian degeneration within 3-7 days. Schwann cells proliferate to form bands of Büngner, guiding regenerating axons.
Nerve Regeneration Rate
- Axonal regeneration proceeds at 1-3 mm/day (approximately 1 inch per month)
- Grade 1-2 injuries: rapid regeneration, excellent recovery
- Grade 3: slower (~1 mm/day), incomplete and unpredictable
- Grades 4-5: no spontaneous regeneration; requires surgical intervention
Denervation Changes in Muscle
- Fibrillation potentials appear on EMG within 3 weeks of axonal injury
- Muscle atrophy begins within weeks; irreversible after approximately 12-18 months
- This establishes the critical window for surgical nerve repair (should not exceed 12 months)
7. Clinical Features
Symptoms
- Foot drop - inability to dorsiflex the foot; the hallmark presentation
- High-stepping gait (steppage gait) - hip and knee flexed excessively to clear the toe from the ground
- Sensory loss over anterolateral leg and dorsum of foot (deep peroneal pattern: 1st web space only; superficial peroneal: broader dorsum)
- Pain - variable; more common with intraneural ganglia or entrapment
- Onset may be acute (trauma) or noticed on waking (compression during sleep)
Signs
| Finding | Significance |
|---|---|
| Weakness of dorsiflexion | Deep peroneal branch |
| Weakness of eversion | Superficial peroneal branch |
| Preserved inversion | Tibial nerve (L4/L5 mediated) - key differentiator from L5 root |
| Preserved plantar flexion | Tibial nerve intact |
| Sensory loss dorsum of foot | Superficial peroneal |
| Sensory loss 1st web space only | Deep peroneal branch only |
| Tinel's sign at fibular head | Suggests compressive/regenerating lesion |
| Steppage gait | Compensation for foot drop |
Selective Deep Peroneal Involvement
In many fibular head lesions, the deep branch fascicles (lying on the deep/medial surface) are preferentially injured, producing predominantly dorsiflexion weakness with relative sparing of eversion. In some cases, the extensor hallucis longus fascicle alone is affected, producing big toe drop rather than full foot drop.
Differential Diagnosis of Foot Drop
| Condition | Key Distinguishing Features |
|---|---|
| CPN palsy | Eversion weak, inversion spared, Tinel at fibular head, NCS abnormal |
| L5 radiculopathy | Inversion AND eversion weak, hip abduction may be weak, back pain, EMG shows paraspinal changes |
| Lumbosacral plexopathy | Broader deficit, hip abduction weak |
| ALS/motor neuron disease | Upper motor neuron signs, widespread fasciculations |
| Tibialis anterior tendon rupture | Palpable gap, normal EMG |
8. Investigation
Clinical
- Detailed neurological examination (motor testing, sensory mapping, reflexes)
- Tinel's sign at fibular head
- Assessment for systemic causes (diabetes, weight loss, vasculitis)
Electrodiagnostic Studies (Gold Standard)
| Study | Finding in CPN Palsy |
|---|---|
| Motor NCS | Slowed conduction velocity across fibular head; reduced CMAP amplitude distal to lesion; localises lesion |
| Sensory NCS | Reduced/absent superficial peroneal SNAP |
| EMG (needle) | Fibrillation potentials, reduced recruitment in tibialis anterior, EHL, EDL, peroneus muscles |
| EMG paraspinals | Normal in CPN palsy - differentiates from L5 radiculopathy |
Key NCS finding: Conduction block (>50% drop in CMAP amplitude) across fibular head = neurapraxia (good prognosis). Axonal loss (reduced amplitude throughout) = axonotmesis or worse.
EMG findings appear 3 weeks post-injury - early testing may be falsely reassuring.
Laboratory
- Blood glucose / HbA1c (diabetes screen)
- ESR, ANCA, cryoglobulins (if vasculitis suspected)
9. Radiograph
Plain X-rays have limited direct utility for nerve assessment but are essential for:
- Fibular head/neck fractures - up to 50% have associated CPN injury
- Knee dislocation - identifies bony injury
- Tibial plateau fractures - associated with posterolateral corner and CPN injury
- Calcification near fibular head suggesting ganglion calcification or bony lesion
- Assessment of alignment (valgus knee increases CPN stretch risk)
10. CT
CT is not the primary modality for nerve assessment but is useful for:
- Characterising bony lesions (osteochondroma, exostosis) compressing the nerve
- Fracture detail at fibular head - exact fracture pattern, displacement
- Pre-operative planning for complex periarticular fractures
- Identifying calcified ganglia
- CT myelogram if MR contraindicated and radiculopathy is in the differential
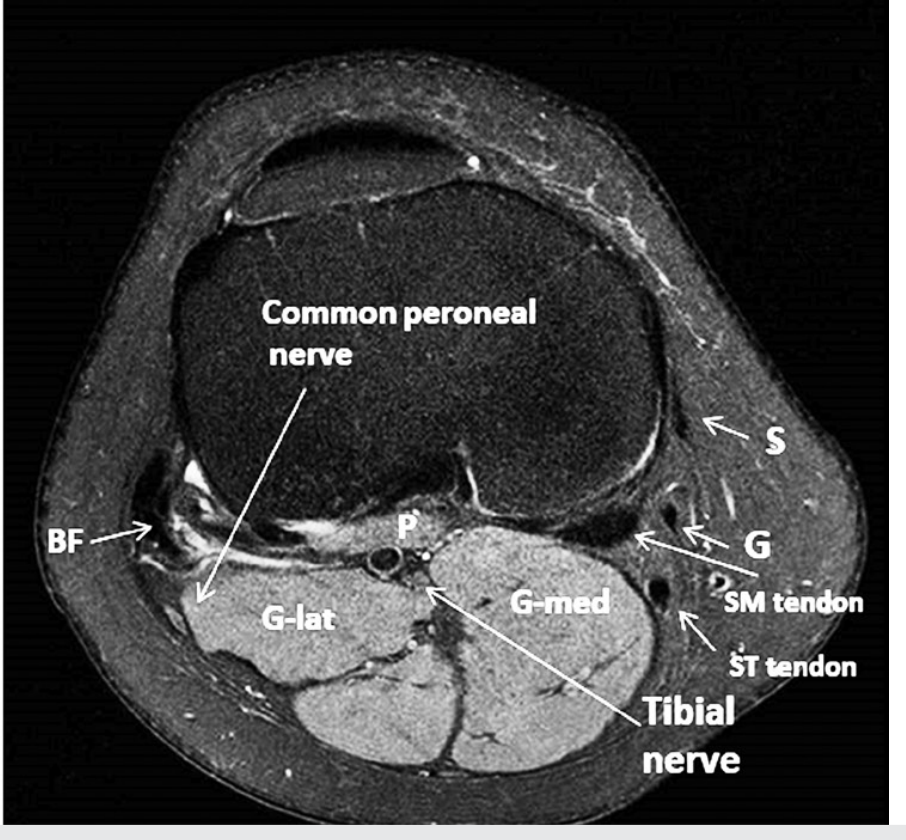
Axial CT/MR hybrid image at the knee level showing the common peroneal nerve in relation to biceps femoris, lateral gastrocnemius, and fibula. - Imaging Anatomy, Vol. 3
11. MRI
MRI is the imaging modality of choice for the common peroneal nerve.
Normal MRI Appearance
- Nerve appears as small bundles of fascicles in a supporting fatty background
- Isointense to muscle on T1; slightly hyperintense on T2/PD
- Best seen on axial sequences; nerve typically visible in most routine knee MRI sequences
Pathological Findings
| Finding | Significance |
|---|---|
| T2 hyperintensity of nerve without enlargement | Neurapraxia (reversible) |
| T2 hyperintensity + nerve enlargement | Axonotmesis, inflammation |
| Nerve discontinuity / neuroma | Neurotmesis (Sunderland grade 5) |
| Intraneural cystic lesion tracking from tibiofibular joint | Intraneural ganglion |
| Denervation changes in anterior compartment (T2 bright muscle) | Subacute/chronic axonal injury |
| Fat replacement in anterior compartment muscles | Chronic denervation (irreversible) |
MRI Knee Series (Axial)
Axial MRI showing the common peroneal nerve at the level of the femoral condyles, adjacent to lateral gastrocnemius (G-lat) and medial gastrocnemius (G-med) origins. - Imaging Anatomy, Vol. 3
MRI Protocol
- Knee MRI: Standard sequences + dedicated axial T1 spin echo for nerve mapping
- High-resolution peripheral nerve MRI (MR neurography): 3T, 3D STIR or DWIBS sequences; allows nerve tracking from sciatic origin to distal branches
- Coverage should extend from proximal thigh to proximal fibula to encompass entire vulnerable segment
12. Classification
Seddon Classification (1942)
| Grade | Description | Prognosis |
|---|---|---|
| Neurapraxia | Myelin injury only; axon intact; conduction block | Full recovery in weeks-months without surgery |
| Axonotmesis | Axon disrupted; endoneurium intact | Recovery at 1-3 mm/day; usually good |
| Neurotmesis | Complete nerve division including connective tissue sheaths | No spontaneous recovery; surgery required |
Sunderland Classification (1951) - More Detailed
| Grade | Structures Disrupted | Recovery Potential |
|---|---|---|
| 1 | Myelin only (= neurapraxia) | Full; within 12 weeks |
| 2 | Axon discontinuity; endoneurium intact (= axonotmesis) | Excellent; rapid regeneration at 2-3 mm/day |
| 3 | Axon + endoneurium; perineurium intact | Incomplete, unpredictable; ~1 mm/day; intraneural scarring |
| 4 | Axon + endoneurium + perineurium; epineurium intact | No spontaneous recovery; neuroma-in-continuity |
| 5 | Complete nerve disruption (= neurotmesis) | No recovery; end neuroma formation |
| 6 (MacKinnon addition) | Mixed/combined pattern across fascicles | Variable early recovery then plateau |
Classification by Location
| Level | Features |
|---|---|
| Above knee (sciatic level) | Combined tibial + peroneal deficits |
| Fibular head (most common) | Classic CPN palsy |
| Deep peroneal only | Dorsiflexion weakness; eversion spared |
| Superficial peroneal only | Eversion weakness; sensory on dorsum |
| Anterior tarsal tunnel | Extensor digitorum brevis + 1st web space |
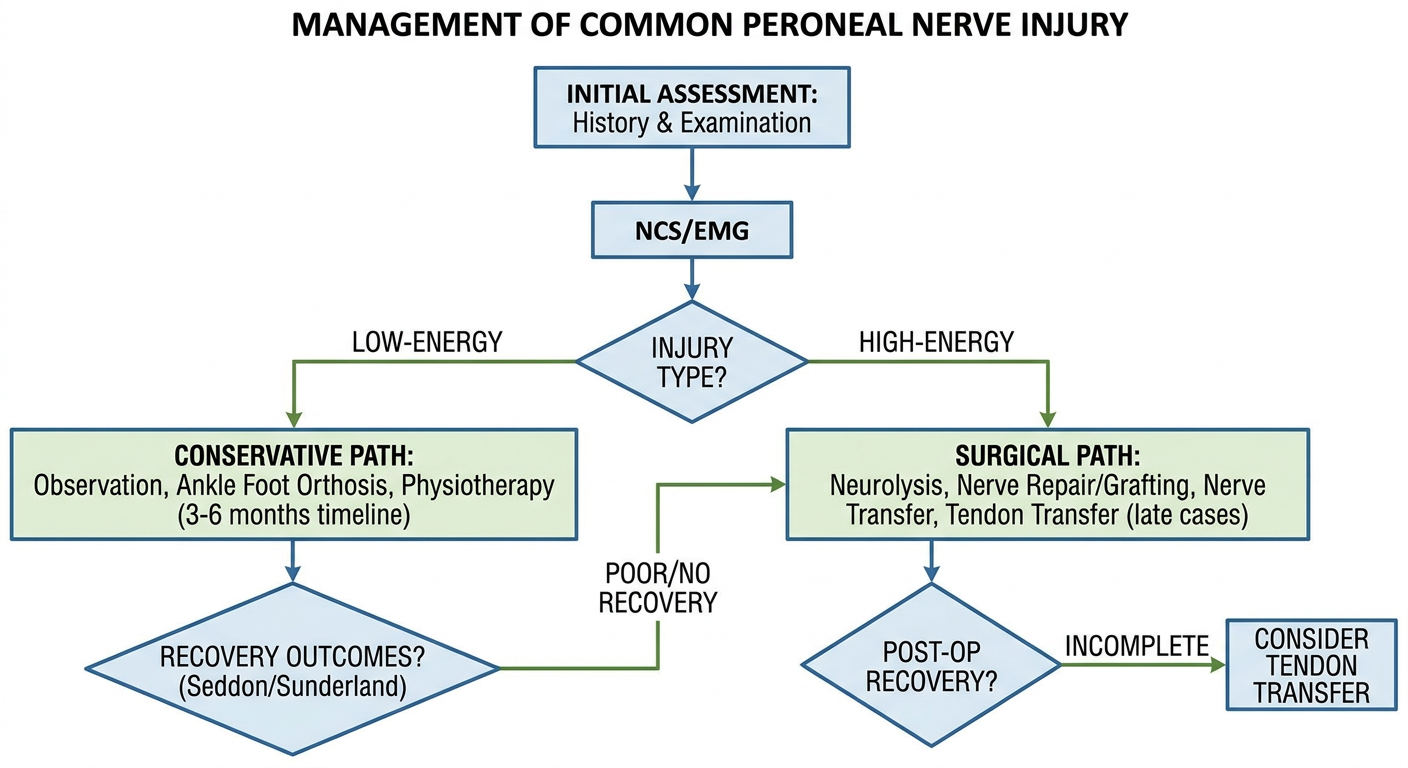
13. Treatment
Management Flowchart
A. Non-Operative Management
Indications:
- Neurapraxia (Sunderland grade 1) / low-energy compressive injuries
- Axonotmesis with reasonable recovery potential
- Systemic/metabolic cause amenable to treatment
1. Activity Modification and Risk Factor Elimination
- Avoid leg crossing, prolonged squatting
- Rapid weight loss if entrapment related to obesity causing excess pressure
- Treat underlying diabetes, vasculitis, hypothyroidism
- Pad lateral knee if continued pressure unavoidable
2. Ankle-Foot Orthosis (AFO)
- Rigid or articulated AFO maintains ankle in neutral dorsiflexion during swing phase
- Provides:
- Toe dorsiflexion during swing phase
- Medial/lateral stability at ankle during stance
- Push-off stimulation during late stance
- Carbon fibre AFOs are lightweight and functionally superior to traditional polypropylene
3. Physiotherapy
- Maintain joint range of motion to prevent contracture
- Stretching of triceps surae to prevent equinus
- Strengthening of intact muscle groups
- Gait retraining
4. Functional Electrical Stimulation (FES)
- Peroneal nerve stimulator devices (e.g., WalkAide, Bioness L300)
- Surface electrode over CPN triggers dorsiflexion during swing phase
- Increasingly used as first-line adjunct to AFO
5. Observation Period
- Neurapraxia: expect recovery within 4-12 weeks
- Axonotmesis: observe for 3-6 months for signs of reinnervation
- Serial EMG/NCS to track recovery
- No spontaneous improvement after 3-6 months → surgical re-evaluation
B. Operative Management
Indications for Surgery:
- High-energy injuries (laceration, fracture-dislocation, gunshot) → explore within 3 weeks
- No recovery after 3-6 months of observation (low energy) or no recovery at 3 months (axonal loss on NCS)
- Known anatomical compressor (ganglion, tumour, bony fragment)
- Intraneural ganglion confirmed on MRI
Critical Surgical Principle: Nerve repair results become suboptimal if surgery is performed more than 12 months after injury or if graft length required exceeds 12 cm.
1. Neurolysis (External and Internal)
- Release of fibrous/scar tissue compressing the nerve externally (external neurolysis) or between fascicles (internal neurolysis)
- Indications: entrapment, neuroma-in-continuity (Sunderland grade 3-4), intraneural ganglion
- For intraneural ganglia: decompression + resection of articular branch + tibiofibular joint capsule repair to prevent recurrence
- Success in up to 60-70% if performed within 6 months of injury
2. Nerve Repair (Neurorrhaphy)
- Primary repair: Direct epineural or fascicular suture; only if tension-free
- Indications: sharp laceration, early exploration, small gap
- Best results when performed early with short gap and low lesion
- Under ideal conditions (early, low lesion, small gap): 60-70% achieve useful dorsiflexion (anti-gravity)
3. Nerve Grafting
- For gaps > 2-3 cm preventing tension-free repair
- Autograft (sural nerve, medial cutaneous nerve of forearm) remains the gold standard
- Mean graft length in published series: 7 cm; shorter grafts give significantly better outcomes
- Among 465 patients undergoing peroneal nerve reconstruction: 49% achieved >M3 recovery - Sabiston Textbook of Surgery
- Allograft (processed decellularised nerve) used for gaps 5-70 mm when donor site morbidity must be minimised
4. Nerve Transfer
- Transfers a fascicle from the tibial nerve to the distal CPN (end-to-end fashion)
- Used when proximal stump unavailable or gap too long for grafting
- Meta-analysis: 62.9% achieved >M3 function with tibial-to-CPN nerve transfer
- Avoids long regeneration distances; particularly useful for proximal injuries
5. Tendon Transfer (Salvage Procedure)
- For late presentations (>12-18 months), irreversible denervation, or failed nerve repair
- Standard transfer: Tibialis posterior transfer to dorsum of foot (Bridle procedure or direct transfer through interosseous membrane)
- Restores active dorsiflexion using a tibial nerve-innervated muscle
- Additional: peroneus longus to brevis transfer, toe extensor augmentation
- Most reliable and durable long-term solution for established foot drop
Surgical Approach
- Patient supine or lateral decubitus; thigh tourniquet
- Longitudinal incision from popliteal fossa, curving anterolaterally around fibular head
- Knee flexion relaxes the nerve
- Expose nerve from popliteal fossa to fibular tunnel
- Protect sural nerve branch
14. Recent Advances
1. MR Neurography (High-Resolution Nerve Imaging)
- 3T MRI with dedicated surface coils, 3D-STIR and diffusion tensor imaging (DTI) allows direct visualisation of the nerve, fascicular detail, and continuity - aiding surgical planning
2. Nerve Transfers
- Expanding use of selective tibial nerve branch transfer to deep peroneal nerve targets (tibialis anterior, EHL)
- End-to-side neurorrhaphy techniques allow partial reinnervation without fully sacrificing donor nerve
3. Intraoperative Nerve Monitoring and Nerve Stimulation
- Intraoperative EMG and nerve action potential (NAP) recording during surgery guides extent of resection vs neurolysis in neuroma-in-continuity cases
4. Nerve Conduits and Processed Allografts
- Polyglycolic acid and collagen conduits for short gaps (< 3 cm); processed nerve allografts (Avance) for 5-70 mm gaps avoiding donor site morbidity from sural nerve harvest
5. Functional Electrical Stimulation (FES) / Neuroprosthetics
- Implantable FES systems (e.g., ActiGait, Bioness L300 Plus) with closed-loop gait-triggered stimulation are now in clinical use, providing functional improvement equivalent to or better than fixed AFO
6. Platelet-Rich Plasma (PRP) and Growth Factors
- Emerging evidence for PRP injection at lesion site to promote remyelination and axonal regeneration; mostly experimental
7. Ultrasound-Guided Diagnosis and Intervention
- High-frequency ultrasound (15-18 MHz) allows real-time dynamic assessment of the nerve at the fibular head, identification of ganglion cysts, and ultrasound-guided aspiration of intraneural ganglia
8. Intraneural Ganglion - Tibiofibular Joint Repair
- Recognition that recurrence after simple decompression is reduced by articular branch excision and tibiofibular joint capsule repair - now the standard surgical approach
Quick Reference Summary
| Feature | Detail |
|---|---|
| Root value | L4, L5, S1, S2 |
| Origin | Lateral division of sciatic nerve |
| Most vulnerable point | Fibular head/neck |
| Most common injury | Compression/entrapment |
| Key clinical sign | Foot drop + weak eversion, preserved inversion |
| Gold standard investigation | NCS/EMG |
| Critical repair window | < 12 months post-injury |
| Best surgical outcome | 60-70% achieve anti-gravity dorsiflexion (ideal conditions) |
| Late salvage | Tibialis posterior tendon transfer |
Sources:
- Adams & Victor's Principles of Neurology 12th Ed - Common Peroneal Nerve, p. 1165
- Localization in Clinical Neurology 8th Ed - Lesions of the Common Peroneal Nerve, p. 154-156
- Harrison's Principles of Internal Medicine 22nd Ed - Peroneal Neuropathy
- Imaging Anatomy Vol. 3 - Peroneal Nerve, p. 307-310
- Campbell's Operative Orthopaedics 15th Ed 2026 - Peroneal Nerve Repair, p. 3017-3019
- Sabiston Textbook of Surgery 8th Ed - Outcomes After Peroneal Nerve Repair
- EFORT Open Reviews - Evidence-based algorithm for CPN injury management (2016)
Generate a quick reference clinical decision support PDF on CPN injury management
For answer structure given According to Orthopaedics point of view
Reading File
Running Command
Running Command
Writing File
Running Command
Editing File
Running Command
Editing File
Running Command
Running Command
Running Command
Writing File
This is a shared conversation. Sign in to Orris to start your own chat.