Discuss emergency management of massive pulmonary embolism
Reading File
Finding Sources
Searching PubMed
"massive pulmonary embolism" AND "emergency management"
Reading File
Reading File
Searching PubMed
"pulmonary embolism" AND "thrombolysis" AND "management"
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive, detailed content from multiple authoritative textbooks. I also have the key management flowchart. Let me now compile the complete answer.
Emergency Management of Massive Pulmonary Embolism
Autopsy Image: Massive PE
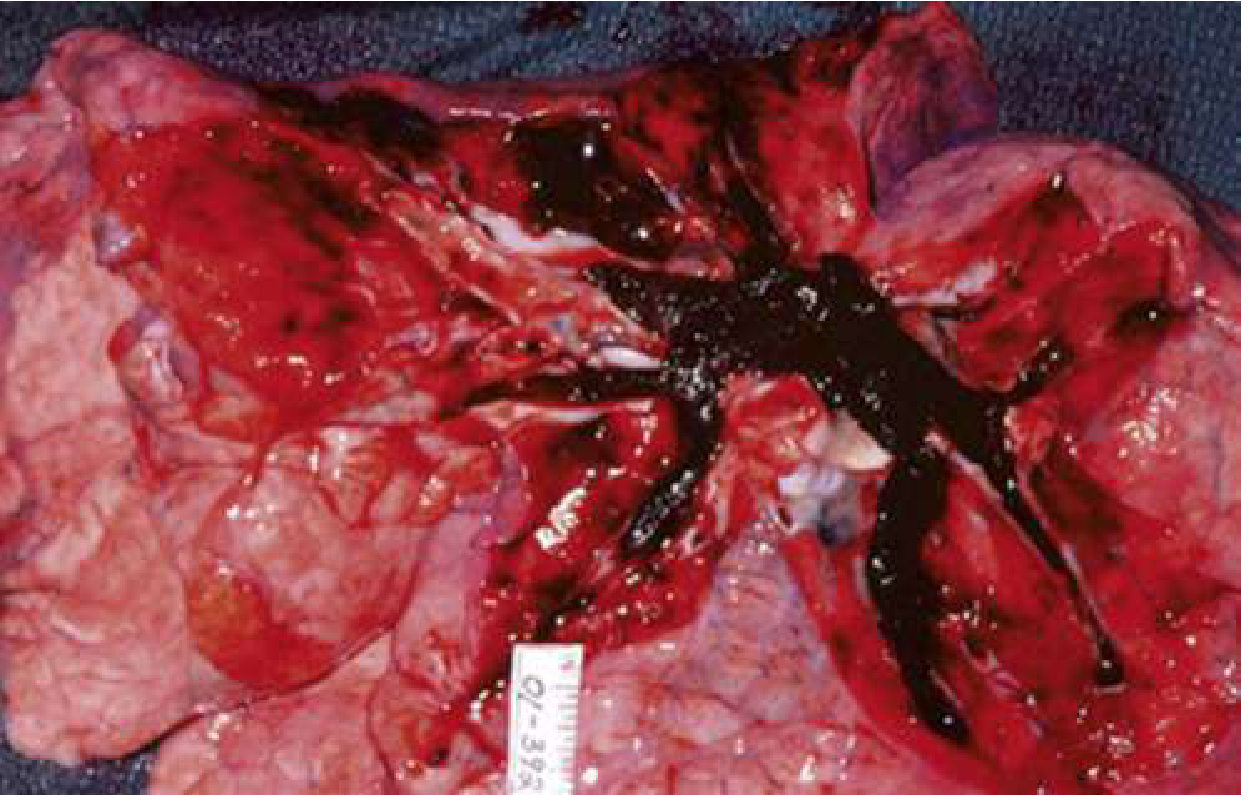
Autopsy photograph showing a massive pulmonary embolism (dark thrombus) completely occluding the right ventricular outflow system. (Rosen's Emergency Medicine, 10e)
1. Definition and Classification
Massive (high-risk) PE is defined by hemodynamic instability, specifically:
- Systolic BP < 90 mmHg sustained for ≥15 minutes not attributable to dysrhythmia or other cause
- A drop in baseline SBP of >40 mmHg
- Requirement for vasopressors
- Profound bradycardia (<40 bpm)
| Category | Criteria | Mortality |
|---|---|---|
| Low-risk | Normotensive, no RV dysfunction | ~1.1% |
| Intermediate-risk | Normotensive + RV dysfunction and/or elevated troponin/BNP | Elevated |
| High-risk (Massive) | Hemodynamically unstable | 25-50% |
2. Pathophysiology of Hemodynamic Collapse
When a large thrombus obstructs >50% of the pulmonary vascular bed, pulmonary artery pressure rises acutely. The right ventricle, which is a thin-walled, low-pressure chamber, is unable to sustain this sudden afterload increase. This produces:
- Acute RV dilation - the RV distends toward the interventricular septum ("D-sign")
- Septal bowing - this reduces LV filling volume and cardiac output
- Myocardial ischemia - RV wall tension compresses coronary perfusion; septal tension on the AV node may produce agonal rhythms
- PEA arrest - the most common cardiac arrest rhythm in PE (>20 depolarizations/min without palpable pulses)
Approximately 25% of sudden cardiac deaths are attributed to PE. Prior to arrest, the classic finding is a shock index >1 (HR > systolic BP), combined with hypoxia, overt respiratory distress, syncope, and severe anxiety.
3. Immediate Resuscitation Priorities
A. Airway and Oxygenation
- Supplemental oxygen targeting SpO₂ >90% to prevent hypoxic pulmonary vasoconstriction (which worsens acute pulmonary hypertension)
- Avoid intubation whenever possible - positive-pressure ventilation increases intrathoracic pressure, reduces preload, and can precipitate complete hemodynamic collapse in severe PE
- When intubation is unavoidable, optimize hemodynamics with vasopressors before induction
B. Hemodynamic Resuscitation
- Cautious fluid resuscitation: small boluses (250-500 mL) may improve cardiac output, but aggressive fluid loading worsens RV distension and further compresses the LV - use with restraint
- Vasopressors: norepinephrine is the first-line vasopressor for hemodynamic support
- Dobutamine: useful adjunct for RV support, but may worsen hypotension unless co-administered with norepinephrine
C. Anticoagulation
- Initiate IV unfractionated heparin (UFH) immediately in all suspected massive PE - UFH is preferred when thrombolysis or surgical intervention is being considered (short half-life allows rapid reversal)
- Do not delay anticoagulation while awaiting imaging in hemodynamically unstable patients with high clinical suspicion
4. Definitive Treatment: Reperfusion
Management Flowchart
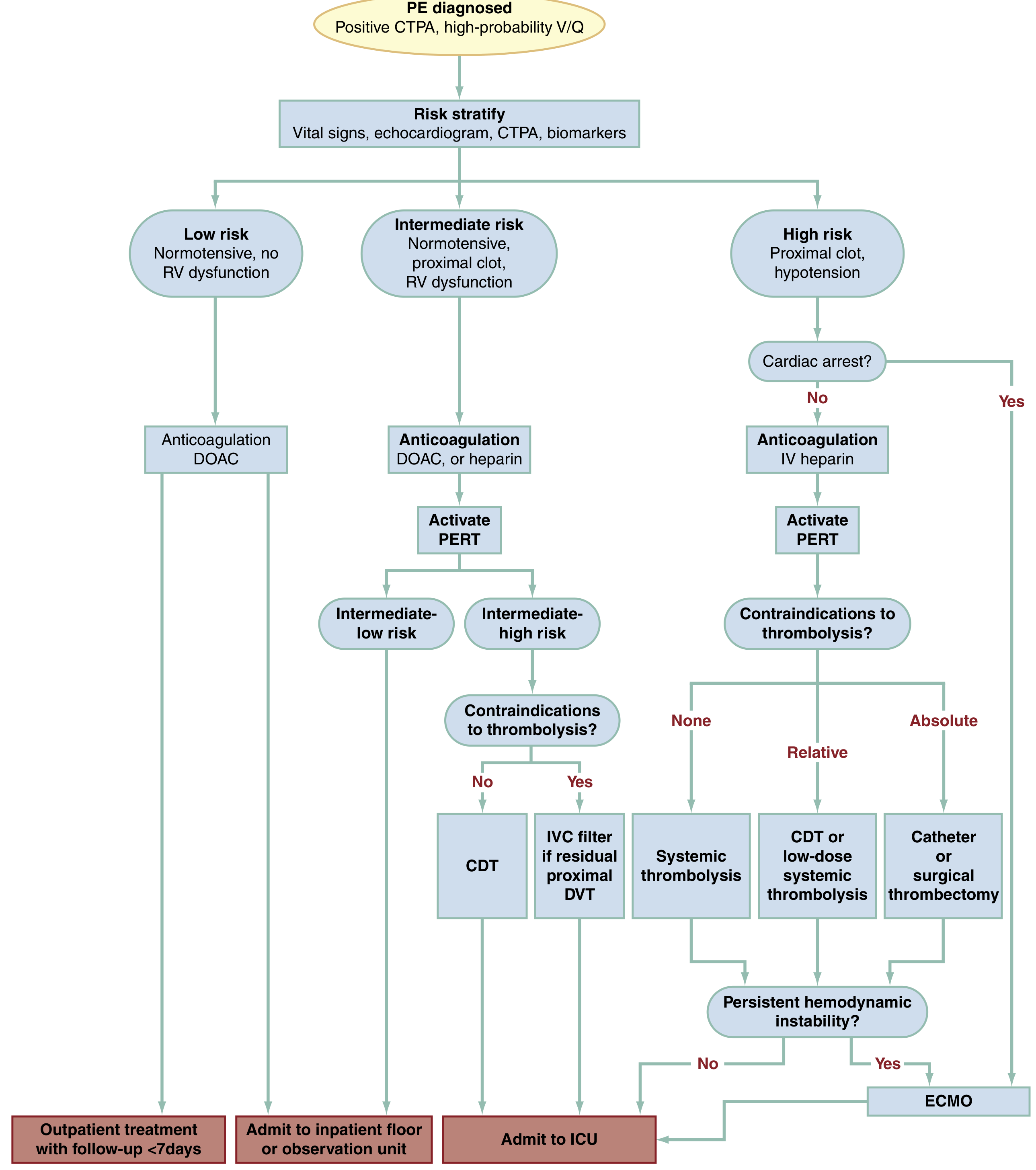
PE Management Algorithm - Rosen's Emergency Medicine, 10e. High-risk PE patients: if no cardiac arrest and no contraindications → systemic thrombolysis; if relative contraindications → CDT or low-dose thrombolysis; if absolute contraindications → surgical/catheter thrombectomy; if persistent hemodynamic instability despite above → ECMO.
4a. Systemic Thrombolysis (First-Line for Massive PE)
Systemic thrombolysis is the treatment of choice for massive PE without contraindications. Thrombolytics activate plasminogen to plasmin, which degrades fibrin within the thrombus.
Dosing Regimens:
| Agent | Dose | Route |
|---|---|---|
| Alteplase (rtPA) - standard | 100 mg IV over 2 hours | IV infusion |
| Alteplase - low dose | 25-50 mg IV over 2 hours | IV infusion |
| Reteplase | 10 units IV bolus, repeated at 30 min | IV bolus ×2 |
| Tenecteplase | Single weight-based bolus over 5-10 seconds | IV bolus |
Alteplase has a half-life of ~5 minutes (cleared hepatically); during infusion, plasma concentrations reach 300-3000 ng/mL, which degrades systemic fibrinogen. Reteplase and tenecteplase offer longer half-lives and convenient bolus dosing, with similar efficacy and toxicity to alteplase.
Efficacy: Thrombolysis reduces mortality and hemodynamic collapse but carries a 2-4% major hemorrhage rate and up to 1% intracranial hemorrhage rate.
Absolute Contraindications to Thrombolysis:
- GI bleeding within the previous 30 days
- Active hemorrhage (intraperitoneal, retroperitoneal, pulmonary, uterine, bladder, nasal)
- Recent intracranial surgery or head trauma
- Intracranial neoplasm or brain metastasis
- History of hemorrhagic stroke
- Aortic dissection
- Liver failure (INR >1.7)
- Surgery requiring opening of the chest, peritoneum, skull, or spinal canal within the previous 14 days
- Subacute bacterial endocarditis under treatment
- Pregnancy
- Large pericardial effusion
Relative Contraindications:
- Age >75 years; dementia
- Surgery 30-60 days prior; any prior stroke
- Symptoms suggesting TIA in past 30 days
- Any prior GI bleeding; concurrent thienopyridine use (e.g., clopidogrel)
- INR >1.7 from warfarin; metastatic cancer
- Recent fracture, head strike, hematuria, dental extraction, or orthopedic surgery
Note: In cardiac arrest from PE, thrombolytics can and should be given despite standard CPR activity - this is not a contraindication in the arrest setting.
4b. Catheter-Directed Thrombolysis (CDT)
CDT delivers a lower dose of thrombolytic directly into the thrombus via a catheter positioned in the pulmonary artery, reducing systemic drug exposure and potentially lowering hemorrhagic risk. It is preferred when patients have:
- Relative contraindications to systemic thrombolysis
- Intermediate-high risk PE requiring advanced intervention
- Failed systemic thrombolysis
Ultrasound-assisted CDT (e.g., the EKOS system) uses high-frequency, low-power ultrasound to facilitate drug penetration. The SEATTLE II study and subsequent meta-analyses support its safety and efficacy in intermediate and high-risk PE, though head-to-head comparisons with systemic thrombolysis in truly massive PE are limited.
4c. Surgical Embolectomy
Surgical pulmonary embolectomy is performed via median sternotomy on cardiopulmonary bypass. It is indicated for:
- Massive PE with absolute contraindications to thrombolysis
- Failed thrombolysis with persistent hemodynamic compromise
- Presence of intracardiac thrombus or patent foramen ovale (PFO) with paradoxical embolism risk
Perioperative mortality is highest in patients who require CPR before surgery and lowest in patients who are stabilized beforehand. Importantly:
- Placing an IVC filter before surgery in stable patients reduces operative mortality
- Prior thrombolytic administration does not absolutely preclude surgery - patients can undergo sternotomy after thrombolytics and survive without fatal hemorrhage, but this decision rests with the cardiothoracic surgeon
Emergency physicians should involve an experienced cardiothoracic surgeon as early as possible in the care of potential embolectomy patients.
4d. Percutaneous Mechanical Thrombectomy (Aspiration/Fragmentation)
Catheter-based mechanical devices allow aspiration or fragmentation of clot without thrombolytics. Options include:
- Aspiration thrombectomy (e.g., FlowTriever, Indigo system)
- Ultrasound-assisted CDT
A 2025 systematic review and meta-analysis (Choksi et al., PMID 39365670) compared aspiration thrombectomy vs. ultrasound-accelerated thrombolysis, supporting both techniques in appropriate patients.
4e. Extracorporeal Membrane Oxygenation (ECMO)
ECMO - particularly veno-arterial ECMO (VA-ECMO) - serves as:
- A bridge to definitive therapy (CDT, surgical embolectomy, or catheter thrombectomy)
- A rescue strategy for refractory hemodynamic instability despite all other interventions
ECMO unloads the right ventricle and restores cardiac output while the thrombus is treated. Survival of PE patients requiring ECMO is approximately 70%. ECMO requires institutional infrastructure and specialized expertise, limiting its availability to tertiary centers. Extracorporeal CPR (ECPR) also enables resuscitation of cardiac arrest from PE at centers where it is available.
5. Pulmonary Embolism Response Teams (PERT)
PERTs are multidisciplinary rapid-response teams including emergency physicians, cardiologists, pulmonologists, vascular/cardiothoracic surgery, and interventional radiology. Key points:
- ~60% of PERT activations originate in the ED
- PERTs facilitate access to advanced therapies (CDT, surgery, ECMO) and reduce disposition times
- Current guidelines recommend PERT activation for all intermediate-high and high-risk PE patients
- Activate PERT early - do not wait for hemodynamic deterioration to call for help
6. IVC Filters
IVC filter placement is indicated in a narrow subset:
- Confirmed PE with an absolute contraindication to anticoagulation (e.g., recent cerebral hemorrhage, large cerebral infarction, brain metastases)
- Central PE in a patient unlikely to survive embolization of a proximal (iliofemoral) mobile DVT
Retrievable filters are preferred. Contact interventional radiology/cardiology urgently for placement in these scenarios.
7. Cardiac Arrest Management in PE
- PEA is the most common arrest rhythm
- If PE is suspected as the cause of PEA, give empirical thrombolysis (alteplase 50 mg IV bolus)
- Continue CPR for at least 60-90 minutes after thrombolytic administration before considering cessation - thrombolytics take time to work
- If available, ECPR/VA-ECMO should be deployed during or after resuscitation
8. Summary of Priorities
| Priority | Action |
|---|---|
| Airway | O₂ to SpO₂ >90%; avoid intubation if possible |
| Hemodynamics | Cautious fluids (250-500 mL boluses); norepinephrine; dobutamine as adjunct |
| Anticoagulation | IV UFH immediately |
| Reperfusion | Systemic alteplase 100 mg/2h if no contraindications |
| If contraindicated | CDT, surgical embolectomy, or mechanical thrombectomy |
| Refractory shock | ECMO as bridge to definitive therapy |
| Team activation | PERT immediately for high-risk PE |
Recent Evidence Updates (2023-2026)
- ACR Appropriateness Criteria 2025 (PMID 41193046) and 2025 ESVM Guidelines (PMID 40587333) both support catheter-directed interventions as valid alternatives to systemic thrombolysis in high-risk PE, particularly when bleeding risk is elevated.
- A 2025 meta-analysis (Choksi et al., PMID 39365670) found that aspiration thrombectomy and ultrasound-accelerated thrombolysis had comparable safety and efficacy - supporting the role of catheter-based strategies alongside traditional thrombolysis.
- The trend in 2024-2026 guidelines is toward earlier PERT activation and more individualized decisions using catheter-based therapy, rather than defaulting to systemic thrombolysis for all massive PE patients.
Sources: Rosen's Emergency Medicine: Concepts and Clinical Practice, 10e; Tintinalli's Emergency Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics; Murray & Nadel's Textbook of Respiratory Medicine; Miller's Anesthesia, 10e; ACR/ESVM Guidelines 2025.
1.Explain interpretation of general urinalysis in renal pathology.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from all major nephrology textbooks. Let me compile the full, detailed answer.
Interpretation of General Urinalysis in Renal Pathology
Urinalysis is often called the "liquid biopsy of the kidney." It provides diagnostic and prognostic information that complements serum markers (creatinine, eGFR), and in many conditions it is the earliest indicator of renal disease - appearing before any decline in GFR is detected. A complete urinalysis has three components: macroscopic assessment, dipstick (chemical) analysis, and microscopic examination of urine sediment.
PART 1 — MACROSCOPIC ASSESSMENT
1a. Urine Color
Normal urine is pale to deep yellow, colored by urochrome. Color changes carry important diagnostic clues:
| Color | Cause | Pathologic Significance |
|---|---|---|
| Pink/Red | Gross hematuria, hemoglobinuria, myoglobinuria | Glomerulonephritis, rhabdomyolysis, tumor |
| Red urine + red sediment | Intact RBCs | Hematuria (glomerular or urological) |
| Red urine + clear sediment | Free hemoglobin or myoglobin | Intravascular hemolysis; rhabdomyolysis |
| Brown/cola-colored | Heme pigments, hemosiderin | Hemolysis; myoglobinuria; severe glomerulonephritis |
| Yellow-brown | Bilirubin | Jaundice; hepatorenal syndrome |
| White/milky | Pyuria, chyluria, lipiduria | UTI; nephrotic syndrome (lipiduria) |
| Colorless | Dilute urine (low osmolality) | Diabetes insipidus; overhydration |
Key clinical point: Red urine in the absence of RBCs on microscopy indicates hemoglobinuria (serum is pink) or myoglobinuria (serum is clear). Myoglobin casts indicate AKI from rhabdomyolysis.
1b. Urine Odor
- Ammonia: bacterial infection (urease-producing organisms)
- Fruity/sweet: ketonuria (DKA, starvation)
- Mousy: phenylketonuria
- Maple syrup: maple syrup urine disease
- Fishy: hypermethioninemia; trimethylaminuria
1c. Turbidity/Clarity
Normal urine is clear. Cloudy urine is most commonly due to leukocytes and bacteria (UTI/pyelonephritis). It may also result from phosphate crystals (alkaline urine), urate crystals (acidic urine), or lipiduria in nephrotic syndrome.
PART 2 — DIPSTICK (CHEMICAL) ANALYSIS
2a. Specific Gravity (SG) and Osmolality
- Normal SG: 1.003-1.030
- SG of 1.001-1.003 = isosthenuria (inability to concentrate) - seen in chronic kidney disease (CKD), diabetes insipidus
- SG 1.008-1.010 = isosthenuric range (equal to plasma osmolality ~280 mOsmol/kg)
- High SG (>1.020): dehydration, prerenal azotemia, SIADH, glucosuria (glucose adds to weight but not ionic strength, causing discrepancy between dipstick and refractometry)
- Fixed SG of 1.010: loss of tubular concentrating and diluting ability; hallmark of end-stage renal disease
Osmolality is the gold standard for concentration. Urine SG rises ~0.001 per 35-40 mOsmol/kg increase in osmolality. SG ≤1.003 by refractometry always indicates maximally dilute urine (≤100 mOsmol/kg).
2b. Urine pH
- Normal range: 4.5 to 7.8
- Alkaline urine (>7.0): infection with urease-producing organisms (Proteus mirabilis, Ureaplasma), renal tubular acidosis type I (distal), metabolic alkalosis
- Acidic urine (<5.5): metabolic acidosis, uric acid crystals/stones
- Persistently alkaline despite systemic acidosis: distal RTA (inability to acidify urine below pH 5.5)
2c. Protein
- Normal: <150 mg/day of total protein; <30 mg/day of albumin
- Dipstick detects: primarily albumin; threshold ~200-300 mg/L (trace = 15-30 mg/dL)
- Dipstick can be falsely positive with: concentrated urine, alkaline pH, hematuria, antiseptic contamination
- Dipstick can be falsely negative for: low-molecular-weight (LMW) proteins (light chains in myeloma, β2-microglobulin in tubular disease)
Types and clinical interpretation:
| Type | Mechanism | Examples | Level |
|---|---|---|---|
| Glomerular | Loss of size/charge selectivity | GN, diabetic nephropathy, FSGS | Often >1 g/day; albumin-predominant |
| Tubular | Impaired proximal reabsorption of LMW proteins | Fanconi syndrome, Dent disease, cisplatin toxicity | Usually <2 g/day; non-albumin proteins |
| Overflow | Excess production exceeds resorption capacity | Myeloma (Bence-Jones), rhabdomyolysis, hemolysis | Variable |
| Postrenal | Inflammation in urinary tract | UTI, stones | Small amounts; nonalbumin IgG/IgA |
KDIGO Albuminuria Categories (Brenner & Rector's, 2022):
| Category | AER (mg/24h) | ACR (mg/g) | Significance |
|---|---|---|---|
| A1 (Normal-mild) | <30 | <30 | Normal or early marker |
| A2 (Moderately increased) | 30-300 | 30-300 | Historically "microalbuminuria"; earliest CKD/DM marker |
| A3 (Severely increased) | >300 | >300 | Overt nephropathy; nephrotic range if >3.5 g/day |
Nephrotic-range proteinuria: >3.5 g/day in adults; >40 mg/m²/h in children. Associated with: edema, hypoalbuminemia, hyperlipidemia, lipiduria.
Albuminuria is now a KDIGO criterion for CKD staging and is a stronger predictor of progression to ESKD and cardiovascular mortality than eGFR alone.
2d. Glucose (Glucosuria)
- Normally absent (glucose is fully reabsorbed by SGLT2 in the proximal tubule)
- With normal blood glucose (euglycemic glucosuria): proximal tubule defect - Fanconi syndrome, SGLT2 inhibitor therapy, hereditary renal glucosuria
- With hyperglycemia: exceeds tubular threshold (~180 mg/dL) - diabetes mellitus
- Clinical pearl: glucosuria in the absence of hyperglycemia is a key finding of Fanconi syndrome (tubular dysfunction)
2e. Blood / Hemoglobin
The dipstick detects both intact RBCs and free hemoglobin/myoglobin by peroxidase activity.
- Positive dipstick + RBCs on microscopy = true hematuria
- Positive dipstick + no RBCs = hemoglobinuria or myoglobinuria
- False positives: myoglobin, oxidizing agents, bacterial peroxidase, povidone-iodine
- False negatives: high vitamin C concentration
2f. Leukocyte Esterase and Nitrites
- Leukocyte esterase (+): pyuria (>5 WBC/hpf); indicates infection, AIN, or glomerulonephritis
- Nitrites (+): nitrate-reducing bacteria (Gram-negatives); specific for bacterial UTI but not sensitive
- Sterile pyuria (positive leukocyte esterase, negative nitrites, negative culture): tuberculosis, AIN, interstitial nephritis, papillary necrosis, contamination
2g. Ketones
Detected when ketoacidosis is present (DKA, starvation, alcoholic ketoacidosis). Dipstick primarily detects acetoacetate, not beta-hydroxybutyrate (may underestimate severity).
2h. Bilirubin and Urobilinogen
- Bilirubin (+): conjugated hyperbilirubinemia; hepatocellular disease or obstructive jaundice
- Urobilinogen (elevated): hepatocellular disease, hemolytic anemia
PART 3 — URINE MICROSCOPY (SEDIMENT EXAMINATION)
Urine microscopy is often called the "most important and most underutilized" diagnostic tool in nephrology. Casts are pathognomonic of renal origin; they form in the tubular lumen when Tamm-Horsfall glycoprotein (uromodulin, secreted by the thick ascending limb of Henle) aggregates and traps cells, debris, or protein within the tubule.
Key principle: Casts are the only formed elements of urine that originate exclusively in the kidney.
3a. Red Blood Cells (Erythrocytes)
Normal: 0-2 RBCs/hpf; >3 RBCs/hpf is abnormal (microscopic hematuria).
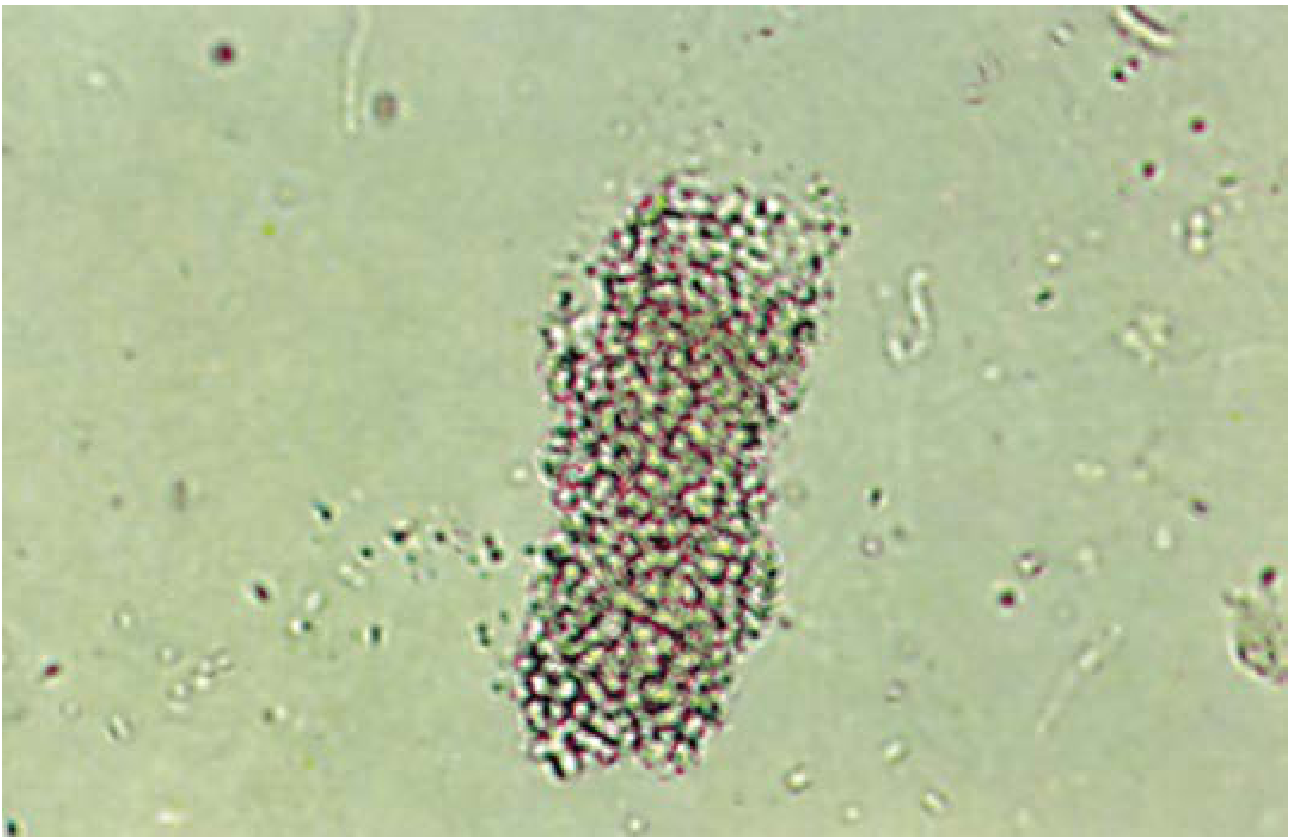
Isomorphic RBCs (uniform biconcave discs, similar to circulating RBCs):
- Indicate non-glomerular bleeding: urological source (tumor, stones, cystitis, trauma, prostatitis)
- RBCs may appear crenated in hypertonic urine or as "ghost cells" in dilute urine
Dysmorphic RBCs (irregular contours, blebs, fragmentation from osmotic and pH changes as cells traverse the tubule):
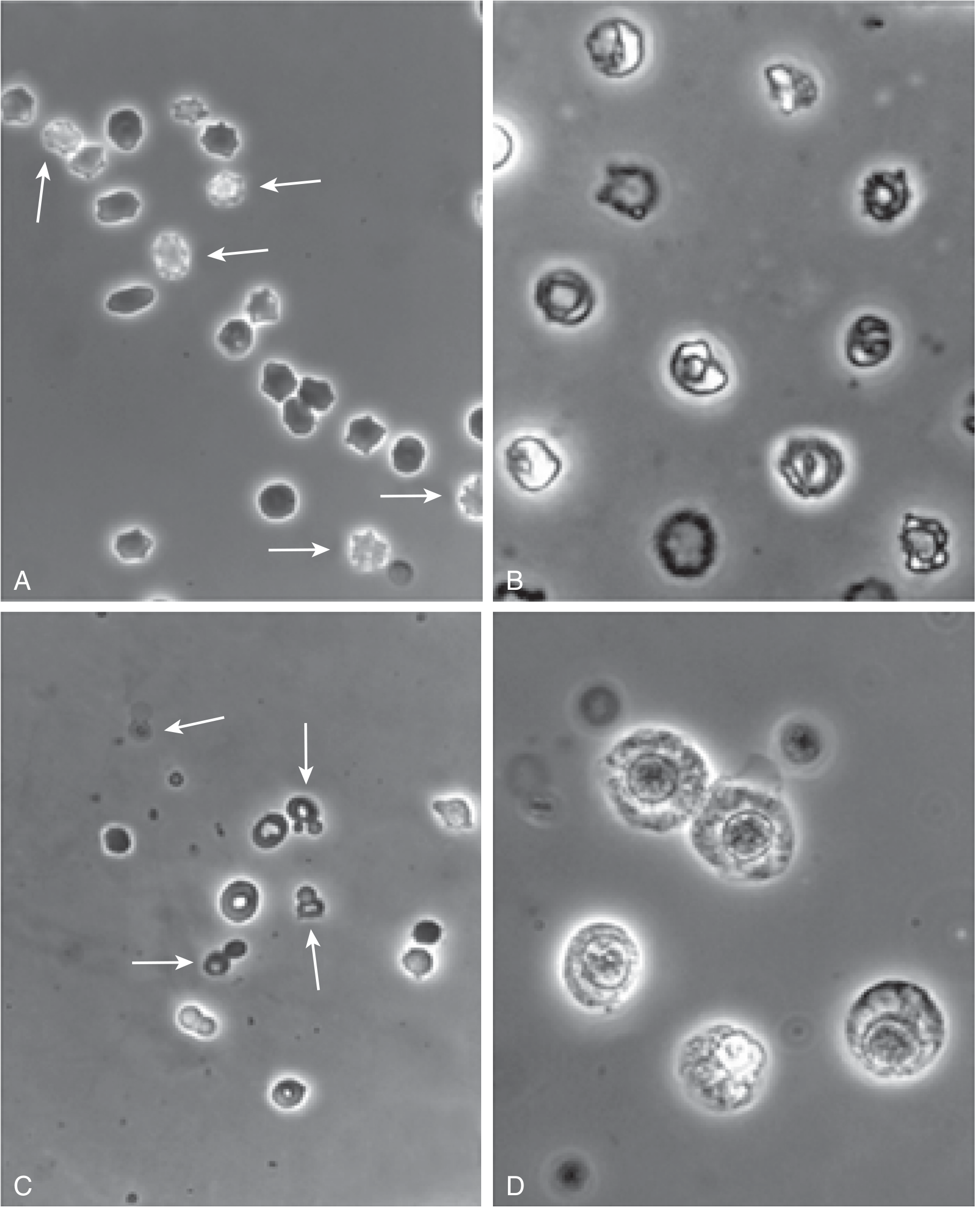
Urine erythrocytes: (A) Isomorphic RBCs with some crenation. (B) Dysmorphic RBCs. (C) Acanthocytes (G1 cells) with membrane blebs - specific for glomerular hematuria. (D) WBCs for comparison. (Brenner & Rector's The Kidney)
- Indicate glomerular origin (passage through damaged GBM causes deformation)
- Acanthocytes (G1 cells): doughnut shape with membrane blebs; most specific for glomerular hematuria
- Generally >10-80% dysmorphic RBCs (threshold varies by institution) = glomerular source
- RBC casts + dysmorphic RBCs = pathognomonic of glomerulonephritis
Clinical significance of hematuria:
- Persistent microscopic hematuria (≥3 RBCs/hpf on ≥2 samples) warrants investigation
- Associated with 19.5× increased hazard for ESKD in long-term follow-up studies
- Warfarin-induced nephropathy: over-anticoagulation → glomerular RBC cast formation → tubular obstruction → AKI
3b. White Blood Cells (Leukocytes)
Normal: 0-5 WBCs/hpf
| Finding | Interpretation |
|---|---|
| Pyuria with bacteria | UTI / pyelonephritis |
| Pyuria without bacteria (sterile pyuria) | AIN, TB, NSAID nephropathy, papillary necrosis |
| Leukocyte casts | Pyelonephritis or acute interstitial nephritis |
| Eosinophiluria | Classically described in drug-induced AIN (low sensitivity/specificity) |
3c. Renal Tubular Epithelial Cells (RTECs)
RTECs are larger than WBCs, with eccentric nuclei. They are the hallmark cells of tubular injury.
- RTECs + granular casts + epithelial casts = acute tubular necrosis (ATN) - the hallmark triad
- RTECs are rarely seen in prerenal AKI (where hyaline casts predominate)
- Scoring systems based on RTEC/granular cast counts predict AKI progression, dialysis need, and death
- Decoy cells: RTECs infected with BK polyomavirus, showing characteristic ground-glass nuclei (see figure below) - important in renal transplant recipients
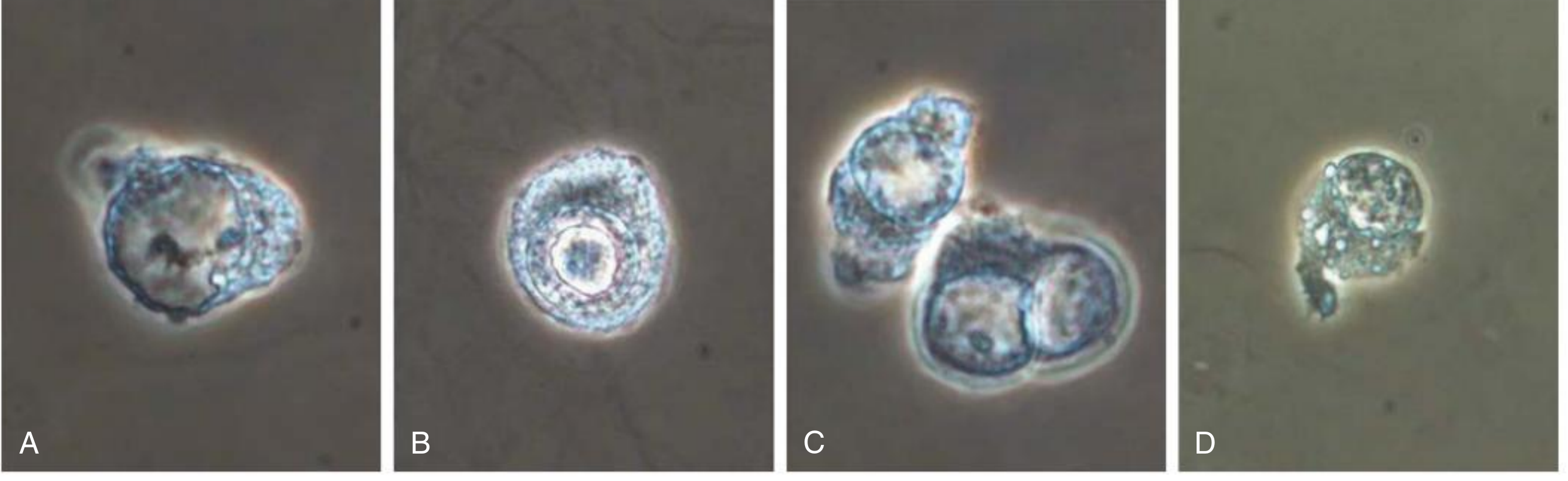
Decoy cells in urine: (A) Ground-glass nucleus (phenotype 1). (B) CMV-like intranuclear inclusion (phenotype 2). (C) Binucleated cell. (D) Clumped chromatin (phenotype 4). Seen in BK virus nephropathy in transplant recipients. (Comprehensive Clinical Nephrology, 7e)
PART 4 — URINARY CASTS
Casts form when Tamm-Horsfall protein precipitates under conditions of:
- Low tubular flow (stasis)
- Acidic pH
- High ionic concentration
- Increased protein load
Cast width reflects the tubular diameter: broad casts form in dilated tubules or collecting ducts and indicate severe, widespread tubular damage - a poor prognostic sign.
Cast Types and Clinical Significance:
| Cast Type | Appearance | Clinical Meaning |
|---|---|---|
| Hyaline | Pale, translucent; nearly invisible on bright-field | Normal in small numbers; increases with dehydration, diuretics, fever, exercise, prerenal azotemia |
| Granular | Coarse or fine granules from degenerated cells | Nonspecific tubular injury; ATN (with RTECs); CKD |
| Waxy | Dense, refractile, brittle-looking; high RI | Advanced/chronic renal disease; tubular stasis |
| Fatty | Contains fat droplets; Maltese cross under polarized light | Nephrotic syndrome (massive proteinuria + lipiduria) |
| RBC (erythrocyte) | Contains RBCs; red-orange color | Always pathologic: glomerulonephritis; vasculitis |
| WBC (leukocyte) | Contains neutrophils | Pyelonephritis; acute interstitial nephritis |
| Epithelial | Contains RTECs | ATN; severe tubular injury |
| Hemoglobin/pigment | Yellow-red to brown; pigmented | Severe glomerulonephritis; intravascular hemolysis; rhabdomyolysis |
| Myoglobin | Red-brown | AKI due to rhabdomyolysis |
| Broad/Waxy | 2-6× normal width; waxy | Severe CKD; dialysis-grade disease; poor prognosis |
Granular cast (×200) - a hallmark of acute tubular necrosis in combination with RTECs and epithelial casts. (Henry's Clinical Diagnosis and Management, 23e)
Red cell casts are ALWAYS pathologic and indicate significant glomerular pathology. (Brenner & Rector's The Kidney)
PART 5 — CRYSTALS
Crystals are identified by their shape, color, and solubility characteristics.
| Crystal | Appearance | Clinical Significance |
|---|---|---|
| Calcium oxalate (monohydrate) | Envelope/dumbbell-shaped | Calcium oxalate nephrolithiasis; ethylene glycol poisoning (needle-shaped monohydrate) |
| Uric acid | Yellow-brown rhomboids/rosettes; soluble in alkali | Urate nephropathy; gout; tumor lysis syndrome |
| Triple phosphate (struvite) | Coffin-lid shaped | UTI with urease-producing organisms; staghorn calculi |
| Cystine | Hexagonal flat plates | Cystinuria (pathognomonic) |
| Calcium phosphate | Prism-shaped | Nephrocalcinosis; distal RTA |
| Bilirubin | Yellow needle clusters | Bilirubinuria |
Massive uric acid crystalluria in the setting of tumor lysis syndrome causes acute urate nephropathy with AKI and pink (uric acid) discoloration of urine.
PART 6 — URINE SEDIMENT PROFILES IN SPECIFIC RENAL DISEASES
The following table synthesizes findings into diagnostic profiles (Comprehensive Clinical Nephrology, 7e):
| Disease | Hallmark Finding | Associated Features | Proteinuria |
|---|---|---|---|
| Prerenal AKI | Hyaline ± hyaline-granular casts | High SG, low pH | Absent or minimal |
| Acute Tubular Necrosis (ATN) | RTECs + epithelial casts + granular casts | Pigmented casts (if hemolysis/myolysis) | Absent to + |
| Acute Interstitial Nephritis (AIN) | Leukocytes + isomorphic RBCs | RTECs, leukocyte casts, RBC casts | Absent to + |
| Active Proliferative GN | Dysmorphic RBCs (30-100+/hpf) + RBC/hemoglobin casts | Leukocytes, RTECs, waxy casts | + to ++++ |
| Nephrotic Syndrome | Fatty casts + fat oval bodies + "Maltese cross" | RTECs, hyaline/granular casts; few RBCs | ++++ (>3.5 g/day) |
| Urinary Tract Infection | Bacteria + leukocytes | Transitional cells, struvite crystals (if urease) | Absent |
| Pyelonephritis | Leukocyte casts + RTECs | Bacteria, leukocytes | Absent to trace |
| Urological disease | Isomorphic RBCs | Transitional/malignant cells; crystals | Absent |
| BK virus nephropathy | Decoy cells | Decoy cell casts, macrophages | Absent |
| Rhabdomyolysis | Myoglobin casts (red-brown) | No RBCs on microscopy; dipstick positive | Trace |
| Advanced CKD | Broad waxy casts ("renal failure casts") | All cast types; low SG, isosthenuria | Variable |
"Telescoped Sediment"
This term describes the simultaneous presence of both nephritic (RBC casts, dysmorphic RBCs) and nephrotic (fatty casts, oval fat bodies) elements in the same specimen. It is classically seen in:
- Lupus nephritis (Class IV/V)
- IgA nephropathy with nephrotic features
- Membranoproliferative GN
- Rapidly progressive GN
PART 7 — SUMMARY: KEY CLINICAL INTERPRETIVE PRINCIPLES
- RBC casts - always abnormal; point to glomerular disease (GN, vasculitis, lupus)
- Dysmorphic RBCs - glomerular bleeding; when >10-80% of RBCs are dysmorphic, suspect GN
- RTECs + granular casts - ATN; score correlates with dialysis need and mortality
- Leukocyte casts - AIN or pyelonephritis; sterile pyuria suggests AIN or TB
- Fatty casts + lipiduria - nephrotic syndrome; look for Maltese cross under polarized light
- Broad/waxy casts - advanced CKD; dialysis-level nephron loss; poor prognosis
- High proteinuria (>3.5 g/day) + normal sediment - minimal change disease or membranous nephropathy
- Isosthenuria (SG fixed at 1.010) - loss of tubular concentrating ability; ESKD or severe CKD
- Glucosuria with normo-glycemia - proximal tubular dysfunction (Fanconi syndrome)
- Cystine crystals - pathognomonic for cystinuria
- Uric acid crystals in quantity + AKI - tumor lysis syndrome / acute urate nephropathy
- Decoy cells in transplant recipient - BK polyomavirus nephropathy; screen with viral PCR
Sources: Brenner and Rector's The Kidney, 11e; Comprehensive Clinical Nephrology, 7e; Henry's Clinical Diagnosis and Management by Laboratory Methods, 23e; Tietz Textbook of Laboratory Medicine, 7e; Goldman-Cecil Medicine
What is cardio genic hypertension and how is it different from pulmonary hypertension?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
cardiogenic hypertension definition cardiac output systemic blood pressure mechanism
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have all the content needed for a complete, authoritative answer. Let me compile it.
"Cardiogenic Hypertension" vs. Pulmonary Hypertension
Important Clarification First
"Cardiogenic hypertension" is not a formally recognized or standard clinical diagnosis in any major cardiovascular, respiratory, or nephrology textbook. A search across the entire medical library returns zero results for this term as a standalone condition. This is important to flag because using unrecognized terminology in clinical practice can cause confusion.
However, the concept it describes is real and well-established - it refers to a mechanism of systemic hypertension driven by elevated cardiac output (CO), as opposed to the more common mechanism of elevated systemic vascular resistance (SVR). Understanding this requires first understanding the fundamental equation of blood pressure:
Blood Pressure (BP) = Cardiac Output (CO) × Systemic Vascular Resistance (SVR)
So elevated BP can arise from either limb of this equation - or both.
Part 1: What "Cardiogenic Hypertension" Actually Means
Since BP = CO × SVR, hypertension can be driven by:
Mechanism A: High Cardiac Output (the "Cardiogenic" / High-Output Mechanism)
This is what "cardiogenic hypertension" most likely refers to. It describes systemic hypertension that arises primarily from an elevated cardiac output (increased heart rate or stroke volume), rather than from increased peripheral resistance.
The NKF Primer on Kidney Diseases (8e) explains:
"Essential hypertension developing in young adults may be initiated by an increase in cardiac output, associated with signs of overactivity of the sympathetic nervous system; the blood pressure (BP) is labile, and the heart rate is increased. Later, the BP increases further because of a rise in SVR, with return to a normal cardiac output."
And from Medscape/Emedicine on hypertension pathophysiology:
"Younger individuals may present with hypertension associated with an elevated cardiac output (high-output hypertension). High-output hypertension results from volume and sodium retention by the kidney, leading to increased stroke volume and, often, with cardiac stimulation by adrenergic hyperactivity. Systemic vascular resistance is generally not increased at such earlier stages."
Causes of high-output (cardiogenic mechanism) hypertension:
| Condition | Mechanism |
|---|---|
| Early essential hypertension in young adults | Sympathetic overactivity → increased HR and CO |
| Volume overload states (heart failure with preserved EF, renal salt retention) | Frank-Starling increase in stroke volume → raised CO |
| Hyperthyroidism | Increased HR + contractility → elevated CO |
| Anemia (chronic) | Compensatory increase in CO |
| Arteriovenous fistula / AV malformation | Increased venous return and CO |
| Aortic coarctation | Upstream high CO + structural obstruction → proximal hypertension |
| Preeclampsia | Expanded blood volume + tachycardia → elevated CO |
| Pheochromocytoma | Catecholamine excess → increased HR, contractility, and CO |
| Obesity | Expanded blood volume → increased CO (SVR actually falls initially) |
The natural history of high-output hypertension, if untreated, is that the sustained high pressure triggers vascular remodeling (hypertrophy and stiffening of arteriolar walls), which progressively raises SVR. Over time, CO normalizes or even falls, but SVR becomes the dominant driver - transitioning into the more typical sustained hypertension pattern with elevated SVR.
Mechanism B: High Systemic Vascular Resistance (the more common mechanism)
Most clinical hypertension in adults is driven by elevated SVR from:
- Renal mechanisms (RAAS activation, salt retention)
- Structural vascular remodeling
- Endothelial dysfunction
- Autonomic dysregulation
In established hypertension, CO is typically normal or slightly reduced, while SVR is elevated.
Why Is "Cardiogenic Hypertension" Not a Standard Term?
Because:
- High-output hypertension is the preferred, more precise term
- "Cardiogenic" usually refers to something caused by cardiac failure (e.g., cardiogenic shock = low output), so calling hypertension "cardiogenic" is terminologically confusing and potentially misleading
- The cardiac output mechanism is just one part of how secondary hypertension is classified - the standard classification is by etiology (renovascular, endocrine, primary, etc.), not by hemodynamic mechanism
Part 2: Pulmonary Hypertension - Definition and Classification
Pulmonary hypertension (PH) is a completely separate condition from systemic hypertension. It is defined as abnormally elevated pressure in the pulmonary arterial circulation, and it affects the right heart, not the systemic (left-heart driven) circulation.
Hemodynamic Definition (Updated 2022 ESC/ERS Guidelines)
Per Murray & Nadel's Textbook of Respiratory Medicine and Grainger & Allison's Diagnostic Radiology:
| Type | mPAP | PCWP/PAWP | PVR | Groups |
|---|---|---|---|---|
| Pulmonary Hypertension (any) | ≥20-25 mmHg | - | - | All WHO groups |
| Pre-capillary PH | ≥20 mmHg | ≤15 mmHg | >3 Wood units | Groups 1, 3, 4, 5 |
| Isolated post-capillary PH | ≥20 mmHg | >15 mmHg | ≤3 Wood units | Group 2 (left heart disease) |
| Combined pre- + post-capillary PH | ≥20 mmHg | >15 mmHg | >3 Wood units | Group 2 with vascular remodeling |
mPAP = mean pulmonary arterial pressure; PCWP = pulmonary capillary wedge pressure; PVR = pulmonary vascular resistance
WHO Classification of Pulmonary Hypertension (5 Groups)
| WHO Group | Category | Examples |
|---|---|---|
| Group 1 | Pulmonary Arterial Hypertension (PAH) | Idiopathic (IPAH), heritable, drug/toxin-induced, connective tissue disease, HIV, congenital heart disease, schistosomiasis |
| Group 2 | PH due to left heart disease | HFrEF, HFpEF, valvular disease (mitral stenosis, aortic stenosis) |
| Group 3 | PH due to lung disease or hypoxia | COPD, ILD, sleep-disordered breathing, altitude |
| Group 4 | Chronic thromboembolic PH (CTEPH) | Unresolved PE → organized thrombus → fixed obstruction |
| Group 5 | PH with unclear/multifactorial mechanisms | Sarcoidosis, histiocytosis, metabolic disorders |
Part 3: Key Differences - Cardiogenic (High-Output) Hypertension vs. Pulmonary Hypertension
| Feature | High-Output ("Cardiogenic") Systemic Hypertension | Pulmonary Hypertension |
|---|---|---|
| Circulation affected | Systemic (left-sided) | Pulmonary (right-sided) |
| Pressure elevated | Systemic arterial BP (>140/90 mmHg) | Mean pulmonary arterial pressure (>20-25 mmHg) |
| Mechanism | Elevated cardiac output (CO), then SVR | Elevated pulmonary vascular resistance (PVR) or left heart back-pressure |
| Ventricle overloaded | Left ventricle (increased afterload) | Right ventricle (increased afterload) |
| Vascular beds involved | Aorta, peripheral arteries (systemic) | Pulmonary arteries, arterioles, capillaries |
| Cardiac output state | Typically HIGH (at least early on) | Often LOW (especially in advanced PAH) |
| Pulmonary artery pressure | Normal | Elevated (by definition) |
| Systemic BP | Elevated | Normal or low (in advanced PH - right heart failure) |
| Key pathology | Vascular stiffening, LVH, nephrosclerosis, retinopathy | Pulmonary vascular remodeling, plexiform lesions, RV hypertrophy/failure |
| Typical symptoms | Headache, epistaxis, visual changes (in severe cases), often asymptomatic | Dyspnea on exertion, syncope, right heart failure (edema, ascites, JVD) |
| Chest pain mechanism | LV ischemia (if severe) | RV ischemia; compression of left main coronary by dilated PA trunk |
| Diagnosis | Sphygmomanometry | Right heart catheterization (definitive) |
| Treatment targets | Reduce CO excess OR SVR (ACEi, CCBs, beta-blockers, diuretics) | Pulmonary vasodilators (prostacyclins, PDE-5 inhibitors, endothelin antagonists) |
Part 4: The Important Overlap - Group 2 PH (Post-Capillary PH)
This is where things intersect: left heart disease (especially heart failure, mitral stenosis) can cause pulmonary hypertension by elevating left atrial pressure, which backs up into the pulmonary veins and capillaries, raising the pulmonary arterial pressure passively. This is called post-capillary pulmonary hypertension (WHO Group 2).
- In this setting, both systemic hypertension AND pulmonary hypertension may coexist - the systemic hypertension (often from elevated SVR in HFpEF) may be the original insult, and the pulmonary hypertension is a downstream consequence of left heart dysfunction
- This is the most common cause of PH encountered in clinical practice
- Distinction from Group 1 PAH is critical because:
- Group 1 PAH requires pulmonary vasodilators
- Group 2 PH requires treatment of the underlying left heart disease - giving pulmonary vasodilators in Group 2 can be harmful (by reducing preload, worsening LV filling)
Summary
| "Cardiogenic" (High-Output) Hypertension | Pulmonary Hypertension | |
|---|---|---|
| Is it a recognized term? | No - "high-output hypertension" is preferred | Yes - well-defined clinical entity |
| What is elevated? | Systemic BP, driven by high CO | Pulmonary arterial pressure (mPAP >20-25 mmHg) |
| Which side of the heart? | Left | Right |
| Circulatory compartment | Systemic | Pulmonary |
| Key measurement | Brachial BP cuff | Right heart catheterization |
The fundamental distinction is anatomical: systemic hypertension (regardless of whether CO- or SVR-driven) affects the systemic circulation and stresses the left ventricle, while pulmonary hypertension is confined to the pulmonary circulation and stresses the right ventricle.
Sources: NKF Primer on Kidney Diseases, 8e; Murray & Nadel's Textbook of Respiratory Medicine, 7e; Grainger & Allison's Diagnostic Radiology; Barash Clinical Anesthesia, 9e; Medscape Hypertension Pathophysiology; ESC/ERS PH Guidelines 2022
What is Nephrogenic hypertension ?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full detailed answer.
Nephrogenic (Renal) Hypertension
Definition
Nephrogenic hypertension - also called renal hypertension - is systemic arterial hypertension that arises as a direct consequence of kidney disease. The term encompasses two distinct but mechanistically related categories:
- Renovascular hypertension (RVH) - caused by reduced perfusion to the kidney due to renal artery disease
- Renal parenchymal hypertension - caused by intrinsic kidney disease (CKD, glomerulonephritis, polycystic kidneys, etc.)
Together, these represent the most common causes of secondary hypertension - i.e., hypertension with an identifiable, potentially correctable underlying cause.
Per Comprehensive Clinical Nephrology, 7e:
"Renovascular hypertension is defined as a syndrome of elevated blood pressure produced by any condition that leads to reduced perfusion of the kidneys."
The Kidney's Central Role in Blood Pressure Regulation
To understand nephrogenic hypertension, the kidney's normal role in BP control must first be understood. The kidney governs long-term BP through two master mechanisms:
1. Pressure-Natriuresis
A rise in mean arterial pressure (MAP) of just 1-3 mmHg triggers the kidney to excrete more NaCl and water - this "pressure natriuresis" directly restrains BP. Conversely, a fall in renal perfusion triggers salt and water retention, raising BP to restore renal perfusion. When this feedback loop becomes dysregulated (as in renal disease), sustained hypertension results.
2. The Renin-Angiotensin-Aldosterone System (RAAS)
The juxtaglomerular apparatus (JGA) in the kidney senses reduced perfusion pressure and releases renin, which catalyzes:
Angiotensinogen → Angiotensin I → Angiotensin II (via ACE)
↓
Vasoconstriction + Aldosterone release
↓
Na⁺/H₂O retention → ↑ blood volume → ↑ BP
As stated in NKF Primer on Kidney Diseases, 8e:
"Salt sensitivity is almost twice as frequent in patients with hypertension and is particularly common among CKD, Black persons, and the elderly... The kidney has a unique role in BP regulation. Kidney salt and water retention sufficient to increase ECF volume, blood volume, and mean circulatory filling pressure enhances venous return, cardiac output, and BP."
Part 1: Renovascular Hypertension (RVH)
Pathogenesis - The Goldblatt Model
The mechanism was established by Harry Goldblatt's landmark experiments. Reducing renal artery perfusion:
- Activates the RAAS (renin → Ang II → vasoconstriction + aldosterone)
- Activates the sympathetic nervous system
- Impairs nitric oxide generation (loss of vasodilation)
- Promotes endothelin release
- Causes hypertensive microvascular injury to the kidney
The behavior of RVH differs critically depending on whether one or both kidneys are affected:
| Model | Kidney Setup | Mechanism | BP Characteristic |
|---|---|---|---|
| 2-Kidney, 1-Clip (unilateral stenosis) | Clipped kidney + normal contralateral kidney | RAAS-driven (renin-dependent); contralateral kidney excretes excess Na⁺ | Renin-dependent; sodium-independent |
| 1-Kidney, 1-Clip (bilateral stenosis or solitary kidney) | Entire renal mass beyond stenosis | Volume-dependent; RAAS initially high but normalized; Na⁺ cannot escape | Volume-dependent; prone to azotemia, flash pulmonary edema |
Per Goldman-Cecil Medicine:
"Bilateral critical renal artery stenosis is a volume-dependent form of hypertension that, unlike unilateral renal artery stenosis, can cause azotemia."
Causes of Renovascular Hypertension
Two Main Etiologies:
1. Atherosclerotic Renal Artery Stenosis (~85% of cases)
- Affects middle-aged to older patients, more commonly men
- Typically involves the proximal renal artery near the ostia
- Associated with diffuse atherosclerosis (CAD, PVD, cerebrovascular disease)
- Risk factors: hypertension, diabetes, smoking, dyslipidemia, CKD
- Can be unilateral or bilateral
- Bilateral critical stenosis → flash pulmonary edema, recurrent heart failure, ischemic nephropathy
2. Fibromuscular Dysplasia (FMD) (~15% of cases)
- Affects younger patients (mean onset of hypertension 44.8 years; mean diagnosis age 53.3 years)
- ~80-90% of cases occur in women
- Involves the mid and distal renal artery
- Non-inflammatory, non-atherosclerotic structural dysplasia of the arterial wall
- Associated with genetic polymorphism in PHACTR1 locus (endothelin 1 regulation)
- Risk factors: cigarette smoking, hormonal influences
- Systemic: can also affect carotid, vertebral, mesenteric arteries
- May be asymptomatic; prevalence in kidney donors: 3.8-6.6%
- Classical angiographic sign: "string of beads" (alternating stenoses and aneurysms of the mid-renal artery)
"String of Beads" - CT Angiogram Image
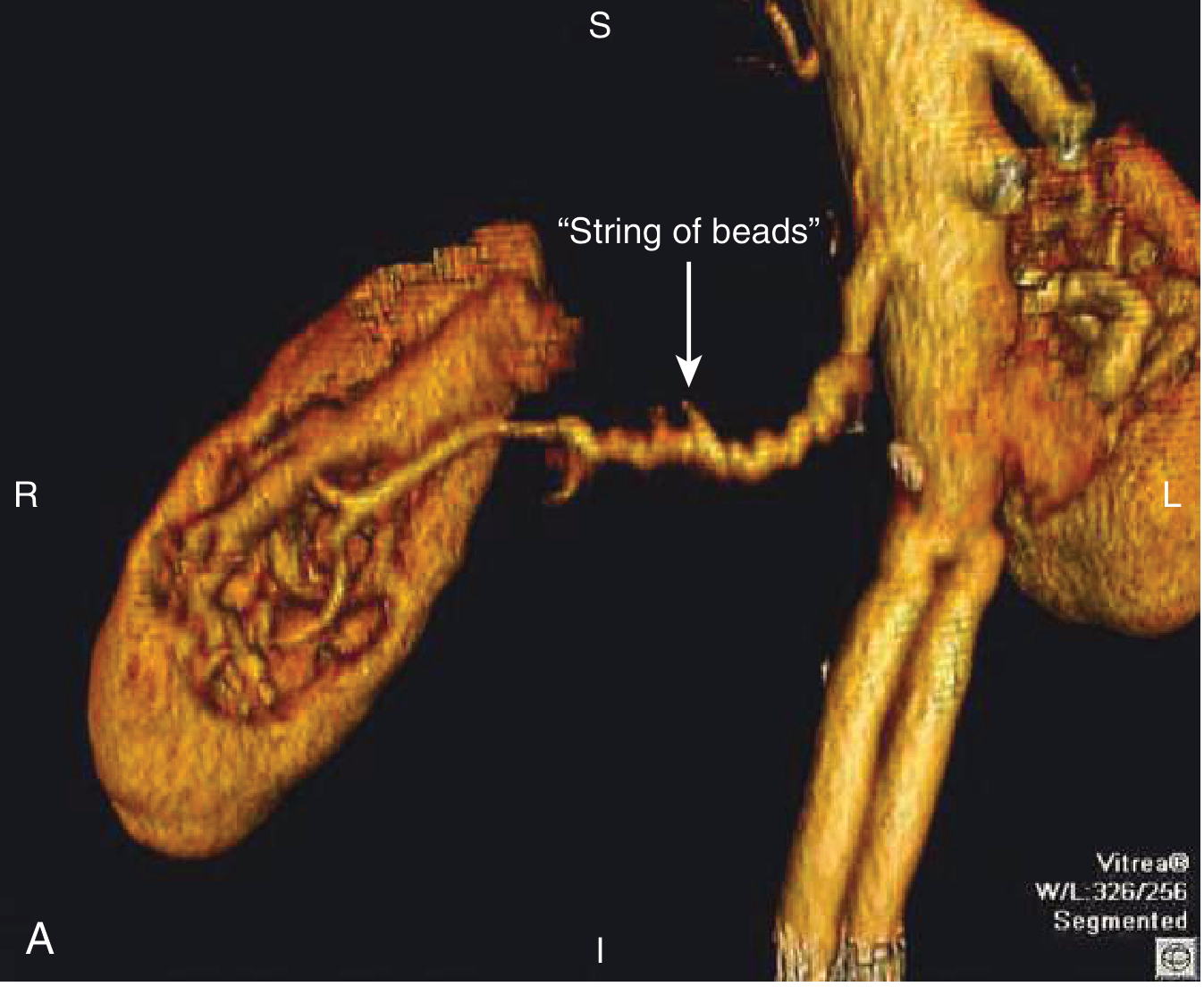
3D CT angiogram demonstrating the classical "string of beads" appearance of fibromuscular dysplasia affecting the right renal artery. (Goldman-Cecil Medicine)
Other Causes of RVH (Comprehensive Clinical Nephrology, 7e):
Two-kidney RVH (unilateral disease, contralateral kidney intact):
- Renal artery aneurysm, embolism, infarction
- Traumatic arterial occlusion
- Arteriovenous fistula
- Renal artery dissection or thrombosis
- Aortic dissection compromising renal ostium
- Page kidney (subcapsular hematoma compressing the kidney)
- Takayasu arteritis (granulomatous aortitis affecting young women)
- Neurofibromatosis
- Pheochromocytoma compressing renal artery
One-kidney RVH (bilateral disease or solitary kidney):
- Bilateral arterial stenosis or dissection
- Coarctation of the aorta
- Vasculitis involving renal arteries
- Congenital vascular anomalies
Clinical Features - When to Suspect RVH
Clinical clues that warrant screening for RVH:
| Clinical Feature | Significance |
|---|---|
| Onset of hypertension before age 30 (especially women) | Suggests FMD |
| Resistant/refractory hypertension (≥3 agents including a diuretic) | Suggests renovascular cause |
| Sudden worsening of previously controlled hypertension | New/progressive renal artery stenosis |
| Flash pulmonary edema (recurrent, unexplained) | Bilateral critical stenosis |
| Abdominal bruit (epigastric or flank) | Turbulent flow through stenotic renal artery |
| Deterioration of renal function on ACEi/ARB | High-grade bilateral stenosis or stenosis to solitary kidney |
| Unilateral small kidney on imaging | Chronic ischemic atrophy |
| Hypokalemia (without diuretics) | Secondary hyperaldosteronism |
| Advanced atherosclerosis in a young patient | Atherosclerotic RVAS |
Diagnosis
Renal artery duplex ultrasound - first-line, non-invasive screening:
- Peak systolic velocity (PSV) >200-220 cm/sec and renal-aortic ratio >3.0-3.5 = >60% stenosis
- Resistive index >0.80 = intrinsic small-vessel renal disease (poor response to intervention)
- Limitations: operator-dependent, difficult in obese patients, misses accessory vessels
CT Angiography (CTA) - excellent anatomical detail, widely available
MR Angiography (MRA) - no radiation; gadolinium-enhanced; avoid in advanced CKD (risk of nephrogenic systemic fibrosis with Group I agents, though Group II agents now considered safe)
Conventional angiography - reference standard; allows simultaneous angioplasty/stenting
Treatment
| Etiology | First-line Treatment | Notes |
|---|---|---|
| FMD | Percutaneous transluminal angioplasty (PTA) without stenting | Resolves hypertension in ~45% of cases; highly effective |
| Atherosclerotic RVAS | Medical therapy (ACEi/ARB, statins, antiplatelet, lifestyle) | Revascularization does NOT improve outcomes over medical therapy in most (ASTRAL, CORAL trials) |
| Atherosclerotic RVAS with refractory HTN, flash pulmonary edema, or ischemic nephropathy | Consider renal artery stenting/revascularization | Individualized decision |
| Takayasu arteritis | Corticosteroids/immunosuppression during active phase | Followed by interventional therapy for residual stenosis |
Key pharmacology in RVH:
- ACEi/ARBs - target RAAS, most pathophysiologically rational; preferred in unilateral RAS with intact contralateral kidney
- Caution with ACEi/ARBs in bilateral RAS or stenosis to solitary kidney - can cause acute prerenal AKI by abolishing the Ang II-driven efferent arteriolar tone that maintains GFR
- Calcium channel blockers - effective, safe alternative
- Diuretics - useful in volume-dependent (bilateral) RVH
Part 2: Renal Parenchymal Hypertension
This is even more common than RVH. Any condition damaging the renal parenchyma impairs the pressure-natriuresis mechanism and activates neurohormonal vasoconstriction.
Mechanisms:
| Mechanism | How It Raises BP |
|---|---|
| Impaired pressure-natriuresis | Damaged tubules cannot excrete Na⁺ appropriately → volume expansion → ↑ CO and BP |
| RAAS activation | Ischemic nephrons release excess renin → Ang II → vasoconstriction + aldosterone |
| Salt sensitivity | Loss of nephron mass → inability to excrete Na⁺ load → progressive volume-dependent HTN |
| Sympathetic activation | Renal afferent nerves from damaged kidney activate central sympathetic outflow |
| Reduced vasodilators | Loss of renal prostaglandins, nitric oxide; loss of bradykinin generation |
| Vascular remodeling | Progressive arteriolar hypertrophy and rarefaction → sustained elevated SVR |
Causes:
- Chronic kidney disease (CKD) of any etiology
- Glomerulonephritis (acute and chronic)
- Diabetic nephropathy
- Polycystic kidney disease (PKD)
- Reflux nephropathy / chronic pyelonephritis
- Obstructive uropathy
- Renovascular disease (overlap with RVH above)
- Renal transplant dysfunction
The CKD-Hypertension Vicious Cycle:
CKD → impaired Na⁺ excretion + RAAS activation
↓
Hypertension
↓
Glomerular hyperfiltration + hypertensive injury to residual nephrons
↓
Further nephron loss → worsening CKD
This bidirectional relationship means hypertension is both a cause and consequence of CKD. Salt sensitivity increases progressively with declining GFR, becoming near-universal in dialysis patients.
Part 3: Summary Comparison Table
| Feature | Renovascular Hypertension | Renal Parenchymal HTN |
|---|---|---|
| Primary lesion | Renal artery (stenosis/obstruction) | Kidney parenchyma (glomeruli, tubules, interstitium) |
| Main mechanism | RAAS activation from reduced renal perfusion | Impaired natriuresis + RAAS + sympathetic activation |
| Key mediator | Renin/Angiotensin II | Volume expansion + Ang II + sympathetics |
| BP type | Often severe, resistant, abrupt onset | Gradual, salt-sensitive, volume-dependent |
| Kidney size | Small on affected side (ischemic atrophy) | Often small bilaterally (CKD); may be enlarged (PKD) |
| Renal function | May be preserved or impaired | Usually impaired (proteinuria, ↑ creatinine) |
| Classic clue | Abdominal bruit; onset <30y or >55y; flash pulmonary edema | Proteinuria, hematuria, ↑ creatinine |
| Diagnosis | Renal artery duplex, CTA, MRA, angiography | Urinalysis, creatinine, GFR, renal biopsy |
| Correctable? | Often yes (FMD especially) | Partially (control BP to slow progression) |
Key Clinical Pearls
- Renovascular hypertension is the most common surgically correctable form of hypertension - identifying FMD in a young woman can be curative with PTA
- ACEi/ARBs can precipitate acute kidney injury in bilateral renal artery stenosis - a rise in creatinine >30% after starting these agents warrants investigation for RAS
- Flash pulmonary edema in a hypertensive patient without obvious cardiac cause should trigger evaluation for bilateral renal artery stenosis
- Resistant hypertension (uncontrolled on 3+ agents) is a strong indication to screen for renovascular disease
- Pressure natriuresis is the fundamental link between kidney disease and hypertension - when damaged kidneys cannot respond to rising BP with natriuresis, a new equilibrium is set at a higher BP
- Salt restriction and diuretics are especially effective in renal parenchymal hypertension because of the volume-dependent component
Sources: Comprehensive Clinical Nephrology, 7e; Brenner and Rector's The Kidney, 11e; Goldman-Cecil Medicine, 27e; NKF Primer on Kidney Diseases, 8e; Harrison's Principles of Internal Medicine, 22e
Pick any 3 topics in the discipline of Surgical disease and answer them in clinical structure for a viva prep
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a summary of what was covered across the three topics:
What You Just Got - Viva Cheat Sheet
| Topic | Key "Killer" Viva Points |
|---|---|
| Acute Appendicitis | Visceral-somatic pain sequence; Alvarado score (MANTRELS); McBurney's + Rovsing's + Psoas signs; always do PR exam; laparoscopic appendicectomy gold standard; Ochsner-Sherren for appendix mass; exclude caecal carcinoma in >40y |
| Intestinal Obstruction | "Drip and suck" first; 4 Cs (colic, vomiting, distension, constipation); always examine hernial orifices; SBO vs. LBO AXR patterns; strangulation = surgical emergency (rising WBC, lactate, constant pain); Rigler's triad for gallstone ileus; Hartmann's for contaminated peritonitis |
| Carcinoma of Breast | Triple assessment (clinical + imaging + biopsy); Foote & Stewart classification; 4 molecular subtypes; Cooper's ligament → dimpling; peau d'orange = advanced; SLNB before ALND; NAST for T3/T4/TNBC/HER2+; tamoxifen vs. aromatase inhibitors; post-BCS RT mandatory; key prognostic factors |
This is a shared conversation. Sign in to Orris to start your own chat.