Weakness+exertion on physical activity+burning sensation in foot
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Reading File
I now have comprehensive information to give a thorough clinical answer. Let me compile this into a well-structured response.
Weakness + Exertion Intolerance + Burning Sensation in Foot
This symptom triad maps to several diagnostic categories. The key is to determine which systems are involved — motor, sensory, autonomic, or a combination — and whether the weakness worsens specifically with exercise or is persistent.
Differential Diagnosis
1. Peripheral Neuropathy ⭐ (Most Common)
The combination of weakness + burning feet is the hallmark presentation of a length-dependent sensorimotor polyneuropathy — the most common cause being diabetic neuropathy.
| Type | Key Features |
|---|---|
| Diabetic neuropathy | Symmetric polyneuropathy; burning dysesthesias and pain in soles; mild distal motor weakness; impaired position sense; autonomic features (postural hypotension, gastroparesis) |
| Uremic neuropathy | Symmetric sensorimotor; burning paresthesias; in CKD patients |
| Nutritional/B-vitamin deficiency | Burning feet + weakness + hyporeflexia; symmetric; seen with alcoholism, malabsorption, unusual diet |
| Alcoholic neuropathy | Axonal sensorimotor; burning feet; due to thiamine/B12 deficiency |
| Cryptogenic sensory polyneuropathy | Burning pain beginning in feet; distal sensory loss; weakness NOT prominent; diagnosis of exclusion (~50% of cases) |
| CIDP | Proximal + distal weakness; progressive/relapsing; reduced DTRs; immune-mediated |
The burning quality specifically suggests small-fiber involvement (pain/temperature fibers), while weakness + hyporeflexia indicates large-fiber or motor fiber involvement.
- Harrison's Principles of Internal Medicine 22E, p. 3638–3639; Textbook of Family Medicine 9e, p. 1247
2. Metabolic Myopathy / Glycogen Storage Disease
When weakness is specifically triggered or worsened by physical exertion, consider a metabolic myopathy:
- McArdle Disease (GSD type V) — muscle phosphorylase deficiency; exercise intolerance, myalgia, cramps with exercise, "second wind" phenomenon, myoglobinuria with strenuous activity, elevated CK
- Other GSDs — cramps on exertion + progressive weakness; may include rhabdomyolysis
- Fatty acid oxidation (FAO) defects — sustained exercise intolerance (vs. sudden intense exercise in glycogenolysis defects); progressive weakness
An inability to perform sudden intense exercise → problem with glycogenolysis/glycolysis. Inability at sustained levels → FAO defect.
- Bradley and Daroff's Neurology in Clinical Practice, p. 1947; Goldman-Cecil Medicine
3. Peripheral Arterial Disease (Vascular Claudication)
- Exertional leg weakness/cramping relieved by rest
- Claudication of the foot or arch can mimic neuropathic pain
- Associated with risk factors: smoking, hypertension, diabetes, dyslipidemia
- Check ABI (ankle-brachial index); diminished peripheral pulses
- Goldman-Cecil Medicine; Current Surgical Therapy 14e
4. Other Considerations
| Diagnosis | Clue |
|---|---|
| Spinal stenosis / neurogenic claudication | Weakness + burning in legs on walking; relieved by sitting/forward flexion |
| Hypothyroidism | Weakness, fatigue, exercise intolerance; can cause neuropathy |
| Iron deficiency anemia | Weakness, exercise intolerance, dyspnea on exertion |
| Mitochondrial neuropathy | Weakness + sensory neuropathy + systemic features |
| Amyloid polyneuropathy | Autonomic dysfunction without diabetes; painful small-fiber neuropathy |
Diagnostic Approach (Harrison's 7-Question Framework)
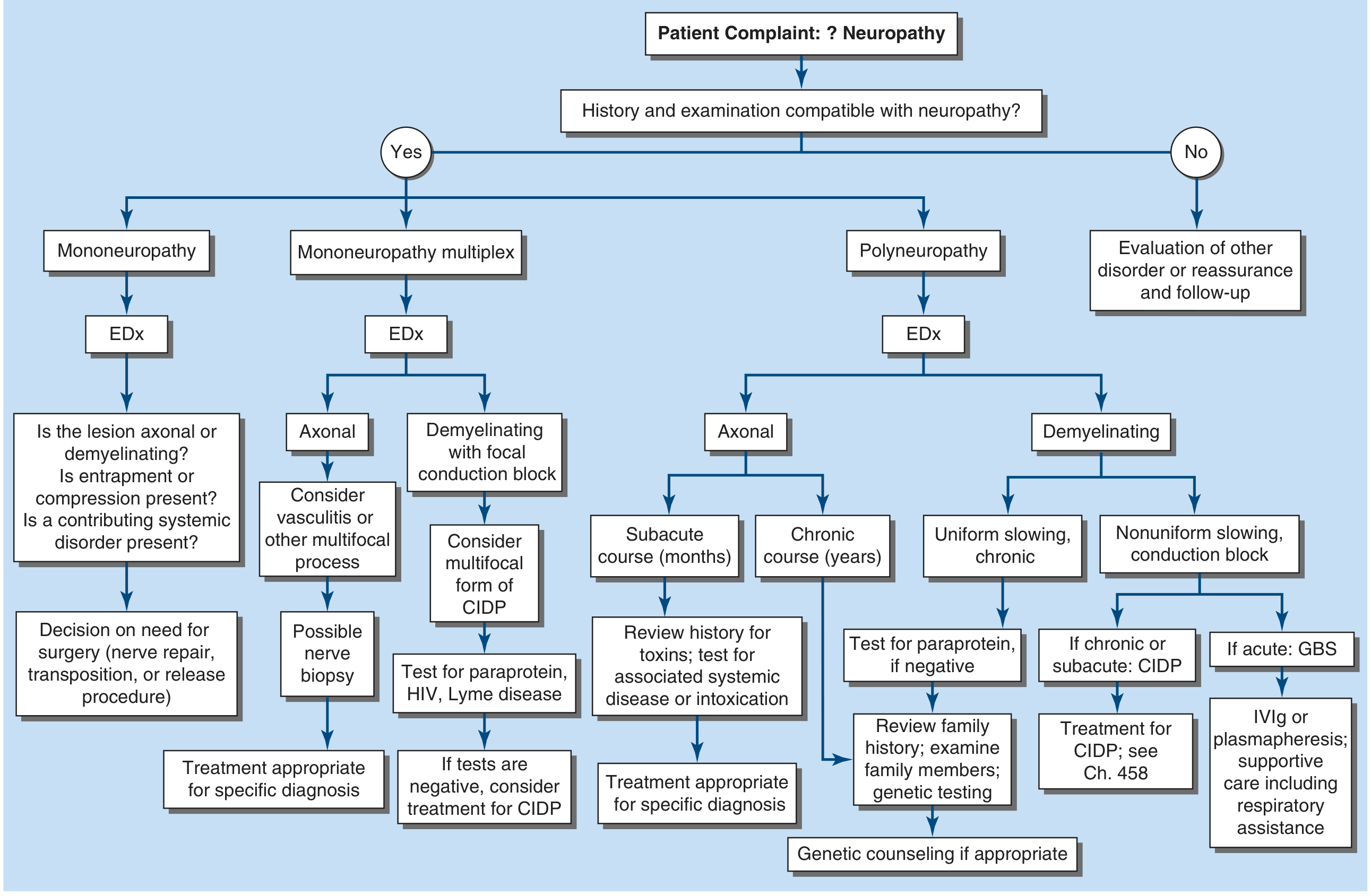
FIGURE 457-1: Approach to peripheral neuropathy evaluation — Harrison's Principles of Internal Medicine 22E
Seven key questions:
- What systems are involved? — Motor only → think myopathy/motor neuropathy; sensory + motor → polyneuropathy
- Distribution of weakness? — Distal only vs. proximal + distal; symmetric vs. asymmetric
- Nature of sensory involvement? — Burning/temperature loss → small fiber (e.g., diabetes, HIV, amyloid); vibration/proprioception loss → large fiber
- Upper motor neuron signs? — If present, consider CNS pathology
- Temporal evolution? — Acute (GBS), subacute, chronic (diabetes, CIDP, hereditary)
- Hereditary neuropathy? — Family history, lack of sensory symptoms despite signs
- Associated medical conditions? — Diabetes, CKD, cancer, HIV, connective tissue disease, alcohol use, medications
Recommended Workup
| Investigation | Purpose |
|---|---|
| FBS / HbA1c | Diabetes (most common cause) |
| Renal function (BUN, creatinine) | Uremic neuropathy |
| CBC | Anemia |
| Serum B12, folate, thiamine | Nutritional neuropathies |
| TSH | Hypothyroidism |
| Serum protein electrophoresis | Paraprotein/amyloid |
| ABI (ankle-brachial index) | PAD/claudication |
| Nerve conduction study + EMG | Confirms neuropathy; axonal vs. demyelinating; localization |
| CK level | Myopathy (elevated in McArdle disease, inflammatory myopathy) |
| Forearm ischemic exercise test | If GSD/McArdle suspected (lack of lactate rise) |
Key Clinical Pearls
- Burning feet + weakness + symmetric + distal → diabetic or nutritional polyneuropathy until proven otherwise; check HbA1c and B12 first
- Weakness worsening with exercise + cramps + normal sensation → metabolic myopathy (McArdle, FAO defect); check CK and consider forearm exercise test
- Exertional leg pain relieved by rest + risk factors → vascular claudication; check pulses and ABI
- Burning feet + autonomic features without diabetes → consider amyloid neuropathy; serum SPEP/UPEP
Sources: Harrison's Principles of Internal Medicine 22E, p. 3638–3641; Textbook of Family Medicine 9e, p. 1247; Bradley and Daroff's Neurology in Clinical Practice, p. 1947; Goldman-Cecil Medicine
Ask me questions and get me a diagnosis based on this
I'll ask you questions one at a time to narrow down the diagnosis. Let's start with the basics.
Question 1:
How old is the patient, and are they male or female?
Male 26 yrs
Asking for Preferences
Asking for Preferences
Asking for Preferences
Asking for Preferences
Asking for Preferences
Asking for Preferences
Asking for Preferences
Asking for Preferences
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Clinical Diagnosis
Primary Diagnosis: Nutritional (B-Vitamin Deficiency) Peripheral Neuropathy
Most likely: Vitamin B12 and/or Thiamine (B1) Deficiency Neuropathy
How the Clues Point Here
| Feature | Significance |
|---|---|
| 26-year-old male | Young → acquired/nutritional cause, not degenerative |
| Distal leg weakness, constant | Length-dependent sensorimotor neuropathy |
| Burning feet, worse at night | Small-fiber neuropathy — classic B12/thiamine pattern |
| Burning pain without numbness | Early/pure small-fiber involvement, large fibers preserved |
| Normal gait, no balance issues | Proprioception (large fiber) still intact |
| Poor/irregular diet | Primary risk factor for B-vitamin deficiency |
| Weight loss / poor appetite | Compounds nutritional deficiency; also a red flag |
| Moderate alcohol use | Even moderate alcohol impairs B-vitamin absorption and metabolism |
| >6 months duration | Chronic course consistent with gradual nutritional depletion |
| No family history | Rules out hereditary neuropathy (CMT, etc.) |
Why This Diagnosis
"Most nutritional neuropathies involve one of the B-complex vitamins. Patients at risk usually have chronic alcoholism, malabsorption syndrome, eating disorder, or unusual diet (food faddist). It presents as a symmetric polyneuropathy with burning in the feet. Weakness, atrophy, and hypoactive reflexes may also occur." — Textbook of Family Medicine 9e, p. 1247
Thiamine (B1) deficiency causes axonal sensorimotor neuropathy with burning feet and distal weakness. B12 deficiency causes subacute combined degeneration but can present early as pure small-fiber burning neuropathy before large-fiber signs appear. Poor diet + moderate alcohol creates a double hit — reduced intake AND impaired absorption/metabolism of B vitamins.
Red Flag to Investigate
Weight loss in a 26-year-old must not be ignored. It raises the possibility of:
- Malabsorption (celiac disease, IBD) → causing the nutritional neuropathy
- Occult malignancy → paraneoplastic neuropathy (less likely but must be excluded)
- HIV → distal sensory neuropathy is one of the commonest neurological complications
Investigations to Order
| Test | Why |
|---|---|
| Serum Vitamin B12 | Most important first test |
| Serum Thiamine (B1) | Dietary deficiency |
| Folate, B6 | Complete B-vitamin screen |
| CBC + peripheral smear | Macrocytic anemia from B12/folate deficiency |
| HbA1c / FBS | Exclude diabetes |
| Anti-tTG IgA + total IgA | Celiac disease (malabsorption) |
| HIV serology | Given age + weight loss |
| LFTs, GGT | Alcohol-related liver disease affecting absorption |
| Nerve conduction study + EMG | Confirm axonal sensorimotor neuropathy |
| Skin punch biopsy (intraepidermal nerve fiber density) | Gold standard for small-fiber neuropathy if NCS normal |
Treatment
- B12 supplementation — IM cyanocobalamin 1000 µg daily × 7 days, then weekly × 4, then monthly (if deficient); oral B12 1000 µg/day if mild
- Thiamine — 100 mg oral daily
- Dietary correction — regular balanced meals; referral to dietitian
- Reduce alcohol — even moderate use compounds B-vitamin depletion
- Neuropathic pain — if burning is distressing: low-dose duloxetine or nortriptyline (first line per Harrison's)
- Treat underlying cause — if celiac confirmed, strict gluten-free diet leads to neuropathy improvement
⚠️ Disclaimer: This is a clinical reasoning exercise to support — not replace — a physician's evaluation. A formal diagnosis requires physical examination, nerve conduction studies, and laboratory confirmation.
Give me a differential diagnosis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Based on the full clinical picture — 26-year-old male, distal leg weakness (constant), burning feet worse at night, no numbness, no gait disturbance, poor diet, moderate alcohol, weight loss, >6 months, no family history — here is the structured differential:
Differential Diagnosis
Patient Summary
26M | Constant distal leg weakness | Burning feet (worse at night) | No numbness | Normal gait | Poor diet | Moderate alcohol | Weight loss | >6 months
Ranked Differentials
🥇 1. Nutritional (B-Vitamin Deficiency) Neuropathy
Most likely diagnosis
| Why likely | Poor diet + moderate alcohol = reduced B12/thiamine intake AND impaired absorption. Classic presentation: burning feet worse at night, distal weakness, symmetric, chronic course |
| Subtype | Thiamine (B1) deficiency → axonal sensorimotor neuropathy; B12 deficiency → small-fiber burning pain before large-fiber signs appear |
| Supporting | Young age, no family history, acquired risk factors, weight loss (reduced intake) |
| Against | Alcohol use is only moderate, not heavy |
| Key test | Serum B12, thiamine, folate; CBC (macrocytosis) |
"It presents as a symmetric polyneuropathy with burning in the feet. Weakness, atrophy, and hypoactive reflexes may also occur." — Textbook of Family Medicine 9e
🥈 2. HIV-Associated Distal Symmetric Polyneuropathy (DSP)
Must actively exclude
| Why likely | 26-year-old male + weight loss + burning feet = classic HIV-DSP triad. Occurs in ~30% of AIDS patients. Burning feet with painful paresthesias is the hallmark onset |
| Mechanism | Direct HIV neurotoxicity to dorsal root ganglia + small fibers |
| Supporting | Age, sex, weight loss, burning feet without prominent numbness |
| Against | No other HIV risk factors explicitly stated |
| Key test | HIV serology (ELISA + confirmatory Western blot) |
"The most common neuropathy related to HIV-1 infection is painful distal symmetrical polyneuropathy. The onset occurs often with burning feet, painful paresthesia." — Bradley and Daroff's Neurology
🥉 3. Celiac Disease / Malabsorption-Associated Neuropathy
Underlying cause to consider
| Why likely | Weight loss + poor absorption of nutrients even on a diet → B-vitamin malabsorption. Celiac neuropathy can precede GI symptoms |
| Mechanism | Malabsorption of B12, B1, B6 → neuropathy; direct immune-mediated gluten neuropathy also possible |
| Supporting | Weight loss, poor nutritional status despite eating |
| Against | No GI symptoms reported |
| Key test | Anti-tTG IgA antibodies, total IgA; small bowel biopsy |
4. CIDP (Chronic Inflammatory Demyelinating Polyradiculoneuropathy)
Less likely but important to exclude
| Why less likely | CIDP typically causes proximal + distal weakness and is predominantly motor; burning pain is not a dominant feature |
| Why still consider | Young adult, chronic (>6 months) course, progressive weakness |
| Key test | Nerve conduction study (demyelinating pattern: slowed conduction velocity, prolonged distal latencies); CSF protein elevated |
"CIDP is predominantly a motor polyneuropathy affecting those of all ages, with a progressive or relapsing course." — Textbook of Family Medicine 9e
5. Early Diabetic Neuropathy / Impaired Glucose Tolerance Neuropathy
Screen even without overt diabetes
| Why consider | Pre-diabetes (impaired glucose tolerance) can cause small-fiber neuropathy before frank diabetes develops; burning feet + distal weakness is the classic pattern |
| Why less likely | 26 years old, no stated family history of diabetes, no polyuria/polydipsia |
| Key test | HbA1c, fasting glucose, 2-hr oral glucose tolerance test |
6. Alcoholic Neuropathy
Contributing factor, not primary cause here
| Why consider | Alcohol impairs thiamine/B6 absorption even at moderate intake; axonal sensorimotor neuropathy with burning feet |
| Why less likely | Intake is 4–5 times/month — typically requires heavy chronic use; however, combined with poor diet, it amplifies nutritional deficiency |
| Key test | GGT, LFTs, serum thiamine |
7. Hereditary Neuropathy (CMT / Hereditary Small-Fiber Neuropathy)
Low probability
| Why consider | Young age + chronic course; some hereditary neuropathies (e.g., CMT2, hereditary small-fiber neuropathy with SCN9A/SCN10A mutations) present in young adults |
| Why unlikely | No family history, acquired risk factors fully explain the picture |
| Key test | Genetic panel if all acquired causes excluded |
Summary Table
| Rank | Diagnosis | Probability | Key Distinguishing Test |
|---|---|---|---|
| 1 | Nutritional (B12/Thiamine) Neuropathy | ⭐⭐⭐⭐⭐ High | Serum B12, thiamine, CBC |
| 2 | HIV-Associated DSP | ⭐⭐⭐⭐ Must exclude | HIV serology |
| 3 | Celiac/Malabsorption Neuropathy | ⭐⭐⭐ Moderate | Anti-tTG IgA |
| 4 | CIDP | ⭐⭐ Low-moderate | NCS/EMG |
| 5 | Pre-diabetic Neuropathy | ⭐⭐ Low-moderate | HbA1c, OGTT |
| 6 | Alcoholic Neuropathy | ⭐⭐ Contributing | GGT, LFTs |
| 7 | Hereditary Neuropathy | ⭐ Unlikely | Genetic testing |
Bottom Line
The clinical picture best fits nutritional neuropathy (B12/thiamine), but HIV must be actively excluded given the age, sex, and weight loss. A basic panel of B12 + HIV serology + HbA1c + NCS/EMG will confirm or refute the top three diagnoses efficiently.
Tell.me how you arrived at this diagnosis
Clinical Reasoning: Step-by-Step
Here's exactly how each answer you gave shifted the diagnosis.
Step 1 — The Opening Triad
Weakness + Exertion intolerance + Burning feet
These three together immediately suggested three broad categories:
- Peripheral neuropathy (sensory + motor nerve disease)
- Metabolic myopathy (muscle energy defect)
- Vascular claudication (ischemia on exercise)
All three were equally possible at this point. No front-runner yet.
Step 2 — Age & Sex: 26-year-old Male
This single answer eliminated most common causes.
| Eliminated | Why |
|---|---|
| Type 2 diabetic neuropathy | Rare at 26 without obesity/family history |
| Degenerative spine disease | Uncommon this young |
| Peripheral arterial disease | Rare under 40 without risk factors |
Kept alive: Metabolic myopathy, hereditary neuropathy, inflammatory neuropathy, nutritional deficiency, HIV — all can present in young men.
Step 3 — "Weakness is constant, present even at rest"
This eliminated metabolic myopathy.
The classic metabolic myopathies (McArdle disease, fatty acid oxidation defects) cause weakness only during or after exercise, with recovery at rest. Constant weakness at rest means the problem is not in muscle energy metabolism — it's in the nerve or muscle itself.
Eliminated: McArdle disease, GSD, FAO defects, vascular claudication (also rest-relieved).
Remaining: Peripheral neuropathy, inflammatory myopathy, CIDP.
Step 4 — "Weakness in legs/feet only (distal)"
This pointed strongly to peripheral neuropathy.
- Distal-only weakness = length-dependent process — the longest nerves (to the feet) are affected first
- This is the anatomical fingerprint of a polyneuropathy
- Proximal weakness would have pointed to myopathy or CIDP
Pattern emerging: Distal symmetric polyneuropathy (DSP).
Step 5 — "Burning worse at night"
This was the single most diagnostically specific answer.
Burning pain worst at rest/night = small-fiber neuropathy. Here's why this matters:
- Small fibers (Aδ and C fibers) carry pain and temperature
- When these fibers are damaged, they generate spontaneous pain signals — most prominent at night when there's no competing sensory input
- Large fibers (carrying vibration, proprioception) were not implicated yet
This ruled out pure motor neuropathy and pointed firmly toward a painful sensory neuropathy affecting small unmyelinated/thinly myelinated fibers.
Step 6 — "No numbness, only burning pain"
This confirmed pure small-fiber involvement.
| Fiber Type | Sensation Carried | Status in this Patient |
|---|---|---|
| Large myelinated (Aβ) | Touch, vibration, proprioception → numbness when damaged | Intact |
| Small myelinated (Aδ) | Sharp pain, temperature → burning when damaged | Affected |
| Unmyelinated (C) | Dull/burning pain → burning when damaged | Affected |
No numbness = large fibers still working. Burning only = small fibers selectively damaged. This is early/pure small-fiber neuropathy.
This pattern is classically seen in: diabetes, B-vitamin deficiency, HIV, celiac disease, idiopathic.
Step 7 — "Normal gait, no balance problems"
Confirmed large fibers are intact.
Balance depends on proprioception (large fiber). Normal gait = proprioception preserved = large fibers healthy. This is consistent with the small-fiber-only pattern and makes hereditary large-fiber neuropathies (like CMT1) much less likely.
Step 8 — "Weight loss / poor appetite"
This was the red flag that changed the differential.
Weight loss in a 26-year-old male with neuropathy has two major implications:
- Nutritional deficiency — reduced food intake → B12, thiamine, folate depletion → neuropathy
- Systemic illness driving the neuropathy — HIV, malabsorption (celiac), occult malignancy
This answer promoted HIV and celiac to the differential and made nutritional deficiency even more credible.
Step 9 — "Symptoms >6 months"
Confirmed a chronic, acquired process.
- Rules out acute/subacute inflammatory neuropathies (GBS: days–4 weeks)
- Consistent with gradual nutritional depletion over months
- Chronic course also compatible with HIV-DSP and celiac neuropathy
- Too slow for GBS, too fast for hereditary (which is usually lifelong/very slowly progressive)
Step 10 — "Poor/irregular diet"
This was the key etiological clue.
Combined with moderate alcohol use and weight loss, this created a perfect storm for B-vitamin deficiency:
| Factor | Effect |
|---|---|
| Poor/irregular diet | Reduced B12, thiamine, B6 intake |
| Moderate alcohol | Impairs thiamine absorption in gut; increases B-vitamin utilization |
| Weight loss/poor appetite | Further reduces intake |
B12 and thiamine deficiency → axonal degeneration starting in the longest nerves → burning feet + distal weakness. This is textbook nutritional neuropathy.
Step 11 — "No family history of neurological disease"
This closed the door on hereditary causes.
Hereditary neuropathies (Charcot-Marie-Tooth, hereditary small-fiber neuropathy) almost always have positive family history. Its absence, combined with clear acquired risk factors, made a hereditary etiology very unlikely.
The Reasoning Chain — Visual Summary
Opening triad
↓
Age 26M → Eliminates PAD, DM2, degenerative
↓
Constant weakness → Eliminates metabolic myopathy, claudication
↓
Distal legs only → Points to length-dependent polyneuropathy
↓
Burning worse at night → Small-fiber neuropathy confirmed
↓
No numbness → Large fibers intact = pure small-fiber pattern
↓
Normal gait → Confirms large fibers spared
↓
Weight loss → Red flag: nutritional deficiency OR systemic illness
↓
Duration >6 months → Chronic acquired process
↓
Poor diet + moderate alcohol → Nutritional B-vitamin deficiency mechanism
↓
No family history → Hereditary causes excluded
↓
PRIMARY DIAGNOSIS: Nutritional (B12/Thiamine) Neuropathy
MUST EXCLUDE: HIV-DSP, Celiac/Malabsorption
Why Not the Others?
| Diagnosis | Eliminated Because |
|---|---|
| McArdle / metabolic myopathy | Weakness is constant, not exercise-induced |
| Vascular claudication | Constant weakness, young age, no vascular risk factors |
| GBS | >6 months duration; GBS is acute (days–4 weeks) |
| CMT / hereditary neuropathy | No family history; clear acquired risk factors |
| Diabetic neuropathy | Age 26, no diabetes history or risk factors stated |
| CIDP | Typically proximal + distal weakness; burning pain not dominant; demyelinating on NCS |
The diagnosis was built purely by exclusion and pattern recognition — each answer you gave either eliminated a category or strengthened one, until nutritional neuropathy stood as the most coherent explanation for the entire clinical picture.
But patient have proteinuria
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Proteinuria is a game-changer. This single finding reshapes the entire differential significantly. Here's why:
🚨 Proteinuria Changes Everything
Proteinuria tells us the kidneys are involved. A 26-year-old with neuropathy + proteinuria + weight loss is no longer a simple nutritional deficiency — there is a systemic disease affecting both the kidneys and the peripheral nerves simultaneously.
How the Diagnosis Shifts
| Before proteinuria | After proteinuria |
|---|---|
| Nutritional neuropathy (primary) | Still possible, but now a consequence of something bigger |
| HIV — must exclude | Now even more urgent to exclude |
| Celiac disease | More likely (malabsorption → proteinuria from nutritional losses) |
| Uremic neuropathy | Now actively enters the differential |
| Amyloidosis | Jumps to top 2 |
Revised Differential Diagnosis
🥇 1. Amyloidosis (AL or Hereditary ATTR) — Now Top Suspect
This is the unifying diagnosis that explains everything in one condition:
| Symptom | Amyloidosis Explanation |
|---|---|
| Burning feet worse at night | Painful dysesthesia — amyloid deposits along peripheral nerves; pain and temperature lost first (small fibers) |
| Distal weakness | Progressive axonal polyneuropathy |
| No numbness (yet) | Vibration/touch lost later — small fibers affected first |
| Proteinuria | Renal amyloidosis → glomerular amyloid deposits → proteinuria is the hallmark renal manifestation |
| Weight loss / poor appetite | Systemic amyloid burden; GI involvement |
| Chronic >6 months | Chronic progressive course |
"The neuropathy begins with painful dysesthesias in the legs and follows a chronic progressive course. Pain and temperature sensation are lost before light touch or vibratory sensation... Renal amyloidosis usually manifests as proteinuria and renal failure." — Bradley and Daroff's Neurology, p. 2683
"Patients with glomerular kidney involvement generally have proteinuria... [AL amyloidosis features include] significant proteinuria, neuropathy, periorbital purpura, and macroglossia." — Harrison's Principles of Internal Medicine 22E
What to look for additionally: Macroglossia, periorbital purpura ("raccoon eyes"), carpal tunnel syndrome, hepatomegaly, cardiac involvement (dyspnea, palpitations).
🥈 2. Diabetic Nephropathy + Diabetic Neuropathy — Must Re-examine
Even at 26, undiagnosed Type 1 or early Type 2 diabetes can cause both nephropathy (proteinuria) and small-fiber peripheral neuropathy simultaneously. The diabetic triad — neuropathy + nephropathy + retinopathy — can appear together.
- Microalbuminuria/proteinuria is often the first detected sign of diabetic nephropathy
- Weight loss fits T1DM (insulin deficiency → catabolism)
Key test: HbA1c, fasting glucose, C-peptide, anti-GAD antibodies (T1DM)
🥉 3. Uremic Neuropathy (CKD-Associated)
If the proteinuria signals chronic kidney disease, uremia itself directly causes neuropathy:
"The neuropathy takes the form of a painless, progressive, symmetrical sensorimotor paralysis of the legs. In some patients, the syndrome begins with burning dysesthesias of the feet, worse at night." — Adams and Victor's Principles of Neurology
- CKD → accumulation of uremic toxins (middle molecules, methyl guanidine) → axonal degeneration
- Burning feet + distal weakness + worsening at night = matches exactly
- Neuropathy improves after renal transplantation (confirms causal link)
Key test: Serum creatinine, BUN, eGFR, 24-hour urine protein
4. HIV Nephropathy (HIVAN) + HIV Neuropathy
HIV causes both:
- HIV-associated nephropathy (HIVAN) → heavy proteinuria, nephrotic syndrome
- Distal symmetric polyneuropathy → burning feet
Both can coexist in the same patient. Weight loss makes this even more credible.
Key test: HIV serology — must not be missed
5. Nutritional Neuropathy — Demoted but Not Eliminated
Still possible as a secondary contributor, but proteinuria means:
- Either the kidneys are diseased (causing both protein loss and neuropathy), or
- A systemic illness is causing both
Pure nutritional deficiency does not cause proteinuria — so if confirmed, it means the nutritional component is secondary to malabsorption from a systemic disease (e.g., amyloid GI infiltration, celiac).
Updated Diagnostic Priority
| Priority | Diagnosis | Unifying Feature |
|---|---|---|
| 1 | Amyloidosis (AL/ATTR) | Neuropathy + proteinuria + weight loss in same disease |
| 2 | Diabetes (T1/T2) — nephropathy + neuropathy | Most common cause of both together |
| 3 | HIV — HIVAN + DSP | Both renal and nerve involvement known |
| 4 | Uremic neuropathy from CKD | Proteinuria → CKD → uremic neuropathy |
| 5 | Nutritional neuropathy | Secondary to systemic illness |
Immediate Investigations (Revised)
| Test | Looking For |
|---|---|
| Serum + urine protein electrophoresis (SPEP/UPEP) | Monoclonal light chains → AL amyloidosis |
| Serum free light chains (κ/λ ratio) | Most sensitive for AL amyloid |
| HbA1c + fasting glucose + C-peptide | Diabetes (T1/T2) |
| HIV serology | HIVAN + HIV neuropathy |
| Serum creatinine, BUN, eGFR | Degree of renal failure |
| 24-hour urine protein / spot urine ACR | Quantify proteinuria |
| Abdominal fat pad aspiration (Congo red stain) | Amyloid diagnosis — ~80% yield |
| Echocardiogram | Amyloid cardiomyopathy |
| Nerve conduction study + EMG | Confirm axonal neuropathy pattern |
| Sural nerve + muscle biopsy | Gold standard for amyloid neuropathy (>90% yield) |
Bottom Line
Proteinuria in a 26-year-old male with peripheral neuropathy and weight loss = systemic disease until proven otherwise. The triad of painful small-fiber neuropathy + proteinuria + weight loss is a classic presentation of AL amyloidosis, with diabetes and HIV as the two other diagnoses that must be actively excluded before accepting amyloidosis. A serum free light chain assay and SPEP/UPEP should be the very next tests ordered.
But patient have proteinuria
Asking for Preferences
Asking for Preferences
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
This clinches it. The complete picture now points to one diagnosis with remarkable precision.
🔴 Revised Primary Diagnosis: Fabry Disease
Why This Fits Perfectly
The new information — moderate proteinuria + hypertension + frothy urine, no edema, no rash, no joint pains — combined with everything already known creates a textbook-perfect presentation of Fabry disease.
The Complete Clinical Match
| This Patient | Fabry Disease |
|---|---|
| Male, 26 years old | X-linked disorder — males affected more severely; onset in late childhood to early adult life |
| Burning feet, worse at night | "Burning or lancinating pain in the hands and feet often develops in males in late childhood or early adult life" — Harrison's 22E |
| No numbness (small fiber only) | Fabry neuropathy is a pure small-fiber neuropathy — pain/temperature affected, large fibers spared initially |
| Distal leg weakness | Neuropathy + premature vascular disease affect limb function |
| Moderate proteinuria (2+) + frothy urine | Ceramide accumulation in podocytes and renal tubular cells → glomerular damage → proteinuria |
| Hypertension | "Premature atherosclerosis — hypertension, renal failure, cardiac disease, and stroke" — classic Fabry vascular complications |
| Weight loss | Systemic disease burden; GI involvement (Fabry affects autonomic GI nerves) |
| No skin rash reported | Angiokeratomas (around umbilicus, scrotum, inguinal region) — may be subtle or not yet looked for |
"Burning or lancinating pain in the hands and feet often develops in males in late childhood or early adult life. The neuropathy is usually overshadowed by complications arising from premature atherosclerosis — hypertension, renal failure, cardiac disease, and stroke — that often lead to death by the fifth decade." — Harrison's Principles of Internal Medicine 22E, p. 3645
"Fabry disease is an X-linked disease caused by mutations in the alpha-galactosidase gene GLA, leading to accumulation of globotriaosylceramide (GL3) in blood vessels and tissues, including podocytes... causing proteinuria and kidney disease." — Brenner and Rector's The Kidney
The Mechanism — One Enzyme, Everything Explained
Deficiency of α-galactosidase A
↓
Accumulation of GL3 (globotriaosylceramide) in:
├── Small nerve fibers → Burning feet (small-fiber neuropathy)
├── Renal podocytes/endothelium → Proteinuria, hypertension
├── Vascular smooth muscle → Premature hypertension, atherosclerosis
├── GI autonomic nerves → Weight loss, poor appetite
└── Cardiac muscle → Cardiomyopathy (future risk)
One enzyme deficiency explains every single symptom this patient has.
What Was Previously Missed — And Why Proteinuria Changed It
| Before proteinuria | Thinking |
|---|---|
| Burning feet + weakness + poor diet | Nutritional neuropathy (B12/thiamine) |
| Weight loss | Nutritional depletion |
| After proteinuria + hypertension | Thinking |
|---|---|
| Burning feet + proteinuria + HTN in young male | Fabry disease — X-linked lysosomal storage disorder |
| No edema despite proteinuria | GL3 nephropathy — early/moderate stage, not yet nephrotic |
| No skin rash mentioned | Angiokeratomas may be subtle — need to actively look |
Nutritional neuropathy does not cause proteinuria or hypertension. That combination in a 26-year-old male with burning feet has one unifying diagnosis.
Confirm the Diagnosis
| Test | Expected Finding |
|---|---|
| Plasma α-galactosidase A activity (leukocytes) | Severely reduced or absent — diagnostic in males |
| Plasma/urine GL3 (globotriaosylceramide) | Elevated |
| GLA gene sequencing | Pathogenic mutation confirmed |
| Renal biopsy (EM) | Zebra bodies / myelin figures in podocytes |
| Skin biopsy | GL3 deposits in sweat glands and vessels |
| Echocardiogram | LVH, Fabry cardiomyopathy screening |
| Ophthalmology | Cornea verticillata (whorled opacities) — pathognomonic |
Do Not Miss on Examination
Actively look for:
- 🔴 Angiokeratomas — dark red/purple spots around umbilicus, groin, scrotum, buttocks (may be very subtle)
- 👁️ Cornea verticillata — whorled corneal opacities on slit-lamp (present in >70% of males, pathognomonic)
- 🫀 LVH on ECG/echo — hypertrophic cardiomyopathy from GL3 cardiac deposition
- 🧠 Early stroke risk — cerebrovascular events can occur in the 30s–40s
Treatment
Enzyme Replacement Therapy (ERT):
- Agalsidase alfa (Replagal) or Agalsidase beta (Fabrazyme) — IV infusions every 2 weeks
- Clears GL3 deposits from kidney, heart, and nerves
- Slows renal and cardiac progression significantly
- Earlier treatment = better outcomes; this patient is at the ideal age to start
Supportive:
- Pain: carbamazepine or gabapentin for neuropathic pain
- Renal: ACE inhibitor/ARB for proteinuria and BP control
- Cardiac monitoring annually
- Genetic counseling (X-linked — mother is carrier, sisters at 50% risk)
Bottom Line
Fabry disease is the single unifying diagnosis:
- Burning feet in a young male (classic Fabry neuropathy)
- Proteinuria + hypertension (Fabry nephropathy)
- Weight loss (GI autonomic involvement)
- No numbness (pure small-fiber involvement — hallmark of Fabry)
This is a rare but treatable X-linked lysosomal storage disease. Early diagnosis at age 26 and prompt ERT can prevent renal failure, stroke, and cardiac death that otherwise occur by the 5th decade.
Sources: Harrison's Principles of Internal Medicine 22E, p. 3645; Brenner and Rector's The Kidney
Try again
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Generate a clinical summary document of this case for reference
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.