
photo-1784274173494.jpg
Answers
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here are complete model answers for all questions, based primarily on Park's Textbook of Preventive and Social Medicine.
Q.1 Rabies (3+3 marks)
a) Categorize Animal Bite Exposures as per Latest WHO Guidelines
WHO classifies rabies exposures into 3 categories:
| Category | Type of Contact | Action Required |
|---|---|---|
| I | Touching/feeding animals; licks on intact skin | No PEP required |
| II | Nibbling of uncovered skin; minor scratches/abrasions without bleeding; licks on broken skin | Wound treatment + Vaccine |
| III | Single/multiple transdermal bites or scratches; contamination of mucous membrane with saliva (licks); all bat exposures; contact with animals of Category 2/3 in endemic area | Wound treatment + Vaccine + Rabies Immunoglobulin (RIG) |
All Category II & III exposures require immediate wound treatment (soap + water wash for 15 min, then virucidal agent - povidone iodine/alcohol).
b) Current Schedule of Intra-Dermal Rabies Vaccination (IDRV) for Post-Exposure Prophylaxis
The Updated Thai Red Cross (TRC) / WHO-recommended ID schedule currently used in India:
2-Site ID (2-2-2-0-2) Schedule:
- Day 0: 0.1 mL ID at 2 sites
- Day 3: 0.1 mL ID at 2 sites
- Day 7: 0.1 mL ID at 2 sites
- Day 14: 0.1 mL ID at 2 sites (some schedules omit)
- Day 28/30: 0.1 mL ID at 1–2 sites (booster)
RIG (Rabies Immunoglobulin): For Category III - Human RIG (HRIG) 20 IU/kg body weight OR Equine RIG (ERIG) 40 IU/kg body weight, infiltrated at wound site on Day 0. Do not delay vaccine while waiting for RIG.
Key advantages of ID route: Saves vaccine (uses 0.1 mL vs 0.5-1.0 mL IM), cost-effective, equally immunogenic.
Previously vaccinated persons: Only 2 doses ID on Days 0 and 3 - NO RIG required.
Q.2 HIV in 28-Year-Old Pregnant Woman (3+3 marks)
a) Describe Public Health Measures to Prevent Mother-to-Child Transmission (MTCT)
Under India's PPTCT Programme (Prevention of Parent-to-Child Transmission):
- Universal HIV counselling and testing - Routine offer of HIV test to ALL pregnant women at ANC with "opt-out" approach; done at ICTCs
- Lifelong ART for all HIV+ pregnant women - TDF + 3TC + EFV (triple drug regimen) regardless of CD4 count or WHO clinical stage (Option B+), both for maternal health and prevention of vertical transmission
- Safe obstetric practices - Institutional deliveries; avoid unnecessary episiotomy, invasive monitoring, prolonged rupture of membranes
- Infant prophylaxis - Nevirapine syrup given to the newborn for 6 weeks
- Infant feeding counselling - Exclusive breastfeeding for 6 months while on ART OR replacement feeding if safe/affordable/feasible/sustainable/accessible (AFASS criteria)
- Family-centric approach - Involve spouse/partner for testing; prevent re-infection
- Co-infection management - Treat STIs, TB, and opportunistic infections
- Nutritional and psychosocial support
b) Explain Role of National AIDS Control Programme in Management
Under NACP IV (National AIDS Control Programme):
- More than 15,000 ICTCs provide PPTCT services nationwide
- Frontline health workers (ANMs) conduct community-based HIV screening at sub-centre level
- ART centres provide free lifelong triple-drug ART
- HIV-exposed infants receive Early Infant Diagnosis (EID) via DNA-PCR at 6 weeks
- Linkage to care: HIV+ mother linked to ART centre; infant followed up at 18 months for confirmatory antibody testing
- Prevention of new infections through IEC/BCC campaigns, targeted interventions for high-risk groups
Q.3 30-Year-Old Man with >5 Hypo-Pigmented Patches (2+4 marks)
Diagnosis (2 marks)
Multibacillary (MB) Leprosy (Lepromatous type or BL/LL spectrum)
Basis of diagnosis:
- More than 5 hypo-pigmented (anaesthetic) skin patches - cardinal sign of leprosy
- Per WHO field criteria: >5 skin lesions = Multibacillary leprosy
- Confirm with: skin smear for AFB (positive in MB), skin biopsy
Cardinal signs of leprosy (any 1 = diagnosis):
- Hypo-pigmented/erythematous skin patches with loss of sensation
- Thickened/enlarged peripheral nerves
- Positive skin smear for AFB
Management as per National Leprosy Eradication Programme (4 marks)
MDT (Multi-Drug Therapy) for Multibacillary Leprosy (MB-MDT):
| Drug | Dose | Supervision |
|---|---|---|
| Rifampicin | 600 mg once a month (adults) / 450 mg for children <10 yr | Supervised |
| Dapsone | 100 mg daily (adults) / 50 mg daily for children | Self-administered |
| Clofazimine | 300 mg once a month + 50 mg daily (adults) | Monthly dose supervised |
Duration: 12 monthly blister packs, to be completed within 18 months
Additional management:
- Provide pre-packed MDT blister packs free of charge under NLEP via PHC/CHC
- Disability assessment at start and end of treatment
- Lepra reaction management:
- Type 1 (Reversal Reaction): Prednisolone 40-60 mg/day, continue MDT
- Type 2 (ENL): Thalidomide / Prednisolone / Clofazimine, continue MDT
- Physiotherapy and self-care to prevent deformities
- Social rehabilitation, counselling to reduce stigma
- Contact examination of household contacts annually
Note: MDT continues even during pregnancy (safe) and in HIV co-infection.
Q.4 Short Notes (Any 3 out of 4) - (3×6=18 marks)
1. Disability-Adjusted Life Year (DALY)
Definition: DALY is a measure of the burden of disease in a population. It represents the number of years of healthy life lost due to ill-health, disability, or early death.
Formula:
DALY = YLL + YLD
- YLL (Years of Life Lost) = due to premature mortality
- YLD (Years Lived with Disability) = due to disability/morbidity
One DALY = one year of healthy life lost
Components:
- YLL = N × L, where N = number of deaths and L = standard life expectancy at age of death
- YLD = I × DW × L, where I = incidence, DW = disability weight (0–1), L = average duration
Uses:
- Measures overall disease burden in a population
- Compares burden of different diseases
- Priority-setting for health interventions and resource allocation
- Used in Cost-Effectiveness Analysis (CEA) as cost per DALY averted
Example: A country reporting 500 DALYs per 1000 population for TB indicates 500 healthy years lost per 1000 people due to TB.
2. Consequences of Failure to Disclose Medical Errors
Definition: Medical error is a preventable adverse event resulting from care provided to a patient, not due to the underlying disease.
Consequences of NON-DISCLOSURE:
A. For the Patient:
- Continued harm from unrecognized/uncorrected error
- Loss of trust in the healthcare system
- Unable to make informed decisions about alternative treatment
- Denied legal recourse or compensation
- Psychological harm - anxiety, anger when truth later discovered
B. For the Healthcare Provider:
- Ethical violation (breaches principle of veracity/transparency)
- Increased risk of litigation (cover-up is legally far worse)
- Loss of professional credibility
- Psychological burden - guilt, moral injury, burnout
- License/disciplinary action if concealment discovered
C. For the Healthcare System/Society:
- Errors not analyzed = errors repeat (no system learning)
- No quality improvement possible without error reporting
- Erosion of public trust in health institutions
- Increased healthcare costs from prolonged treatment of unresolved errors
- Undermines patient safety culture
Ethical basis for disclosure: Principles of autonomy, non-maleficence, beneficence, justice, and veracity all mandate honest communication of errors.
3. Confounding Factor and Bias in Epidemiological Studies
BIAS:
Definition: A systematic error in study design, data collection, or analysis that leads to an incorrect estimate of the true association between exposure and disease.
Types:
- Selection Bias - Systematic error in selecting study subjects (e.g., Berkson's bias, Neyman bias, Volunteer bias)
- Information/Measurement Bias - Error in classifying exposure or outcome
- Recall bias: Cases remember past exposure more than controls
- Observer bias: Investigator's knowledge influences data collection
- Confounding bias - (see below)
CONFOUNDING:
Definition: Confounding occurs when a third variable (confounder) is associated with both the exposure and the outcome, and distorts the true relationship between them.
Criteria for a confounder:
- Must be associated with the exposure
- Must be an independent risk factor for the disease
- Must NOT be on the causal pathway between exposure and disease
Example: In studying coffee-smoking-lung cancer relationship: Smoking is a confounder - it is associated with coffee drinking AND is independently a cause of lung cancer.
Control of confounding:
- At design stage: Randomization, Matching, Restriction
- At analysis stage: Stratification (Mantel-Haenszel), Multivariate analysis, Standardization
4. Role of Family in Health and Disease (Describe with Suitable Examples)
Family as the basic unit of society plays critical roles in health:
A. In Health Promotion:
- Healthy lifestyle habits (diet, exercise, hygiene) are shaped within the family
- Immunization decisions are family decisions
- Example: A family that maintains hand hygiene reduces diarrheal disease burden
B. In Disease Prevention:
- Genetic counseling and carrier detection (e.g., sickle cell, thalassemia)
- Early identification of symptoms and health-seeking behavior
- Example: Family history of diabetes prompts early screening in offspring
C. In Disease Causation (Family as a risk unit):
- Communicable diseases spread within families (TB, COVID-19, cholera)
- Genetic diseases cluster in families (hypertension, cancer)
- Behavioral risks - alcoholism, domestic violence, tobacco use
- Example: TB contact tracing is done within the family
D. In Care and Rehabilitation:
- Family provides physical, emotional, and financial support during illness
- Adherence to treatment (e.g., DOTS supervision by family member)
- Example: Caregiver in the family critical for stroke rehabilitation
E. Family Life Cycle and Health:
- Different stages (marriage, childbirth, aging) bring specific health challenges
- Family planning services target the family unit
Family Health Approach (7×7 Matrix by ICMF) is used to identify family health problems at each stage of family life cycle.
5. 7×7 Strategy of Anaemia Mukt Bharat (AMB)
Anaemia Mukt Bharat (AMB) was launched in 2018 under the National Nutrition Mission (POSHAN Abhiyaan) with the target of reducing anaemia prevalence by 3 percentage points per year among target beneficiaries.
The 7×7 Strategy:
7 Target Beneficiary Groups:
- Children 6–59 months
- Children 5–9 years
- Adolescent girls and boys (10–19 years)
- Pregnant women
- Breastfeeding women
- Women of reproductive age (15–49 years, non-pregnant, non-lactating)
- Elderly (60+ years)
7 Interventions:
- Prophylactic Iron and Folic Acid (IFA) supplementation - across life stages
- Deworming - biannual deworming for children and adolescents
- Intensified year-round IFA supplementation - using platform-based delivery (schools, AWCs)
- Mandatory IFA fortification of rice - supplied through PDS/mid-day meal
- Delayed cord clamping - at least 3 minutes at birth (for newborns)
- Treatment of moderate/severe anaemia at health facilities
- Behavioural change communication - to improve dietary diversification, address compliance issues
Delivery Platforms used: ICDS (AWCs), schools, health facilities, ASHA/ANM
Target: Reduce anaemia prevalence in all target groups by 3% per year, achieving anaemia-free India.
All answers based on Park's Textbook of Preventive and Social Medicine (PSM).
Define family as per K Park PSM book
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Found the exact definition. Here it is directly from the textbook:
Definition of Family - as per K. Park's Textbook of Preventive and Social Medicine
"The family is a primary unit in all societies. It is a group of biologically related individuals living together and eating from a common kitchen."
(Park's Textbook of Preventive and Social Medicine, Chapter: THE FAMILY)
Additional Elaboration Given by Park
Park further explains the family as a multi-dimensional unit:
| As a unit | Description |
|---|---|
| Biological unit | Family members share a pool of genes |
| Social unit | They share a common physical and social environment |
| Cultural unit | Reflects the culture of the wider society; determines behaviour and attitudes of its members |
| Epidemiological unit | Disease patterns cluster within families |
| Unit for social services | Basis for providing comprehensive medical care and social services |
Distinction: Family vs. Household
Park draws a clear distinction:
- Family = all members are blood relations (biologically related)
- Household = members may NOT be blood relations (e.g., servants living in the same house)
Two Types of Family (Sociological Terms)
- Family of origin - the family into which one is born
- Family of procreation - the family which one sets up after marriage

IMG_3522.jpg
Answer
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
All content retrieved. Here are the complete model answers for Q.4 (Any 5 out of 6), 5×2=10 marks.
Q.4 Very Short Answer (Any 5 out of 6) — 5×2=10 marks
1. Define Disability-Adjusted Life Year (DALY)
DALY is a measure of overall disease burden, expressing the number of years of healthy life lost due to ill-health, disability, or premature death.
Formula:
DALY = YLL + YLD
- YLL (Years of Life Lost) = No. of deaths at each age × expected remaining years of life (using a global standard life expectancy - Japanese life expectancy used as standard)
- YLD (Years Lived with Disability) = No. of incident cases × average duration of disease × disability weight (0 = perfect health; 1 = dead)
One DALY = One year of healthy life lost.
(Developed by Harvard University for World Bank in 1990; later adopted by WHO.)
2. Differentiate Control, Elimination and Eradication
| Feature | Control | Elimination | Eradication |
|---|---|---|---|
| Definition | Reducing incidence, duration, and effects of disease to a level where it is no longer a public health problem | Interruption of transmission of disease in a large geographic region/area | Termination of ALL transmission worldwide by extermination of the infectious agent |
| Agent | Still persists in community | Absent in the defined region | Completely exterminated globally |
| Scope | Local / national | Regional | Global |
| Example | Malaria control | Polio/measles elimination from a region | Smallpox (only disease eradicated globally) |
Elimination is an intermediate goal between control and eradication; it is now seen as an important precursor of eradication.
3. Describe the "One Health" Approach
"While there are many diseases, there is, in a sense, only ONE HEALTH" - Park's PSM
Definition: One Health is a collaborative, multisectoral, and transdisciplinary approach - working at local, regional, national, and global levels - with the goal of achieving optimal health outcomes, recognizing the interconnection between people, animals, plants, and their shared environment.
Key Pillars:
- Human health
- Animal health (domestic + wildlife)
- Environmental/ecosystem health
Rationale:
- ~60% of human infectious diseases are zoonotic (arise from animals)
- Emerging infections (Ebola, Nipah, Avian flu, COVID-19) arise at the human-animal-environment interface
- Antimicrobial resistance (AMR) spans all three sectors
Stakeholders involved: Physicians, veterinarians, ecologists, agriculture experts, public health professionals, policy makers
Example: Controlling rabies requires veterinary (dog vaccination), medical (human PEP), and environmental (stray dog management) sectors working together - a classic One Health application.
4. Isolation V/s Quarantine
| Feature | Isolation | Quarantine |
|---|---|---|
| Applied to | Infected persons (cases/carriers) | Healthy contacts of infectious disease |
| Definition | "Separation, for the period of communicability, of infected persons or animals from others, to prevent direct or indirect transmission of the infectious agent" | "Limitation of freedom of movement of well persons exposed to communicable disease, for a period not longer than the longest incubation period, to prevent contact with non-exposed persons" |
| Duration | Duration of communicability of the disease | Duration = longest incubation period of the disease |
| Purpose | Protect community from infected person | Prevent spread from potentially incubating persons |
| Current status | Still used (especially for highly infectious diseases) | Largely replaced by active surveillance |
| Example | Isolating a TB patient, COVID-19 case | 14-day quarantine for COVID-19 contacts |
5. Define Herd Immunity - Give One Suitable Example
Definition (Park's):
"Herd immunity (or community immunity) describes a type of immunity that occurs when the vaccination of a portion of the population (or herd) provides protection to unprotected individuals."
Herd immunity proposes that when a large number of a population are immune, it is difficult to maintain a chain of infection - reducing the likelihood that a susceptible person will come in contact with the infectious agent.
Elements contributing to herd immunity:
- Occurrence of clinical and subclinical infections in the herd
- Immunization of the herd
- Herd structure (births, deaths, population mobility)
Herd Immunity Threshold: The proportion of immune individuals above which a disease may no longer persist in the population. It varies with the virulence, vaccine efficacy, and contact patterns.
Example: During the measles epidemic in the Faroe Islands (1854) - the population had no prior immunity ("virgin population"), resulting in very high attack and case fatality rates. The epidemic declined only as herd immunity built up following natural infection. Conversely, once measles vaccination achieves ~>95% coverage, herd immunity prevents outbreaks even in unvaccinated individuals.
6. Two Characteristics of a Point-Source Epidemic + Diagram
Definition: In a point-source (common-source, single exposure) epidemic, exposure to the disease agent is brief and essentially simultaneous, and the resultant cases all develop within one incubation period of the disease.
Example: Food poisoning outbreak at a wedding feast.
Two Key Characteristics:
-
The epidemic curve rises and falls rapidly, with NO secondary waves - cases cluster within a narrow interval of time (explosive onset)
-
All cases develop within ONE incubation period of the disease from the time of exposure
(Third feature: The curve has a single peak, and the "median incubation period" - time for 50% of cases to occur after exposure - can be identified)
Epidemic Curve Diagram (Point-Source Epidemic from Park's):
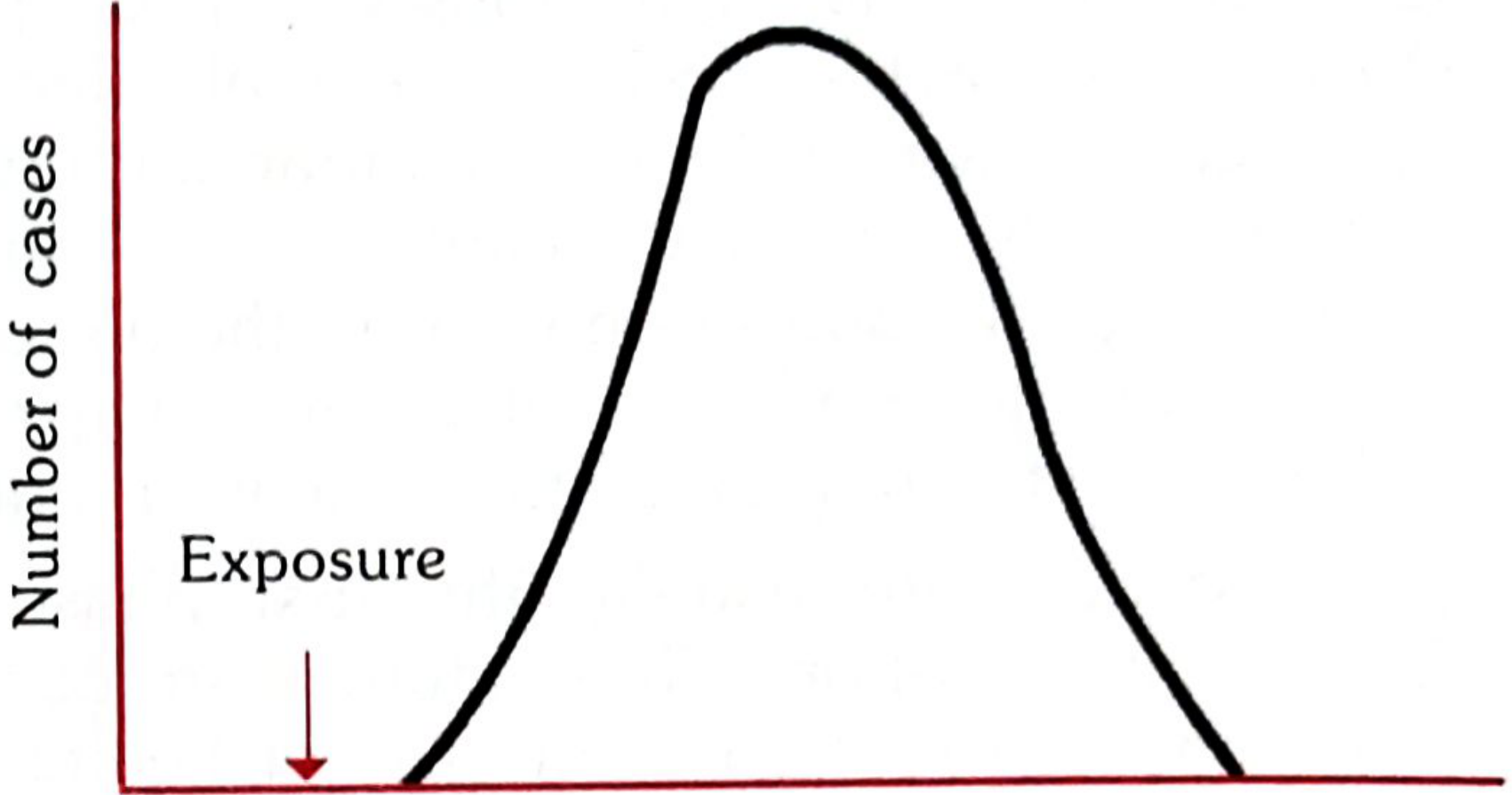
X-axis: Time | Y-axis: Number of cases | Arrow indicates point of single exposure
The curve shows a single bell-shaped peak - rapid rise, single peak, rapid fall - with all cases falling within one incubation period after the point of exposure.
All answers sourced from Park's Textbook of Preventive and Social Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.