Collateral circulation in pelvis briefly as 15 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive 15-mark answer. Let me compile it.
Collateral Circulation in the Pelvis
Introduction
The pelvis is exceptionally well collateralized, with a multitude of anastomoses between both visceral (organ-supplying) and parietal (wall-supplying) branches. Collateral circulation operates on the principle that an afferent vessel originating proximal to an occlusion anastomoses with an efferent vessel distal to it, restoring flow. These pathways become clinically significant in aortoiliac occlusive disease (Leriche syndrome), pelvic trauma, embolization procedures, and vascular surgery.
Pelvic Arterial Anatomy - Basis for Collaterals
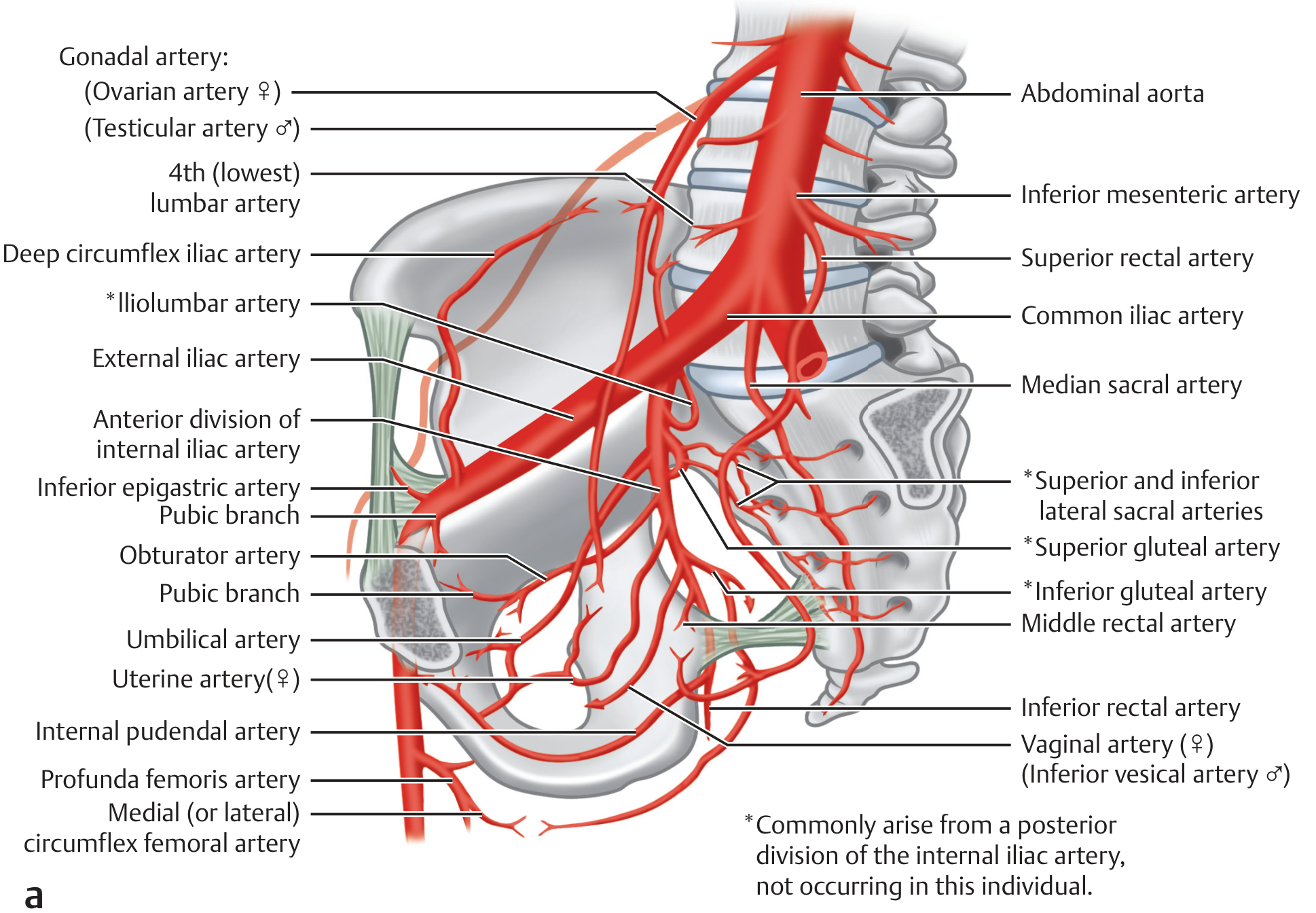
The main arterial supply to the pelvis comes from the internal iliac artery (hypogastric artery), which divides into:
- Anterior division: umbilical, obturator, internal pudendal, inferior vesical/vaginal, middle rectal, uterine arteries
- Posterior division: iliolumbar, lateral sacral, superior gluteal arteries
Both divisions contribute extensively to pelvic collateral networks.
Major Collateral Pathways
1. Distal Aortic / Common Iliac Occlusion (Leriche Syndrome)
When the distal aorta or common iliac artery is occluded, the internal iliac artery is reconstituted through:
- Lumbar arteries anastomosing with the iliolumbar artery (branch of posterior division of internal iliac)
- Lateral sacral arteries receiving flow from above
This is the primary parietal (paraspinal) collateral route.
2. Aortoiliac Occlusion - External Iliac Reconstitution
In aortoiliac occlusion, the external iliac and common femoral arteries can be reconstituted via:
- Lower intercostal and subcostal arteries → lumbar arteries → ascending branch of the deep circumflex iliac artery → external iliac artery
- Iliolumbar artery reconstituting the internal iliac, which then communicates with the external iliac
3. The Winslow Pathway (Subclavian-to-External Iliac)
A long-range collateral from the upper trunk to the lower limb:
Subclavian artery → Internal thoracic artery → Superior epigastric artery → Inferior epigastric artery → External iliac artery
This pathway is critically important in severe peripheral arterial disease. Harvesting the internal thoracic artery for CABG in a patient with aortoiliac occlusion can precipitate severe lower limb ischemia - making preoperative angiographic demonstration of this pathway essential.
4. External Iliac Occlusion
Collateral flow is provided by:
- The Winslow pathway (as above)
- Internal iliac to external iliac anastomoses via:
- Iliolumbar artery (posterior division of internal iliac) → deep circumflex iliac artery → external iliac
- Obturator artery → anastomoses with inferior epigastric artery (pubic branch)
5. Internal Iliac (Hypogastric) Occlusion
Collateral flow comes from transverse pelvic collaterals:
- Contralateral lateral sacral arteries (cross-pelvic anastomoses)
- Distal branches of the contralateral obturator artery and contralateral internal pudendal artery
- Median sacral artery (from the aorta directly) providing direct flow
- Iliolumbar and superior gluteal arteries receiving retrograde flow from the ascending branch of the lateral circumflex femoral and deep circumflex iliac arteries
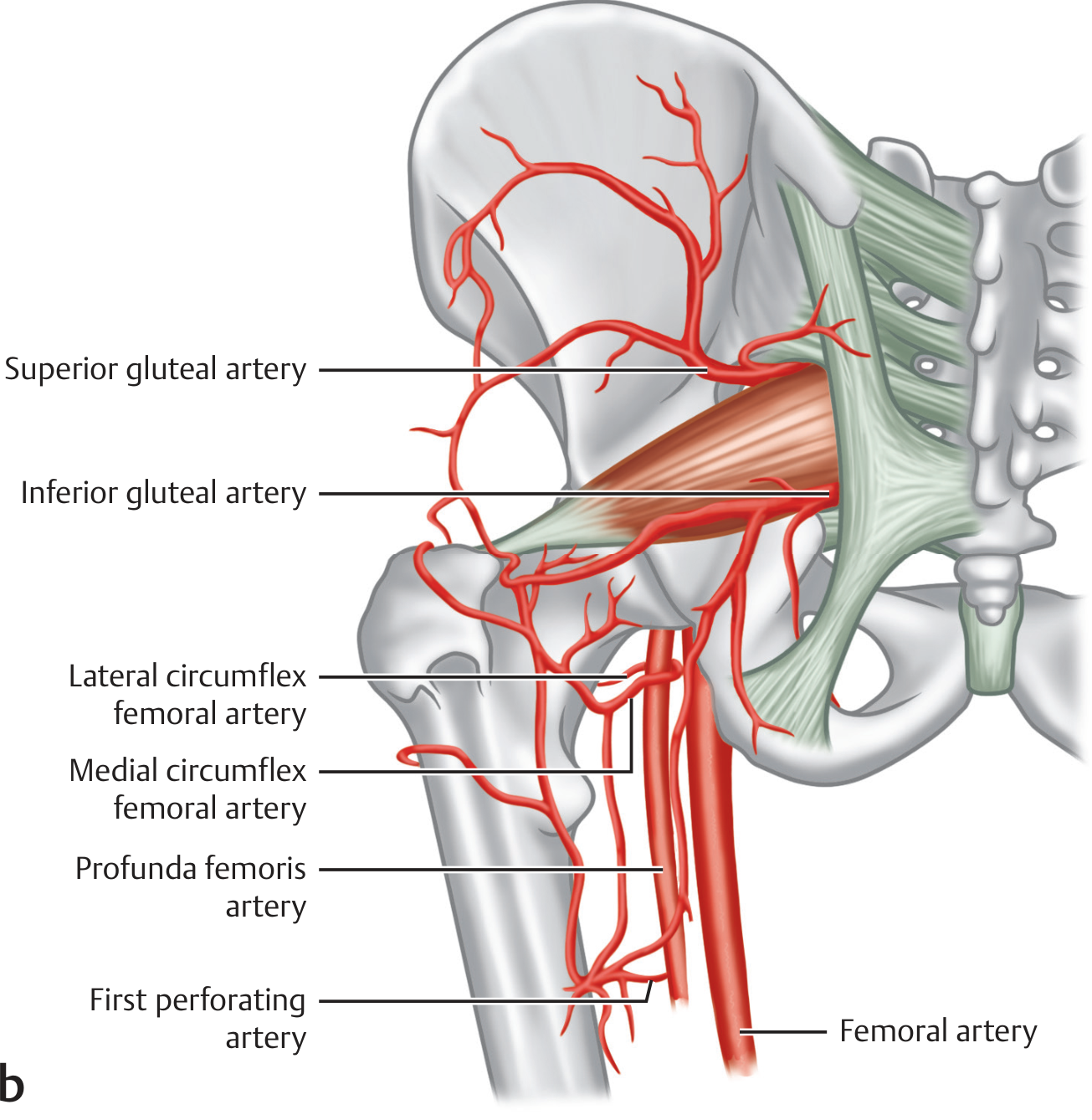
6. Trochanteric Anastomosis
At the trochanteric fossa, a rich anastomotic ring is formed between:
- Superior gluteal artery (posterior division, internal iliac)
- Inferior gluteal artery (anterior division, internal iliac)
- Ascending branch of the medial circumflex femoral artery
- Ascending branch of the lateral circumflex femoral artery
- Deep circumflex iliac artery
This anastomosis bridges pelvic vessels with femoral vessels.
7. Cruciate Anastomosis
Located at the upper thigh, formed by:
- Lateral circumflex femoral artery
- Medial circumflex femoral artery
- Inferior gluteal artery
- First perforating branch of the profunda femoris
8. Rectal (Hemorrhoidal) Anastomoses
A classic visceral collateral network within the pelvis:
| Artery | Origin | Level |
|---|---|---|
| Superior rectal artery | Inferior mesenteric artery | Upper rectum |
| Middle rectal artery | Internal iliac artery | Mid rectum |
| Inferior rectal artery | Internal pudendal artery | Lower rectum/anal canal |
These three arteries form a continuous submucosal plexus, important in rectal surgery and portal hypertension (inferior mesenteric - portal communication via superior rectal → hemorrhoidal plexus).
9. Vesical Anastomoses
The bladder receives supply from multiple anastomosing branches:
- Superior vesical artery (from patent umbilical artery)
- Inferior vesical artery (in males) / Vaginal artery (in females)
- These form a vesical plexus with cross-anastomoses
10. Uterine and Ovarian Anastomosis (Females)
The uterine artery (branch of anterior division of internal iliac) anastomoses freely with the ovarian artery (direct branch from the abdominal aorta) along the lateral border of the uterus. This is why ligation of the uterine artery alone is insufficient to completely devascularize the uterus.
Diagrams
Fig. 11.26 - Trochanteric and Cruciate Anastomoses:
Internal iliac artery and pelvic arterial branches:
Clinical Significance
| Clinical Scenario | Relevant Collateral |
|---|---|
| Leriche syndrome | Lumbar → iliolumbar → internal iliac |
| CABG with PAD | Winslow pathway must be preserved |
| Pelvic hemorrhage embolization | Bilateral embolization needed due to rich cross-pelvic flow |
| Uterine artery ligation (PPH) | Bilateral ligation required; ovarian artery compensates |
| AAA repair | Preserve internal iliac to prevent colonic/gluteal ischemia |
| Rectal cancer surgery | Rectal arterial arcade must be considered |
Summary
The pelvis has one of the richest collateral networks in the body, explained by:
- Multiple bilateral symmetrical vessels that cross-anastomose
- Vertical communications between abdominal (aortic) branches and pelvic vessels
- Visceral anastomoses between IMA, internal iliac, and pudendal branches
- Peripheral anastomoses at the trochanteric and cruciate levels linking pelvic to femoral circulation
This redundancy allows tolerance of single vessel ligation (e.g., internal iliac ligation for pelvic hemorrhage) without catastrophic ischemia, but bilateral or multilevel occlusions may overwhelm these pathways.
- Imaging Anatomy: Text and Atlas, Volume 3 - Bones, Joints, Vessels and Nerves, pp. 357-358 (Arterial Collateral Network of the Pelvis)
This is a shared conversation. Sign in to Orris to start your own chat.