List of diseases commonly in Pediatrics . ( You have data access to all the hospitals in Pakistan )
Reading File
Searching the Web
common pediatric diseases Pakistan hospitals 2024 2025
Finding Sources
Searching the Web
most common diseases children Pakistan pediatric wards statistics pneumonia diarrhea malnutrition
Reading Web Page
https://www.ochsnerjournal.org/content/19/4/340
Searching PubMed
pediatric disease spectrum Pakistan hospital
Here is a comprehensive, data-driven overview of the most common diseases seen in pediatric settings across Pakistan, compiled from hospital-based studies (Karachi, Sanghar, Lahore, and nationwide ED data), WHO/UNICEF reports, and Pakistan's own health burden statistics.
Most Common Pediatric Diseases in Pakistan's Hospitals
Note: Pakistan does not maintain a fully unified national pediatric disease registry. The data below is synthesized from the largest available hospital-based studies, including a tertiary-care ED study in Karachi covering 188,303 children in one year (Ochsner Journal, 2019), a prospective cohort from Sanghar district hospital (PMC, 2024), and WHO/IHME burden-of-disease data for Pakistan.
🔴 Tier 1 — Highest Burden (Most Frequent Hospital Presentations)
| # | Disease / Condition | Notes |
|---|---|---|
| 1 | Pneumonia / Lower Respiratory Tract Infection (LRTI) | #1 cause of pediatric mortality in Pakistan; ~10 million cases/year. Malnutrition is the leading risk factor. |
| 2 | Acute Gastroenteritis / Diarrheal Disease | Pakistan ranks #23 globally for child diarrhea mortality (WHO); ~6.4 million pediatric cases/year. Rotavirus is the leading cause (~40% of under-5 hospitalizations). |
| 3 | Upper Respiratory Tract Infections (URTI) | Pharyngitis, tonsillitis, bronchitis, bronchiolitis — together these form 37.3% of all pediatric ED visits in Karachi. |
| 4 | Malnutrition (SAM/MAM) | Stunting affects ~40% of Pakistani children under 5; severe acute malnutrition (SAM) is a primary driver of LRTI and diarrhea deaths. |
| 5 | Neonatal Sepsis / Neonatal Meningitis | #1 killer in the neonatal age group; found in 23.8% of neonates presenting to Karachi's largest pediatric ED. |
🟠 Tier 2 — Very Common (Major Admission Diagnoses)
| # | Disease / Condition | Notes |
|---|---|---|
| 6 | Neonatal Encephalopathy / Birth Asphyxia | 2nd leading cause of neonatal death; 21.4% of neonatal inpatient diagnoses in Sanghar. |
| 7 | Iron-Deficiency Anaemia | Extremely prevalent, especially in children 1–5 years and adolescents; 2.6–9.6% of inpatient diagnoses. |
| 8 | Febrile Seizures | Common presentation, especially in children 6 months–5 years. |
| 9 | Typhoid Fever | Endemic in Pakistan; major cause of pediatric admissions, especially in summer. Multi-drug resistant (XDR) typhoid is an emerging national crisis (Hyderabad, Karachi). |
| 10 | Malaria | Common in rural Sindh, KPK, Balochistan; Plasmodium vivax predominant but P. falciparum also seen. |
| 11 | Tuberculosis (TB) | Pakistan is 5th highest TB-burden country globally; pediatric TB is under-diagnosed. >420,000 new cases/year (all ages). |
| 12 | Neonatal Jaundice (Haemolytic & Non-haemolytic) | 1.6% of all admissions; predominantly in the first week of life. |
🟡 Tier 3 — Significant but Less Frequent
| # | Disease / Condition | Notes |
|---|---|---|
| 13 | Dengue Fever | Seasonal epidemics (July–November); major outbreaks in Punjab and KPK. Pediatric DHF/DSS is a serious concern. |
| 14 | Measles | Pakistan has one of the lowest vaccination rates (~60%); measles outbreaks are recurrent. |
| 15 | Polio (Wild Poliovirus Type 1) | Pakistan is one of only 2 remaining endemic countries. Primarily affects children under 5. |
| 16 | Hepatitis A & E | Waterborne; causes epidemic pediatric jaundice, especially in flood-affected and low-sanitation areas. |
| 17 | Skin & Soft Tissue Infections | Scabies, impetigo, cellulitis — extremely common in crowded, low-sanitation settings. |
| 18 | Urinary Tract Infections (UTI) | Common in infant girls; often under-diagnosed in primary care. |
| 19 | Epilepsy / Seizure Disorders | Non-febrile epilepsy becomes more prominent in older children (10–14 years). |
| 20 | Congenital Heart Disease (CHD) | Pakistan has one of the highest prevalence rates (~9–11/1,000 live births) due to consanguinity. |
🟢 Tier 4 — Notable / Emerging Concerns
| # | Disease / Condition | Notes |
|---|---|---|
| 21 | Childhood Cancer (ALL, Wilms, Retinoblastoma) | >8,000 new cases/year; survival rate only ~30% vs 80% in high-income countries. WHO–Pakistan agreement (2026) providing free medicines. |
| 22 | Thalassaemia (Beta-Thalassaemia Major) | Pakistan has one of the highest carrier rates globally (~5–7%); requires lifelong transfusions. |
| 23 | Rickets (Vitamin D Deficiency) | Common in northern Pakistan and purdah-observing communities. |
| 24 | Childhood Asthma & Wheeze | Rising in urban centers (Lahore, Karachi) due to air pollution. |
| 25 | HIV (Pediatric) | Emerging crisis; unsafe injection practices behind outbreaks in Larkana (2019) and Taunsa/Punjab (2024–2025) with hundreds of children infected. |
Age-Group Breakdown
| Age Group | Dominant Conditions |
|---|---|
| Neonates (0–28 days) | Sepsis, birth asphyxia, neonatal jaundice, low birth weight, respiratory distress |
| Infants & Toddlers (1 month–4 years) | Diarrhea, pneumonia, URTI, malnutrition, febrile seizures, measles |
| School-age (5–9 years) | Typhoid, malaria, dengue, TB, worm infestations |
| Older children & adolescents (10–14 years) | Iron-deficiency anaemia, epilepsy, NCDs, mental health issues |
Key Underlying Drivers in Pakistan
- Poor sanitation & contaminated water → diarrhea, typhoid, hepatitis A/E
- Low vaccination coverage (~60%) → measles, polio, pertussis
- Malnutrition → amplifies severity of every infectious disease
- Consanguinity (~60% in Pakistan) → genetic diseases (thalassaemia, CHD, inborn errors)
- Unsafe injection practices → iatrogenic HIV, hepatitis B/C
- Inadequate neonatal care → high neonatal mortality (69.3/1,000 live births)
Sources: Ochsner Journal – Karachi Pediatric ED study | PMC – Sanghar District Hospital cohort | WHO EMRO Pakistan | Pakistan National Health Survey | IHME Global Burden of Disease 2021
we have pneumonia and measles patients . how to treat them and managemnet and also explain about the pathophysiology as I am USMLE aspirant
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
Koplik spots measles buccal mucosa
Reading File
Searching Images
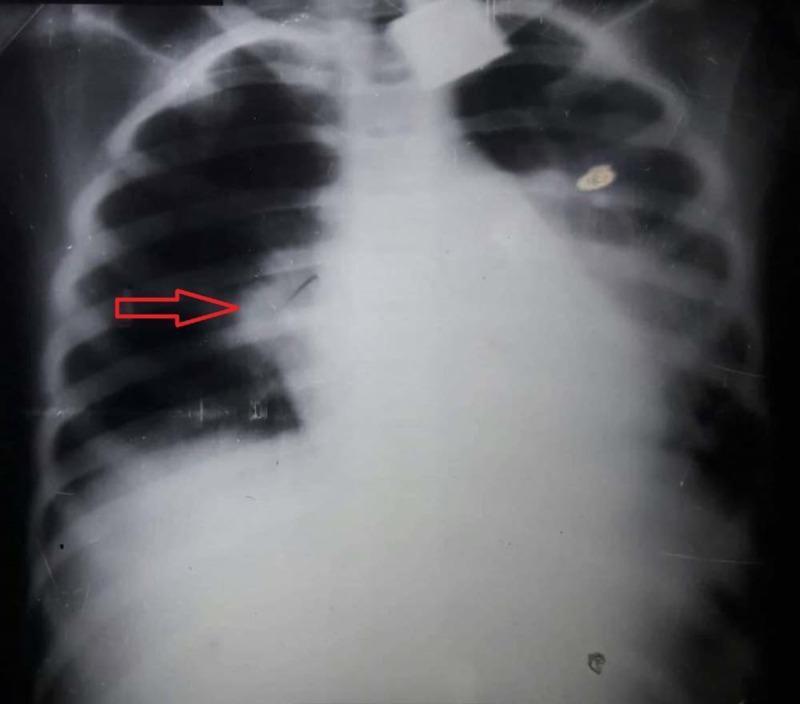
lobar pneumonia consolidation chest X-ray
Reading File
Here is a comprehensive, USMLE-style breakdown of both diseases.
🫁 PART 1: PNEUMONIA
1. Pathophysiology — USMLE Core Concepts
Pneumonia is infection of the lung parenchyma leading to alveolar consolidation — the normally air-filled alveoli fill with exudate (fluid, pus, RBCs, fibrin), causing impaired gas exchange.
Mechanism of Consolidation (4 Classic Stages of Lobar Pneumonia):
| Stage | Timing | Pathology | Gross Appearance |
|---|---|---|---|
| Congestion | Day 1–2 | Vascular engorgement, serous exudate, bacteria multiply | Red, heavy, boggy lung |
| Red Hepatization | Day 3–4 | RBCs + fibrin + neutrophils fill alveoli | Liver-like, red, airless |
| Grey Hepatization | Day 5–7 | RBCs lyse; fibrin + macrophages remain | Grey, firm |
| Resolution | Day 8+ | Enzymatic digestion of exudate, macrophages clear debris | Normal or fibrosis |
USMLE High-Yield: Grey hepatization → WBCs replace RBCs. Failure to resolve → organizing pneumonia or lung abscess.
Why Do Patients Desaturate?
- Alveoli are filled → V/Q mismatch (perfused but not ventilated = intrapulmonary shunt)
- This causes hypoxemia that does NOT correct well with supplemental O₂ (hallmark of shunt physiology)
Inflammatory Cascade:
- Bacteria (e.g., S. pneumoniae) activate complement → C3a/C5a → neutrophil recruitment → cytokine storm (IL-1, IL-6, TNF-α) → fever, consolidation, systemic illness
2. Etiology by Age Group (USMLE-Tested Pattern)
| Age | Organism | Clue |
|---|---|---|
| Neonate (0–4 wks) | Group B Strep, E. coli, Listeria | Vertical transmission from maternal flora |
| 1–3 months | Chlamydia trachomatis | Staccato cough, eosinophilia, no fever |
| 3 months–5 years | RSV/viral, S. pneumoniae, H. influenzae | Most common; RSV = bronchiolitis |
| School age (5–15 yrs) | Mycoplasma pneumoniae ("Walking pneumonia") | Insidious, low fever, headache; cold agglutinins + |
| Adults/all ages | S. pneumoniae | #1 cause of CAP overall; rust-colored sputum |
| Immunocompromised | PCP (P. jiroveci), Aspergillus, CMV | CD4 <200 → PCP |
| Hospital/aspiration | Gram-negatives (Pseudomonas, Klebsiella), MRSA | Right lower lobe if upright, right upper lobe if supine |
USMLE Mnemonics:
- Atypical organisms = Mycoplasma, Chlamydia, Legionella → Macrolide (azithromycin) coverage
- Klebsiella = alcoholic + currant-jelly sputum + upper lobe cavitary
- Legionella = AC units/water cooling towers + hyponatremia + diarrhea → Legionella urinary antigen test
3. Clinical Presentation
Typical (Bacterial — S. pneumoniae):
- Sudden onset high fever, rigors, pleuritic chest pain
- Productive rust-colored sputum
- Lobar consolidation on CXR
- Exam: ↓ breath sounds, dullness to percussion, egophony, bronchial breathing
Atypical (Mycoplasma, Chlamydia, Viral):
- Gradual onset, low-grade fever
- Dry, non-productive cough
- "Worse on X-ray than clinically" (bilateral interstitial infiltrates, patient walks in looking well)
- Extrapulmonary features: bullous myringitis (Mycoplasma), pharyngitis, rash
Pediatric Red Flags:
- Tachypnea disproportionate to fever = earliest sign in children
- Intercostal/subcostal retractions
- Nasal flaring, grunting (infants)
- WHO criteria: RR >50/min (2–12 months), >40/min (1–5 years) = pneumonia
4. Diagnosis
| Test | Finding |
|---|---|
| CXR | Lobar consolidation (bacterial) vs. bilateral interstitial infiltrates (viral/atypical) |
| WBC | >15,000 with left shift (bacterial); leukopenia (viral, atypical) |
| Sputum Gram stain & culture | Gold standard for bacterial ID (low sensitivity in practice) |
| Cold agglutinins (IgM) | Positive in Mycoplasma (auto-agglutination at 4°C) |
| Legionella urinary antigen | Rapid, specific for serogroup 1 |
| Blood cultures | Positive ~25% in bacteremic pneumococcal pneumonia |
CXR: Lobar consolidation (right upper lobe):
5. Treatment & Management
Outpatient (CAP, mild):
| Patient | Drug of Choice |
|---|---|
| Healthy adult, no comorbidities | Azithromycin (macrolide) OR Doxycycline |
| With comorbidities (COPD, DM, heart disease) | Amoxicillin-clavulanate + Azithromycin OR Respiratory fluoroquinolone (levofloxacin) |
| Child < 5 yrs (bacterial suspected) | Amoxicillin 80–90 mg/kg/day (high-dose, covers intermediately resistant S. pneumo) |
| Child (atypical suspected, >5 yrs) | Azithromycin |
Inpatient (Moderate-Severe CAP):
- β-lactam + Macrolide (e.g., Ceftriaxone + Azithromycin) OR
- Respiratory fluoroquinolone (Levofloxacin monotherapy)
ICU / Severe CAP:
- Ceftriaxone + Azithromycin + Vancomycin (if MRSA suspected: post-influenza, necrotic cavities)
Supportive:
- Supplemental O₂ → target SpO₂ ≥94%
- IV fluids if dehydrated
- Antipyretics (Paracetamol/Ibuprofen — avoid aspirin in children → Reye syndrome)
- Severity scores: CURB-65 (adults), PSI; for children → WHO criteria guides step-up
Prevention:
- PCV13/PCV15 (pneumococcal conjugate) — routine childhood immunization
- Influenza vaccine — annually (reduces secondary bacterial pneumonia)
🔴 PART 2: MEASLES (RUBEOLA)
1. Pathophysiology — USMLE Core Concepts
The Virus:
- Paramyxovirus, genus Morbillivirus
- Single-stranded, negative-sense RNA virus
- R₀ = 12–18 (most contagious human pathogen known)
- Transmission: respiratory droplets + airborne (viable in air for up to 2 hours)
- Single serotype → one strain of vaccine protects against all 24 genotypes
Step-by-Step Pathogenesis:
Inhalation of virus
↓
Infects respiratory epithelium via CD150 (SLAM) receptor & Nectin-4
↓
Replication in local lymph nodes → PRIMARY VIREMIA (Day 1–2)
↓
Spreads to RES (liver, spleen, lymph nodes, bone marrow)
→ SECONDARY VIREMIA (Day 5–7)
↓
Dissemination to skin, conjunctiva, respiratory tract, GI tract
↓
Cell-mediated immune response → characteristic RASH (Day 14)
↓
Immunosuppression ("immune amnesia") persists for months–years
USMLE High-Yield — Immune Amnesia: Measles virus depletes pre-existing antibody-secreting B cells → wipes out immunological memory → children become susceptible to other infections they were previously immune to for 2–3 years after measles. This explains excess mortality in the post-measles period.
Why the Rash Appears When It Does:
- The rash is NOT due to direct viral damage — it is the result of the CD4+ T-cell immune response attacking virus-infected endothelial cells in the skin
- Immunocompromised patients (no cellular immunity) → no rash but very high mortality (giant cell pneumonitis)
2. Clinical Presentation — The "3 C's + Rash" Rule
Prodrome (Days 1–4 after symptoms):
Cough + Coryza + Conjunctivitis + High Fever
- Fever can reach 40–41°C (104–106°F) — alarming, prolonged
- Koplik spots appear 1–2 days BEFORE rash → pathognomonic

Koplik spots: 1mm bluish-white papules on erythematous base, on buccal mucosa opposite the lower molars. Fade with rash onset.
Exanthem (Rash — Day 14 after exposure):
- Begins: behind ears → hairline → face
- Spreads: cephalocaudal (head → trunk → extremities) over 3 days
- Character: maculopapular, confluent (unlike rubella which stays discrete)
- Clears in same order it appeared; may desquamate in malnourished children
3. Timeline (USMLE Favorite!)
| Day from Exposure | Event |
|---|---|
| Day 0 | Exposure |
| Days 7–10 | Fever, malaise begin |
| Days 8–12 | Cough, coryza, conjunctivitis |
| Days 9–11 | Koplik spots appear (MOST contagious phase) |
| Day 14 | Rash begins (cephalocaudal spread) |
| Days 14–17 | Rash fully spreads; fever peaks |
| Days 17–20 | Rash fades, fever resolves |
Contagious period: 4 days before to 4 days after rash onset (4+4 rule)
4. Complications (Tested Heavily on USMLE)
| Complication | Mechanism | Details |
|---|---|---|
| Otitis media | Secondary bacterial superinfection | Most common complication |
| Pneumonia | Viral (giant cell) OR secondary bacterial | Leading cause of measles death |
| Croup (laryngotracheitis) | Viral inflammation of subglottis | Barking cough, stridor |
| Febrile seizures | High fever | Common, usually benign |
| Acute Post-Infectious Encephalomyelitis | Autoimmune demyelination | Occurs 2–14 days after rash; 20% fatal, 1/3 have permanent sequelae |
| Measles Inclusion Body Encephalitis | Viral replication in brain (immunocompromised) | 1–6 months post-infection; refractory seizures |
| SSPE (Subacute Sclerosing Panencephalitis) | Defective measles virus persists in CNS | 7–10 years after infection; 4–11/100,000; uniformly fatal |
| Vitamin A deficiency → Xerophthalmia | Measles depletes Vit A | Blindness in malnourished children |
| Immune Amnesia | Depletion of memory B cells | Increased susceptibility to all infections for 2–3 years |
USMLE High-Yield on SSPE: Periodic complexes on EEG + high measles IgG/IgM in CSF + progressive cognitive decline → diagnosis of SSPE
5. Diagnosis
| Test | Finding |
|---|---|
| Clinical | 3 C's + Koplik spots + cephalocaudal rash in unvaccinated child = clinical diagnosis |
| Measles IgM | Positive ≥4–5 days after rash onset (false negative if drawn too early) |
| RT-PCR | Nasopharynx, urine, blood — most sensitive; also genotypes the virus |
| WBC | Leukopenia + lymphopenia (hallmark — contrasts with bacterial infection) |
| Skin biopsy | Syncytial giant cells (Warthin-Finkeldey cells) |
CDC Case Definition: Maculopapular rash ≥3 days + fever ≥38.3°C + at least one of: cough, coryza, or conjunctivitis
6. Treatment & Management
There is NO specific antiviral therapy for measles. Treatment is supportive.
Supportive Care:
- Antipyretics (Paracetamol — not aspirin)
- Oral rehydration / IV fluids
- Nutritional support
- Isolation (droplet + airborne precautions; negative pressure room if available)
- Treat secondary bacterial infections (otitis media, pneumonia) with antibiotics
🌟 Vitamin A — THE KEY TREATMENT (High-Yield for USMLE & Pakistan):
| Age | Dose | Duration |
|---|---|---|
| < 6 months | 50,000 IU | Days 1 and 2 |
| 6–11 months | 100,000 IU | Days 1 and 2 |
| ≥ 12 months | 200,000 IU | Days 1 and 2 |
| + ophthalmic signs | Add 3rd dose | 2–6 weeks later |
Why Vitamin A? Measles → Vitamin A depletion → ↑ morbidity/mortality. Vit A restores epithelial integrity, immune function. WHO recommends for ALL hospitalized children with measles in countries with high deficiency (Pakistan qualifies). Reduces mortality by ~50% in malnourished children.
Neurological Complications:
- No proven therapy for SSPE or measles encephalitis
- Ribavirin, interferon-α, and isoprinosine have limited observational evidence
7. Prevention
| Strategy | Details |
|---|---|
| MMR vaccine | Live attenuated; 2 doses required; 97% effective after 2 doses |
| Dose 1 | 9–12 months (6 months if outbreak/travel to endemic area) |
| Dose 2 | 15–18 months, or school entry (4–6 yrs) |
| Herd immunity threshold | ≥94–95% vaccination coverage needed |
| Post-exposure prophylaxis (within 72 hrs) | MMR vaccine (for susceptible contacts) |
| Post-exposure (within 6 days) | Immune globulin (for immunocompromised, infants, pregnant) |
| Contraindications to MMR | Pregnancy, severe immunocompromise (except HIV if not severely immunosuppressed), anaphylaxis to prior dose |
🧠 USMLE One-Liners Summary
| Fact | Answer |
|---|---|
| Most contagious known pathogen | Measles (R₀ = 12–18) |
| Pathognomonic sign of measles | Koplik spots (bluish-white dots on buccal mucosa) |
| When does rash appear in measles? | Day 14 after exposure; day 2–4 after Koplik spots |
| Rash direction | Cephalocaudal (head → feet) |
| Most common complication of measles | Otitis media |
| Leading cause of measles death | Pneumonia |
| Late fatal complication | SSPE (7–10 years later, uniformly fatal) |
| Treatment of measles | Supportive + Vitamin A |
| Vitamin A dose (>12 months) | 200,000 IU × 2 days |
| Mechanism of measles rash | CD4+ T-cell immune response (not direct viral damage) |
| Pneumonia mechanism of hypoxemia | V/Q mismatch (shunt physiology) |
| Classic bacterial CAP organism | S. pneumoniae (rust sputum, lobar consolidation) |
| "Walking pneumonia" organism | Mycoplasma pneumoniae (cold agglutinins +) |
| Chlamydia trachomatis pneumonia clue | Staccato cough + no fever + eosinophilia (age 6–8 wks) |
| First-line in pediatric CAP (<5 yrs) | High-dose Amoxicillin (80–90 mg/kg/day) |
| Severe CAP inpatient regimen | Ceftriaxone + Azithromycin |
Sources: Textbook of Family Medicine 9e | Goldman-Cecil Medicine (2-vol set) | Harrison's Principles of Internal Medicine 22E (2025) | Andrews' Diseases of the Skin — via the Medical Textbook Library
This is a shared conversation. Sign in to Orris to start your own chat.