About influenza vaccine
"influenza vaccine" effectiveness
influenza vaccine types recommendations 2025 2026
Influenza Vaccine
Overview
Types of Influenza Vaccines
1. Inactivated Influenza Vaccine (IIV) - Egg-based
- Prepared from inactivated, detergent-solubilized virion particles (HA and NA proteins) grown in embryonated chicken eggs.
- Available as trivalent or quadrivalent formulations.
- Administered by intramuscular (or intradermal) injection.
- Standard dose: 0.5 mL for adults; 0.25 mL (or 0.5 mL depending on brand) for children 6-35 months.
- About 60% effective in healthy persons under 65 years.
- 50-60% effective in preventing hospitalization and ~80% effective in preventing death among the elderly.
- Immunity develops within 14 days and lasts 6-12 months.
- Should be stored at 2-8°C and must NOT be frozen.
2. High-Dose IIV (HD-IIV) and Adjuvanted IIV (aIIV) - for adults ≥65 years
- Designed to overcome the waning immune response in older adults.
- HD-IIV contains 4 times the standard HA antigen dose.
- Shown to be 24% more effective than standard-dose IIV in preventing lab-confirmed influenza in the elderly.
- aIIV contains an adjuvant (MF59) to boost immune response.
- Both are trivalent and available only for persons ≥65 years.
- ACIP has preferred HD-IIV (Fluzone High-Dose), adjuvanted IIV (Fluad), or recombinant vaccine (Flublok) for older adults since 2022.
3. Live Attenuated Influenza Vaccine (LAIV)
- Approved in 2003. Contains cold-adapted attenuated viruses that replicate in nasopharyngeal mucosa.
- Administered as a nasal spray (0.2 mL; 0.1 mL per nostril).
- Approved only for healthy, non-pregnant persons ages 2-49 years.
- 87% effective against culture-confirmed influenza in children 60-84 months.
- Also reduces febrile otitis media (27%) and antibiotic use for otitis media (28%) in children.
- Vaccinated children can shed vaccine virus in secretions for up to 3 weeks.
- Does NOT contain thimerosal.
4. Recombinant Influenza Vaccine (RIV - Flublok)
- The HA gene is isolated and expressed in insect cell cultures - completely egg-free.
- Contains 3 times the HA antigen of the standard-dose IIV.
- Licensed for persons 18 years and older.
5. Cell-Cultured Vaccine (ccIIV)
- Grown in animal cells rather than eggs - allows faster manufacturing.
- May contain trace egg proteins despite not using eggs as the primary substrate.
Dosing Schedule
| Age Group | Dose | Number of Doses | Route |
|---|---|---|---|
| 6-35 months | 0.25 or 0.5 mL (brand-dependent) | 1-2* | Intramuscular |
| 3-8 years | 0.5 mL | 1-2* | Intramuscular |
| 9-17 years | 0.5 mL | 1 | Intramuscular |
| ≥18 years | 0.5 mL | 1 | Intramuscular |
| 2-49 years (healthy) | 0.2 mL | 1-2* | Intranasal (LAIV) |
Who Should Be Vaccinated
- All children aged 6-59 months and all persons ≥50 years
- Persons with chronic pulmonary (asthma), cardiovascular, renal, hepatic, neurologic, hematologic, or metabolic disorders (including diabetes)
- Immunocompromised individuals (including HIV)
- Pregnant women (or women who will be pregnant during flu season)
- Children/adolescents on aspirin therapy (Reye syndrome risk)
- Residents of nursing homes or long-term care facilities
- Persons with BMI ≥40
- American Indians/Alaska Natives
- Healthcare workers and household contacts/caregivers of high-risk persons
Contraindications and Precautions
- Children <2 years or persons ≥50 years
- Pregnant women
- Immunocompromised individuals (any cause, including HIV)
- Persons with chronic pulmonary, cardiovascular, metabolic, renal, or hematologic conditions
- Children on long-term aspirin therapy
- Persons with severe egg allergy (LAIV contains residual egg protein)
- History of Guillain-Barre Syndrome (GBS) within 6 weeks of a prior influenza vaccine is a precaution. Generally avoid vaccination in low-risk individuals; however, in high-risk individuals, benefits typically outweigh risks.
- Urticaria only: any licensed influenza vaccine can be given.
- More severe allergic reactions (angioedema, respiratory distress, anaphylaxis): any licensed vaccine can still be used, but it should be administered in a supervised medical setting by a provider capable of managing allergic reactions.
Side Effects
Recent Evidence (2024-2026)
-
Enhanced vaccines in older adults (HD-IIV, aIIV, RIV4) provide superior protection against influenza hospitalization compared to standard-dose vaccines - PMID 39230284.
-
LAIV vs IIV in children: A 2025 network meta-analysis (2003-2023 data) found LAIV to be at least as effective as IIV in children, with strong real-world effectiveness - PMID 40697050.
-
Overall vaccine outcomes: A 2025 meta-analysis found influenza vaccines provide meaningful morbidity benefits (reduced hospitalizations, complications, severe disease) even when infection prevention rates are modest - PMID 39778922.
Vaccine used in Indian settings
influenza vaccine India available brands recommendations IAP NIP 2025
https://acvip.org/professional/columns/influenza-vaccine
influenza vaccine brands available India Vaxigrip Fluarix Nasovac manufacturers
Influenza Vaccine in India
Epidemiological Context
Optimal Timing to Vaccinate in India
Vaccine Types Available in India
1. Inactivated Influenza Vaccine (IIV)
- Quadrivalent IIV is preferred over trivalent IIV (IAP-ACVIP recommendation).
- Available brands include:
- Vaxigrip Tetra (Sanofi Pasteur) - quadrivalent IIV
- Fluarix Tetra (GSK) - quadrivalent IIV
- Influvac Tetra (Abbott/Mylan) - quadrivalent IIV
- Dose: 0.5 mL (15 mcg HA/strain) from 6 months onwards, given intramuscularly.
2. Live Attenuated Influenza Vaccine (LAIV) - Nasal Spray
- NASOVAC-S4 - India's first needle-free seasonal flu vaccine, developed and manufactured by the Serum Institute of India (SII) in collaboration with Mylab Discovery Solutions. This is a landmark product - the only indigenously developed LAIV in India.
- Given as a nasal spray (0.2 mL total; 0.1 mL per nostril).
- For healthy persons 2-49 years of age.
- Especially useful in settings where needle phobia is a concern or injection infrastructure is limited.
IAP-ACVIP Recommendations (Pediatric Use)
| Parameter | Details |
|---|---|
| Minimum age for IIV | 6 months |
| Minimum age for LAIV | 2 years |
| Preferred formulation | Quadrivalent IIV (over trivalent) |
| Universal recommendation (0-5 yrs) | All children 6 months to 5 years |
| 6-18 years | Only high-risk children (see below) |
| LAIV use | Healthy children aged 2-18 years only |
- Chronic cardiac or respiratory disease
- Hematological, renal, or hepatic conditions (including nephrotic syndrome)
- Diabetes mellitus
- Congenital or acquired immunodeficiency (including HIV)
- Children on long-term salicylate therapy
- Laboratory personnel and healthcare workers
Dosing Schedule (IAP India)
- Age 6 months to <9 years: 2 doses, at least 4 weeks apart
- Age 9 years and above: single dose
- If <2 total doses received in past seasons: give 2 doses this season.
- If ≥2 doses received in past (even across different seasons): give 1 dose this season.
LAIV (NASOVAC) - Contraindications in India
- Children <2 years
- Children on aspirin/salicylates (ages 2-17 years)
- Immunocompromised children
- Children with asthma or wheezing in the past 12 months (ages 2-4 years)
- Children with chronic medical conditions
- Those who received influenza antivirals in the previous 48 hours
Key India-Specific Points
| Feature | India |
|---|---|
| Influenza pattern | Year-round with monsoon peak |
| Recommended vaccine timing | May-June (pre-monsoon) |
| Preferred strain | Southern Hemisphere (SH) formulation |
| Preferred formulation | Quadrivalent IIV |
| Indigenous vaccine | NASOVAC-S4 (Serum Institute of India) - nasal LAIV |
| National Immunization Program (NIP) | Influenza vaccine is NOT currently part of India's Universal Immunization Programme (UIP); it is recommended only under IAP guidelines for high-risk and young children |
Best area for Im on shoulder
deltoid muscle IM injection best site landmark acromion shoulder anatomy
deltoid IM injection safe zone triangle acromion axillary nerve SIRVA avoidance
Best Site for IM Injection on the Shoulder - Deltoid Muscle
The Injection Site
Two Landmarking Methods
Method 1 - Finger-breadth Method (CDC / most common)
- Expose the whole upper arm.
- Palpate the acromion process (the bony point at the tip of the shoulder).
- Place 2-3 finger-breadths (approximately 2.5-5 cm) below the lower edge of the acromion process.
- The injection is given at this level, into the middle of the lateral upper arm.
- The lower border is at the level of the axilla (armpit).
- Inject at 90° to the skin, into the center of this zone.
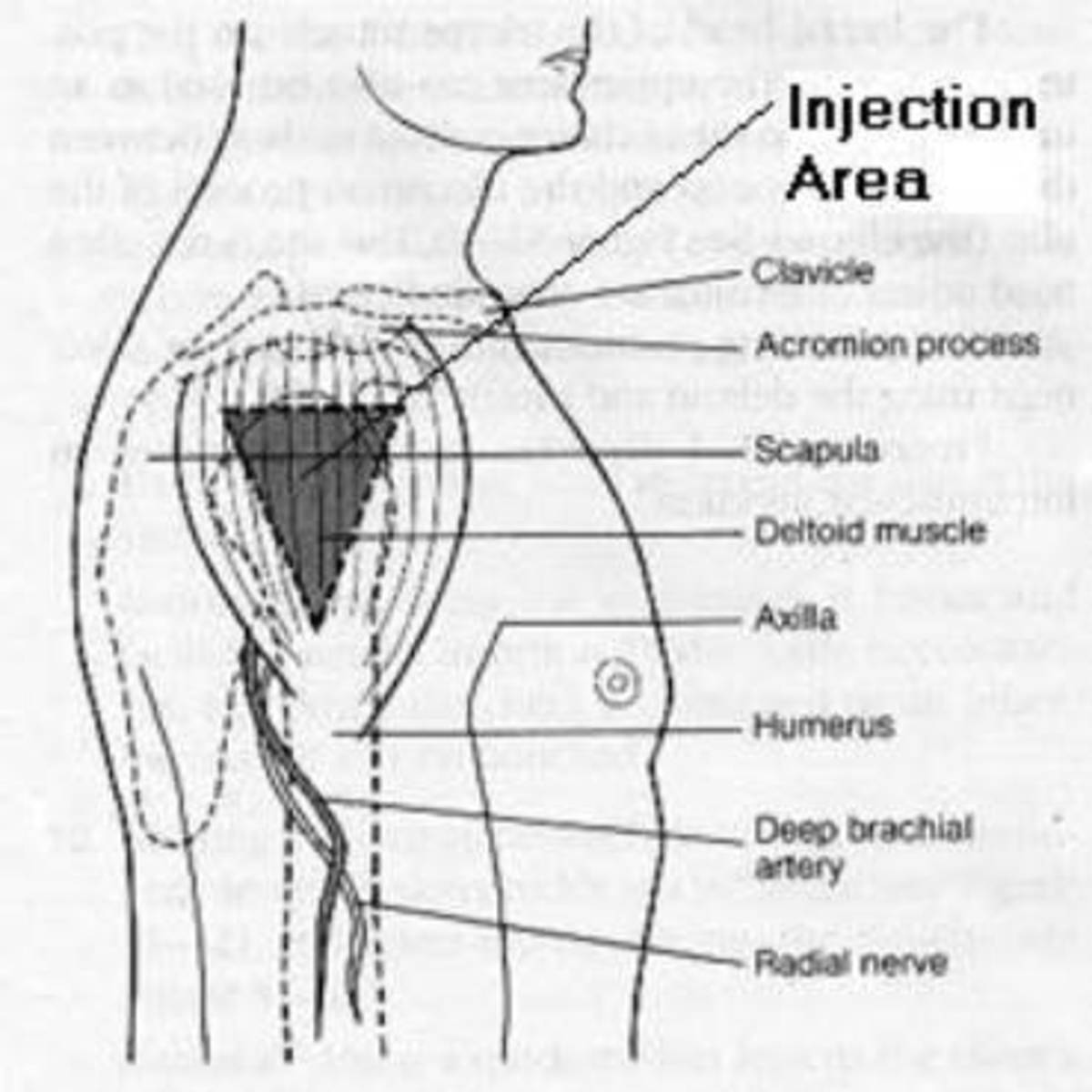
Method 2 - Axillary Triangle Method (more precise)
- Palpate the acromion process - draw an imaginary base line at the lower edge of the acromion.
- The apex (tip) of the triangle points down toward the axillary fold/armpit crease.
- The injection site is the center of this inverted triangle.
- This method is considered more anatomically reliable for identifying the safe zone.
Structures to Avoid
| Too high (above the safe zone) | Too low | Too lateral/posterior |
|---|---|---|
| Shoulder joint / subacromial bursa | Radial nerve | Axillary nerve & posterior circumflex humeral artery |
| Causes SIRVA (Shoulder Injury Related to Vaccine Administration) | Radial nerve palsy | Axillary neuropathy |
Safe Zone Summary
Acromion process (bony tip of shoulder)
|
2-3 finger-breadths below
|
┌──────────────┐ ← UPPER BORDER (safe zone begins here)
│ │
│ SAFE ZONE │ ← INJECT HERE (center of deltoid)
│ (triangle) │
└──────────────┘ ← LOWER BORDER (level of axillary fold)
- Upper border: 2-3 finger-breadths below the acromion
- Lower border: level of the axilla (armpit)
- Lateral border: middle of the lateral arm (avoid going too far posterior or anterior)
Patient Position
- Arm should be relaxed at the side, or have the patient place their hand on their hip with the shoulder slightly abducted (~60°) - this relaxes the deltoid and makes the muscle belly more prominent and easier to target accurately.
Needle Length (Adults)
| Body weight | Needle length |
|---|---|
| <60 kg | 5/8 inch (16 mm) |
| 60-90 kg | 1 inch (25 mm) |
| >90 kg (female) | 1-1.5 inch |
| >90 kg (male) | 1-1.5 inch |
Key Rule to Remember
"Inject into the central and thickest part of the deltoid - never in the upper third."
- Always inject at 90° to the skin surface.
- The influenza vaccine for adults is given IM in the deltoid of the non-dominant arm by convention, though either arm is acceptable.
Show me image
deltoid IM injection site diagram image acromion triangle landmark
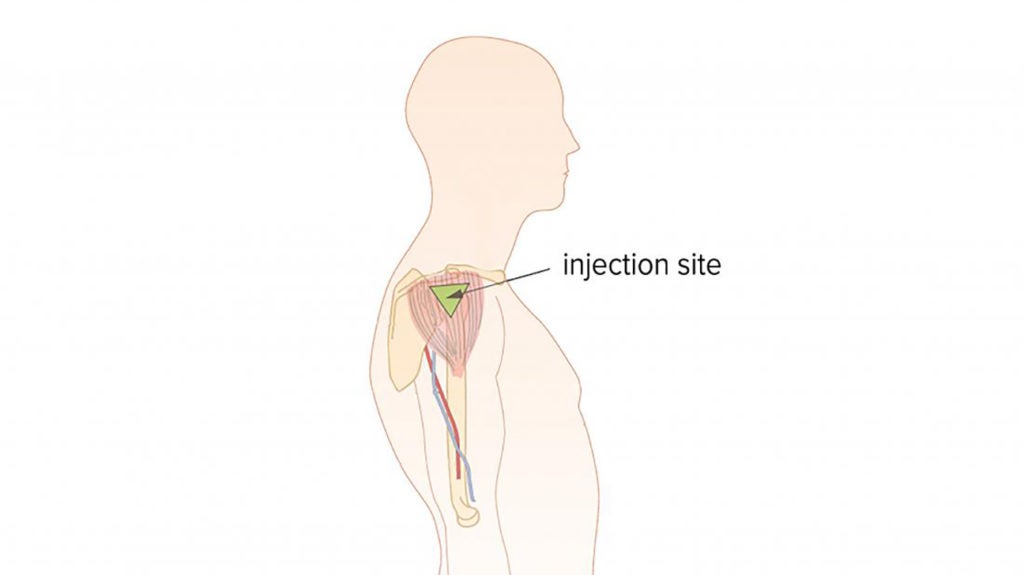
- Injection area = the shaded inverted triangle within the deltoid
- Upper border = just below the acromion process
- Lower border = at the level of the axilla
- Avoid below: Radial nerve and deep brachial artery run inferiorly - going too low risks radial nerve injury
- Avoid above: Too high enters the shoulder capsule/bursa causing SIRVA
Acromion process → go 2-3 finger-breadths down → inject in the center of the inverted triangle → always at 90° to the skin.
Show me image of real life dr. Giving im to patient
A doctor or nurse giving an intramuscular injection into the deltoid muscle of a patient's shoulder. The healthcare professional is holding a syringe at 90 degrees to the skin, inserting the needle into the middle of the outer upper arm. The patient is seated, arm relaxed, sleeve rolled up. Clinical setting, realistic medical photo style.

- Patient seated, sleeve rolled up, arm relaxed at the side
- Needle inserted at 90° to the skin surface
- Injection into the middle of the lateral upper arm - the deltoid muscle belly
- Not too high (avoiding the shoulder joint/bursa) and not too low (avoiding the radial nerve)