Diverticulae in esophagus
Reading File
Finding Sources
Searching PubMed
"esophageal diverticula"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Diverticula of the Esophagus
Classification
Esophageal diverticula are outpouchings of the esophageal wall, classified by location and mechanism:
| Type | Location | Mechanism | Wall composition |
|---|---|---|---|
| Pharyngoesophageal (Zenker's) | Above UES (Killian triangle) | Pulsion (false) | Mucosa + submucosa only |
| Killian-Jamieson | Just below UES | Pulsion (true esophageal) | Mucosa + submucosa |
| Mid-esophageal | Mid thorax | Traction (historically) or pulsion | All layers (true) |
| Epiphrenic | Distal 10 cm, above LES | Pulsion (false) | Mucosa + submucosa |
- True diverticulum - all wall layers herniate
- False (pulsion) diverticulum - only mucosa and submucosa herniate through a muscular defect
1. Zenker's Diverticulum (Pharyngoesophageal)
Most common esophageal diverticulum.
Anatomy & Site
- Posterior outpouching through the Killian triangle (Killian's dehiscence) - bounded above by the oblique fibers of the inferior pharyngeal constrictor and below by the transverse fibers of the cricopharyngeus muscle
- Typically at the level of C5-C6
- Most deviate to the left of midline

Pathogenesis
- Impaired UES opening (diminished, not absent, relaxation) leads to increased hypopharyngeal pressure
- Myogenic degeneration: histologic studies show connective tissue replacement of skeletal muscle fibers and fiber degeneration
- A pulsion mechanism drives mucosa and submucosa through the area of relative mural weakness
- Sometimes called "cricopharyngeal achalasia" (though technically UES does relax)
Epidemiology
- Prevalence 0.01-0.11%; majority asymptomatic at discovery
- Median age ~70 years; male predominance
- Rare under age 30
Symptoms
- Dysphagia (most common, 80-90% of patients)
- Regurgitation of undigested food
- Halitosis
- Neck gurgling or mass
- Aspiration/cough
- ~30% have associated GERD
Complications
- Aspiration pneumonia
- Pill retention
- Ulceration, fistula, hemorrhage
- Squamous cell carcinoma (reported in 0.4% over 53 years)
Diagnosis
- Barium swallow - gold standard; shows the pouch and its size; radiologic field must include the hypopharynx
- Endoscopy - not essential; carry perforation risk due to the posterior diverticular orifice; perform with caution
- Esophageal manometry - can show UES incoordination, hypertensive UES; also locates LES for pH monitoring
Treatment
Asymptomatic - follow clinically.
Symptomatic - surgical or endoscopic intervention; all approaches target the common septum (cricopharyngeus myotomy):
Open Transcervical Approach
- Left-sided neck incision along medial border of sternocleidomastoid
- Complete division of cricopharyngeus + myotomy of upper 3 cm of posterior esophageal wall
- Small diverticula (<2 cm) - myotomy alone
- Large diverticula - diverticulectomy (stapler, with bougie in place) or diverticulopexy (suspension to prevertebral fascia)
- Diverticula >5 cm are typically resected
- Complications (2-3%): esophageal leak, mediastinitis, stenosis, recurrent laryngeal nerve damage
- Recurrence: 5-10%
- Operative mortality <2%
Rigid Endoscopic Technique
- General anesthesia; diverticuloscope placed with one blade in esophagus, one in pouch
- Linear stapler fires across the septum, creating a common cavity
- Limitation: small diverticula (2-3 cm) don't allow proper stapler positioning
Flexible Endoscopic Technique
- Patient in left lateral decubitus; septum divided under direct vision
- Devices used: needle knife, hook knife, or argon plasma coagulation
- Endoclips placed to close the incision
- Both rigid and flexible endoscopic approaches have ~90% success rate
Z-POEM (Per-Oral Endoscopic Myotomy for Zenker's)
- Submucosal injection + mucosotomy ~3 cm proximal to the septum
- Submucosal tunnel created on both sides of the septum
- Cricopharyngeus fibers transected under direct vision; mucosotomy closed with clips
- ~90% good results; ~6% complication rate (perforation, bleeding)
- Long-term data still accumulating
2. Killian-Jamieson Diverticula
- Arise from proximal cervical esophagus below the UES (caudal to cricopharyngeus)
- Less common than Zenker's; less likely to cause dysphagia
- Usually unilateral, left-sided; bilateral in 25%; may coexist with Zenker's
- True esophageal diverticula (below UES, in striated/smooth muscle transition zone)
- Can be confused radiographically with Zenker's
3. Mid-Esophageal Diverticula
Pathogenesis
- Historically: traction diverticula from fibrous adhesions due to adjacent mediastinal lymph node inflammation (tuberculosis, histoplasmosis, sarcoidosis, anthracosis)
- Now most cases are pulsion-type associated with esophageal dysmotility (uncoordinated or high-amplitude contractions)
Presentation
- Dysphagia with or without regurgitation
- Symptoms correlate more with the underlying motility disorder than diverticulum size
Diagnosis
- Barium contrast radiography (usually)
- Manometry to evaluate underlying motility
Treatment
- Asymptomatic: observation
- Symptomatic: surgical diverticulectomy + myotomy (or endoscopic myotomy)
4. Epiphrenic Diverticula
- Herniation of mucosa and submucosa through the distal 10 cm of esophageal musculature
- Most commonly caused by functional LES obstruction due to motility disorders (achalasia, diffuse esophageal spasm), or mechanical obstruction (leiomyoma, stricture, web, prior surgery)
- More commonly protrude to the right
- Can enlarge over time (16% in one series over 12 years)
Symptoms
- Dysphagia, regurgitation, odynophagia, chest pain, heartburn, aspiration
- Often asymptomatic (incidentally found)
Diagnosis
- Barium radiography (primary)
- Endoscopy to exclude structural obstruction
- Esophageal manometry - essential to evaluate underlying motility disorder
Treatment
- Symptomatic: diverticulectomy + LES myotomy + partial fundoplication (to prevent reflux post-myotomy); laparoscopic transhiatal approach is established
- Botulinum toxin A injection of LES - limited utility (moderate efficacy, poor durability)
5. Esophageal Intramural Pseudodiverticulosis
A rare, distinct entity (<1% of esophageal radiologic studies):
- Multiple small outpouchings from dilation of excretory ducts of submucosal esophageal glands (not true diverticula)
- First described by Mendl et al. (1960)
- Presents after 6th decade with chronic dysphagia
- Associated with proximal esophageal strictures (70-90%) and manometric abnormalities (two-thirds)
- Also associated with corrosive esophageal injury
- Best diagnosed on barium studies (intramural contrast tracking in 50%)
- Diverticula can regress after stricture treatment
Summary Comparison
| Feature | Zenker's | Mid-esophageal | Epiphrenic |
|---|---|---|---|
| Location | Pharyngoesophageal junction | Mid-thorax | Distal 10 cm |
| Mechanism | Pulsion | Traction/Pulsion | Pulsion |
| Type | False | True (traction) / False (pulsion) | False |
| Associated disorder | UES dysfunction | Motility/TB | Achalasia/DES |
| Key symptom | Regurgitation/halitosis | Dysphagia | Dysphagia/chest pain |
| Treatment | UES myotomy ± resection | Diverticulectomy + myotomy | Diverticulectomy + LES myotomy + fundoplication |
Sources: Yamada's Textbook of Gastroenterology (7th ed.), Goldman-Cecil Medicine, Sabiston Textbook of Surgery, Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Oesophageal cancers
Finding Sources
Searching PubMed
"esophageal neoplasms"[MeSH Terms] AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have extensive material from Harrison's, Sabiston, and Yamada's for a comprehensive answer. Let me compile this.
Oesophageal Cancers
Epidemiology
Oesophageal cancer is the 7th most common cancer and the 6th leading cause of cancer mortality worldwide, with approximately 604,000 new cases and 544,000 deaths in 2020. The 5-year overall survival remains only ~20%, largely because most patients are diagnosed at an advanced stage (only 18% have early-stage disease at presentation).
- Predominant in the 6th and 7th decades; ~70% of cases occur in males
- Highest incidence: Central Asian "esophageal cancer belt" (Iran, Central Asian republics, China), Southern/Eastern Africa, Northern Europe
- In the United States: 17th most common cancer (~21,560 new diagnoses, ~16,120 deaths/year, 2023 estimates)
Types / Histology
Two predominant histologic subtypes with fundamentally different epidemiology, risk factors, genomics, and biology:
| Feature | Adenocarcinoma (EAC) | Squamous Cell Carcinoma (ESCC) |
|---|---|---|
| Global prevalence | More common in North America, Western Europe | Most common worldwide |
| Location | 80% distal esophagus or GEJ | Upper third (10-20%), Middle third (50%), Lower third (40%) |
| Sex | Male predominance | Male predominance (3-4x) |
| Key risk factors | GERD, Barrett's esophagus, obesity | Tobacco + alcohol (synergistic 3x risk) |
| Precursor lesion | Barrett's metaplasia → dysplasia | Squamous dysplasia / high-grade intraepithelial neoplasia |
| Genomic profile | Resembles gastric adenocarcinoma | Resembles HPV-negative head-and-neck SCC |
Other rare types
- Leiomyosarcoma
- Small cell carcinoma
- Melanoma (rare primary)
- Lymphoma (rare)
Risk Factors
Squamous Cell Carcinoma
- Tobacco and alcohol - strongest risk factors; synergistic ~3-fold increased risk with both combined
- Risk increases with amount consumed and cigarettes smoked
- Low fruit and vegetable intake; vitamin/nutrient deficiencies
- Foods containing N-nitrosamines, pickled vegetables, high-temperature liquids (hot tea in Iran, mate in South America)
- Areca (betel) nut chewing (India)
- Chronic achalasia
- Plummer-Vinson (Patterson-Kelly) syndrome (iron deficiency anemia, esophageal webs)
- Caustic (lye) ingestion
- Prior radiation therapy (for Hodgkin's lymphoma, breast cancer)
- Hereditary: Tylosis (RHBDF2 gene mutation) - markedly increased SCC risk; Fanconi anemia
Adenocarcinoma
- GERD - major risk factor; leads to Barrett's metaplasia
- Barrett's esophagus (BE) - risk of progression to cancer ~0.4-0.5% per year
- Obesity (increases reflux; note: many young EAC patients are fit without obesity)
- Tobacco use
- H. pylori infection is inversely correlated (protective for EAC)
- Hereditary: Lynch syndrome, BRCA germline mutations (modest increased risk)
Pathogenesis
ESCC
- Repeated toxin exposure + chronic inflammation → squamous dysplasia → high-grade intraepithelial neoplasia (carcinoma in situ, no basement membrane violation)
- Risk of progression from intraepithelial neoplasia to SCC: 24% at 14 years (low-grade), 50% (moderate-grade), 75% (high-grade)
- Penetration of basement membrane = invasive carcinoma
- Key genomic: TP53 mutation (most prevalent); oncogene amplification of CCND1, MYC, CDK6, EGFR, FGFR ligands
EAC
- Chronic acid exposure → columnar metaplasia (Barrett's) → dysplasia → adenocarcinoma
- Genetic accumulation: TP53 inactivation → overexpression of ERBB2 (HER2), KRAS, CCNE1
- HER2/ERBB2 amplification in ~20-25% of EAC/GEJ adenocarcinomas
- Microsatellite instability (MSI) and EBV infection can drive a subset
Clinical Features
Symptoms
- Progressive dysphagia - most common (initially solids, then liquids) - usually indicates >50% luminal obstruction, hence late presentation
- Odynophagia (painful swallowing)
- Unintentional weight loss
- Regurgitation
- Chest pain or retrosternal discomfort
- Cough, hoarseness (recurrent laryngeal nerve involvement)
- Hematemesis / melena (bleeding)
- Fatigue (anemia from occult bleeding)
Signs
- Cachexia (advanced disease)
- Left supraclavicular lymphadenopathy (Virchow's node)
- Cervical lymphadenopathy
- Hepatomegaly (metastatic disease)
Diagnosis and Workup
- Upper endoscopy + biopsy - establishes diagnosis and histology; biopsy at presentation determines histology and guides molecular testing
- Next-generation sequencing (NGS) / molecular diagnostics - should be performed on all metastatic disease to guide targeted therapy; PD-L1 by IHC; HER2 testing
- CT scan (chest/abdomen/pelvis) - assess metastatic disease
- FDG-PET/CT - assess for metastatic disease, especially occult metastases
- Endoscopic ultrasound (EUS) - most accurate for T and N staging; tumor appears hypoechoic against alternating hyperechoic/hypoechoic wall layers
- Bronchoscopy - for mid/upper esophageal tumors to rule out tracheobronchial invasion (invasion of trachea = unresectable)
- Laparoscopy - for GEJ tumors, to assess peritoneal involvement
- Esophageal manometry - if motility disorder suspected
- Circulating tumor DNA (ctDNA) - emerging tool for detecting genomic alterations and assessing minimal residual disease
Staging (AJCC 8th Edition TNM)
The 8th edition separates staging into clinical (cTNM), pathologic (pTNM), and post-neoadjuvant pathologic (ypTNM) groups, with separate stage groupings for SCC and adenocarcinoma.
T Stage (Depth of invasion)
| Stage | Definition |
|---|---|
| Tis | High-grade dysplasia; malignant cells confined to epithelium, no basement membrane penetration |
| T1a | Invades lamina propria or muscularis mucosa |
| T1b | Invades submucosa |
| T2 | Invades muscularis propria |
| T3 | Invades adventitia (no surrounding structures) |
| T4a | Invades resectable adjacent structures (diaphragm, pleura, pericardium) |
| T4b | Invades unresectable structures (trachea, aorta) |
N Stage
- N0: No regional LN metastasis
- N1: 1-2 regional LNs
- N2: 3-6 regional LNs
- N3: ≥7 regional LNs
M Stage
- M0: No distant metastasis
- M1: Distant metastasis
Key prognostic note: T3-T4 cancers have >80% probability of nodal spread and generally require neoadjuvant therapy. T1-T2 cancers are more likely N0 and may be treated with upfront resection.
For GEJ adenocarcinomas: tumors with epicenters ≤2 cm into the gastric cardia are staged/treated as esophageal; those extending further distally (Siewert III) are staged/treated as gastric cancers.
Treatment
Screening / Surveillance
- General population screening not recommended in low-incidence countries (no proven cost-effective biomarkers)
- Periodic endoscopy recommended for high-risk patients (Barrett's esophagus with dysplasia)
Stage-Based Treatment Overview
Early-Stage Disease (Tis / T1a, selected small T1b)
- Endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) for tumors <2 cm
- EMR/ESD also used as part of staging to confirm T stage
- Ablative therapy (RFA, cryotherapy) for Barrett's eradication
- Esophagectomy if endoscopic therapy not feasible
Locally Advanced Disease (T2-T4, N+)
Standard of care is multimodal therapy - surgery alone is inferior:
CROSS Trial (2012): Carboplatin/paclitaxel + concurrent RT (41.4 Gy, 23 fractions) → surgery vs. surgery alone
- pCR: 49% for SCC, 29% for EAC
- Median OS: 49.4 months (neoCRT) vs. 24 months (surgery alone)
- R0 resection: 92% vs. 69%
NEOCRTEC Trial (2018, SCC only): Vinorelbine/cisplatin + RT → surgery
- 5-year OS: 47% vs. 34%; pCR 43.2%
Perioperative chemotherapy (for adenocarcinoma):
- MAGIC trial: Epirubicin + cisplatin + 5-FU (ECF) pre/post-op → improved 5-year OS (36% vs. 23%)
- FLOT regimen (docetaxel, oxaliplatin, leucovorin, 5-FU): In the ESO-PEC trial, preoperative FLOT improved survival compared to CROSS chemoradiation for locally advanced adenocarcinoma - now a preferred regimen
For SCC of upper/mid esophagus:
- Definitive chemoradiation (without surgery) is a standard option
- Surgery reserved for patients not achieving complete response
Adjuvant Therapy (post-surgery)
- CheckMate 577 trial: Nivolumab (PD-1 inhibitor) adjuvant therapy significantly improved survival in esophageal/GEJ cancer patients who received preoperative chemoradiation + R0 resection but had residual tumor in specimen (not ypT0N0M0) - now standard of care
Metastatic Disease (Palliative Intent)
- Goal: symptom palliation + life extension
- HER2-positive (~20-25%): Trastuzumab + chemotherapy; or trastuzumab + chemotherapy + pembrolizumab (improves PFS)
- HER2-negative, PD-L1 positive: PD-1 inhibitors (e.g., nivolumab, pembrolizumab) + chemotherapy as first-line
- Checkpoint inhibitors are also second-line monotherapy for PD-L1 expressing tumors
- Systemic therapy regimens: platinum-based combinations (cisplatin/oxaliplatin + 5-FU/capecitabine)
Molecular Targets Summary
| Tumor Type | Biomarker | Assay | Therapy |
|---|---|---|---|
| Esophageal SCC | PD-L1 | IHC | PD-1 inhibitor |
| Esophageal Adeno/GEJ | HER2/ERBB2 | IHC/FISH | Trastuzumab |
| Esophageal Adeno/GEJ | PD-L1 | IHC | PD-1 inhibitor |
| Esophageal Adeno/GEJ | MSI-H | PCR/IHC | Pembrolizumab |
| Esophageal Adeno/GEJ | BRCA mutation | NGS | Platinum agents |
| Lynch syndrome | MMR deficiency | IHC | Immunotherapy |
Surgical Approaches
- Esophagectomy (transthoracic/transhiatal/minimally invasive) remains the cornerstone for resectable disease
- High-volume centers and surgeons have markedly better outcomes
- Minimally invasive esophagectomy (MIE) - non-inferior to open (TIME trial) with reduced pulmonary complications
Palliation
- Esophageal stenting (self-expanding metal stents) for malignant dysphagia
- Laser therapy / photodynamic therapy for luminal obstruction
- Radiotherapy for dysphagia palliation
- Nutritional support (feeding jejunostomy, gastrostomy)
Prognosis
5-year overall survival by stage:
- Localized (early): ~47% (esophageal SCC), 47% (EAC)
- Regional (lymph node spread): ~26%
- Distant (metastatic): ~5%
- Overall (all stages): ~20%
From 1973-2010, 5-year OS improved from 3.6% to 21.1% for SCC and from 5.4% to 24.2% for EAC - improvement attributed to better multimodal therapy, higher-volume surgery, and improved radiation delivery.
Sources: Harrison's Principles of Internal Medicine 22E (2025), Sabiston Textbook of Surgery, Yamada's Textbook of Gastroenterology (7th ed.), Goldman-Cecil Medicine
Recent evidence note (PubMed, 2025): Recent meta-analyses (PMID 40207218, PMID 40386769) confirm that PD-1/PD-L1 inhibitors + chemotherapy as first-line treatment for advanced gastroesophageal junction/esophageal adenocarcinoma significantly improve overall survival and progression-free survival in both HER2-negative and HER2-positive subgroups, supporting integration of immunotherapy into standard first-line regimens.
Surgeries for esophageal cancers
Finding Sources
Searching PubMed
"esophagectomy"[MeSH Terms] AND "surgical procedures"[MeSH Terms]
Finding Sources
Searching PubMed
"esophagectomy"[MeSH Terms] AND outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive data. Let me compile the full surgical answer.
Surgeries for Oesophageal Cancer
Overview and Patient Selection
Surgery remains the cornerstone of curative treatment for resectable oesophageal cancer. Esophagectomy is recommended for any case without invasion of unresectable structures (trachea, aorta) or distant metastatic disease. However, because esophagectomy traverses three body compartments (neck, chest, abdomen), it is one of the most technically complex and physiologically demanding operations in surgery.
Key principle: Surgical resection is pursued in less than half of all potentially resectable stage I-III cancers, largely because of historically high morbidity and mortality. The most important determinant of outcome is not technique choice but surgeon and institutional volume - mortality rates differ by ~50% between low- and high-volume centers.
Preoperative Assessment
Before esophagectomy:
- Upper endoscopy - confirm tumor location and plan approach
- Bronchoscopy - for mid or upper third tumors to exclude tracheobronchial invasion
- Nutritional assessment - malnutrition is common; a feeding jejunostomy is often placed
- Pulmonary function testing - single-lung ventilation required for thoracic approaches
- Cardiopulmonary fitness - cardiac risk stratification essential
- Staging CT + PET/CT + EUS - to confirm resectability
The Esophageal Conduit
After esophagectomy, gastrointestinal continuity must be restored. The conduit options are:
| Conduit | Use | Notes |
|---|---|---|
| Stomach (gastric conduit) | First choice in >95% of cases | 3-5 cm wide gastric tube; single blood supply (right gastroepiploic artery); simplest and most reliable |
| Colon interposition | When stomach unavailable (prior gastrectomy, gastroparesis) | Longer operation; requires three anastomoses; isoperistaltic or antiperistaltic |
| Jejunal interposition | Less common; for short-segment replacement | Free jejunal graft with microvascular anastomosis for pharyngeal defects |
A pyloroplasty or botulinum toxin injection of the pylorus is routinely performed to aid gastric conduit emptying (prevents delayed gastric emptying/outlet obstruction post-vagotomy).
The Four Major Surgical Approaches
1. Ivor Lewis Esophagectomy (Two-field / Transthoracic)
Most commonly performed worldwide.
- Incisions: Abdominal (laparotomy or laparoscopy) + Right thoracotomy (right posterolateral, 5th intercostal space) or thoracoscopy
- Patient positioning: Supine (abdominal phase) → Left lateral decubitus (thoracic phase)
- One-lung ventilation: Required (double-lumen ETT or capnothorax)
- Anastomosis: Right intrathoracic (high in the chest, above azygos vein)
- Order of operation: Abdomen first → then thorax
Steps:
- Abdominal phase: D2 lymph node dissection at celiac trunk, hepatic and left gastric artery; gastric conduit creation (3-5 cm wide, stapled from incisura to fundus); pyloroplasty; transhiatal dissection of the distal esophagus
- Patient repositioned; right thoracotomy/thoracoscopy
- Azygos vein divided
- Thorough posterior mediastinal lymphadenectomy
- Esophagus divided; gastric conduit pulled up into thorax
- Intrathoracic esophagogastric anastomosis (end-to-side or end-to-end; stapled or hand-sewn)
Best for: Mid and distal esophageal tumors; GEJ tumors
Advantages:
- Excellent direct visualization of the thoracic esophagus
- Superior mediastinal lymphadenectomy
- Lower anastomotic leak rate than cervical anastomosis
- Less GERD post-op (anastomosis high in chest)
Disadvantages:
- If anastomotic leak occurs in the chest - more dangerous, often requires reoperation or stenting
- Requires one-lung ventilation; higher pulmonary morbidity
- Longer recovery
2. McKeown Esophagectomy (Three-incision / Three-field)
- Incisions: Right thoracotomy/thoracoscopy + Abdominal (laparotomy/laparoscopy) + Left cervical
- Patient positioning: Left lateral decubitus (thoracic) → Supine with neck extension (abdominal + cervical)
- One-lung ventilation: Required
- Anastomosis: Left cervical (neck)
- Order of operation: Right thoracic first → Abdominal → Left cervical
Steps:
- Right thoracoscopy/thoracotomy: esophageal mobilization from thoracic inlet to hiatus; mediastinal lymphadenectomy; azygos vein ligated
- Abdominal phase: gastric conduit creation; D2 nodal dissection; pyloroplasty
- Left cervical incision (anterior to SCM): cervical esophagus freed, divided; specimen extracted through neck; gastric conduit pulled to neck; cervical anastomosis constructed (single-layer interrupted silk or stapled posterior row)
Best for:
- Mid and upper thoracic tumors near the airways (where proximal margin is at risk)
- Extensive Barrett's esophagus requiring maximal esophageal resection
- Concern for adequate proximal margin
Advantages:
- Maximal proximal margin - widest possible excision
- Access to all mediastinal nodal stations (two-field or three-field dissection)
- Cervical leak (if occurs) is much less morbid than intrathoracic leak
- Avoids severe post-op GERD (less residual esophageal mucosa)
Disadvantages:
- Three separate incisions/positions
- Highest rate of recurrent laryngeal nerve (RLN) injury (vocal cord palsy 2-14%)
- Higher anastomotic leak rate at the cervical site than intrathoracic
- Longer operative time
3. Transhiatal Esophagectomy (THE)
- Incisions: Abdominal (laparotomy/laparoscopy) + Left cervical only - no thoracotomy
- Patient positioning: Supine throughout
- One-lung ventilation: Not required
- Anastomosis: Left cervical
- Key feature: Mediastinal esophageal dissection performed bluntly via the diaphragmatic hiatus (surgeon's hand passed into mediastinum) and from the neck downward
Steps:
- Abdominal phase: same as Ivor Lewis; gastric conduit creation; pyloroplasty; hiatus dilated; surgeon's hand inserted transhiatally into posterior mediastinum to bluntly free the thoracic esophagus
- Left cervical incision: cervical esophagus dissected downward; esophagus divided in neck; specimen pulled down through hiatus into abdomen
- Gastric conduit passed through posterior mediastinum to neck; cervical anastomosis
Best for:
- Lower esophageal early-stage disease (T1-T2)
- Barrett's esophagus with high-grade dysplasia (lymph node dissection less critical)
- Patients with poor pulmonary function who cannot tolerate one-lung ventilation
Advantages:
- Least invasive - no thoracotomy, no one-lung ventilation
- Shortest operative time
- Lower pulmonary morbidity
- Cervical anastomotic leaks less dangerous (drain to skin rather than into pleural cavity)
- Excellent functional outcomes and quality of life
Disadvantages:
- Limited lymphadenectomy (cannot access mediastinal nodes as thoroughly)
- Higher anastomotic leak rate (cervical)
- Higher rate of RLN injury
- Intraoperative cardiac dysrhythmias during blunt mediastinal dissection (up to 65% - usually atrial, mostly tolerated)
- Rare but serious: hemorrhage (<2%), airway injury (<1%) from blind mediastinal dissection
- Many consider it to have lower oncologic yield for advanced tumors
4. Left Thoracoabdominal Esophagectomy
- Incisions: Single left thoracoabdominal incision (chest + abdomen through the same incision extended across the costal margin)
- Patient positioning: Supine with chest bumped 45 degrees
- One-lung ventilation: Yes
- Anastomosis: Left chest
- Best for: Cardia and GEJ tumors, re-do cases, patients where prior abdominal surgeries make separate abdominal access difficult
Advantages:
- Excellent exposure to distal esophagus, GEJ, and proximal stomach
- Single incision (no repositioning)
Disadvantages:
- Limited access to the upper mediastinum and proximal esophagus
- High risk of post-op GERD due to low position of intrathoracic anastomosis
- Restricted use compared to the other three approaches
Comparison Summary
| Feature | Transhiatal (THE) | Ivor Lewis (IL) | McKeown (3-field) | Left Thoracoabdominal |
|---|---|---|---|---|
| Incisions | Abdomen + Neck | Abdomen + Right chest | Right chest + Abdomen + Neck | Left chest-abdomen |
| Anastomosis | Left cervical | Right intrathoracic | Left cervical | Left intrathoracic |
| One-lung ventilation | No | Yes | Yes | Yes |
| Lymphadenectomy | Limited | Good | Best (3-field) | Limited to lower mediastinum |
| Anastomotic leak rate | Higher (but less dangerous) | Lower (but more dangerous) | Higher (but less dangerous) | Moderate |
| RLN injury | Moderate | Low | Highest | Low |
| Best for | Early distal disease; poor pulmonary reserve | Mid/distal/GEJ tumors | Upper/mid tumors; long Barrett's | GEJ/cardia; re-do surgery |
| GERD post-op | Less | More | Least | Most |
Minimally Invasive Esophagectomy (MIE)
All of the approaches above can be performed with laparoscopic, thoracoscopic, and/or robotic techniques. MIE is increasingly the standard at high-volume centers.
Definition: An operation where no retraction/lifting of the chest or abdominal wall occurs, and the surgeon visualizes via a monitor; tissue is manipulated only by instruments. Procedures with only one minimally invasive component are "hybrid."
Evidence:
- TIME Trial (2012): MIE (thoracoscopic + laparoscopic) vs. open Ivor Lewis - MIE had significantly fewer pulmonary complications (9% vs. 29%) with equivalent oncologic outcomes (R0 resection, lymph node yield)
- ECOG E2202 trial (16 institutions): 30-day MIE mortality 2%
- University of Pittsburgh series (222 patients): median ICU stay 1 day, median hospital stay 7 days, 30-day mortality 1.4%
- High-volume experienced centers report mortality as low as 0.9%
Advantages of MIE:
- Fewer pulmonary complications
- Shorter ICU and hospital stay
- Less blood loss
- Faster recovery
- Equivalent oncologic outcomes (lymph node yield, R0 rate, survival) to open
Robotic esophagectomy: Feasible; may benefit the surgeon more than the patient. A recent NSQIP analysis found no significant difference in 30-day postoperative outcomes between robotic and other MIE approaches.
Lymph Node Dissection
The extent of lymphadenectomy is an important oncologic determinant:
- Two-field dissection: Abdominal + mediastinal nodes (standard for most cases)
- Three-field dissection: Abdominal + mediastinal + bilateral cervical nodes - performed for upper thoracic SCC or tumors at/above the carina; associated with higher morbidity but improved staging and potentially improved survival in SCC
- Transthoracic approaches provide better access to relevant mediastinal nodes than transhiatal approaches
- A minimum of 15-20 lymph nodes recommended for adequate staging
Resection Classification (AJCC)
| Category | Meaning |
|---|---|
| R0 | No residual tumor (complete resection) - goal of curative surgery |
| R1 | Microscopic residual tumor (positive margins) |
| R2 | Macroscopically visible residual tumor |
Proximal and distal surgical margins of at least 5 cm are desired.
Complications
Intraoperative
- Cardiac dysrhythmias: up to 65% (mainly during transhiatal blunt dissection; mostly atrial, well-tolerated)
- Hemorrhage: <2% (transhiatal); may require emergency thoracotomy
- Airway injury (trachea/bronchi): <1% - detected by smell of inhaled anesthetic; management by advancing ETT past injury, possible primary repair
Perioperative Morbidity (30-50% of patients have at least one serious complication)
| Complication | Incidence |
|---|---|
| Anastomotic leak | 6-14% |
| Anastomotic stricture | 16-48% |
| Conduit (gastric) necrosis | 0.5-2% |
| Vocal cord palsy (RLN injury) | 2-14% |
| Chylothorax | 0.8-9% |
| Pneumonia | 8-26% |
| Atrial fibrillation | 14-17.5% |
| Delayed gastric emptying | 1.8-3.7% |
| Respiratory failure | 1.8-16% |
| Wound infection | 5.3-12% |
| Renal failure | 0.9-3.4% |
| DVT | 0.9-2% |
| MI | 0.7-1.2% |
Key complication management:
- Anastomotic leak: 57% managed non-operatively; options include endoscopic stenting (if small/contained), primary repair, muscle flap reinforcement, esophageal diversion. Early leaks (<5 days) or those with conduit necrosis often need surgery
- Chylothorax: NPO + TPN for low output; thoracic duct embolization (IR) or surgical ligation for high output
- Anastomotic stricture: Endoscopic dilation (up to 3 dilations needed in 6.6% of patients)
- Atrial fibrillation: Electrolyte correction, antiarrhythmics; always prompt workup for anastomotic leak
Mortality and Volume-Outcome Relationship
| Centre volume (esophagectomies/year) | Mortality |
|---|---|
| 1-10 per year | ~12.1% |
| 11-20 per year | ~7.5% |
| >50 per year | ~4.9% |
| High-volume experienced centres (MIE) | As low as 0.9-2% |
Specialty training reduces mortality by 37-50% vs. non-specialty surgeons. Institutional volume (>12/year) and surgeon volume (>5/year) are the most important predictors of outcome beyond surgical technique choice.
Post-Esophagectomy Quality of Life
- Most patients report good satisfaction with life after gastric conduit replacement
- Long-term issues: dysphagia (from stricture), early satiety, loss of appetite, reflux
- Post-op GERD is more common with intrathoracic anastomoses (Ivor Lewis, left thoracoabdominal) vs. cervical anastomoses
- SF-36 scores in patients operated for high-grade dysplasia/early cancer generally equal healthy controls at ~46 months post-op
- Patients who had esophagectomy report more reflux and eating problems vs. endoscopic therapy patients; endoscopy patients report higher fear of cancer recurrence
Sources: Mulholland & Greenfield's Surgery (7th ed.), Current Surgical Therapy (14th ed.), Yamada's Textbook of Gastroenterology (7th ed.)
Recent evidence (PubMed 2024): A meta-analysis (PMID 38869981) comparing mediastinoscopy-assisted vs. thoracoscope-assisted esophagectomy found comparable perioperative outcomes and long-term survival, supporting both as valid minimally invasive options depending on institutional expertise.
Courvoisier law
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Courvoisier's Law
The Statement
"In the presence of jaundice, a palpable, non-tender, distended gallbladder is unlikely to be due to gallstones, and is more likely caused by malignant (neoplastic) obstruction of the common bile duct."
Conversely: if the gallbladder is not palpable in an icteric patient, gallstones are the more probable cause.
First described by the Swiss surgeon Ludwig Courvoisier in 1890, when he noted the association between an enlarged gallbladder and a pancreatic tumour.
The Diagram
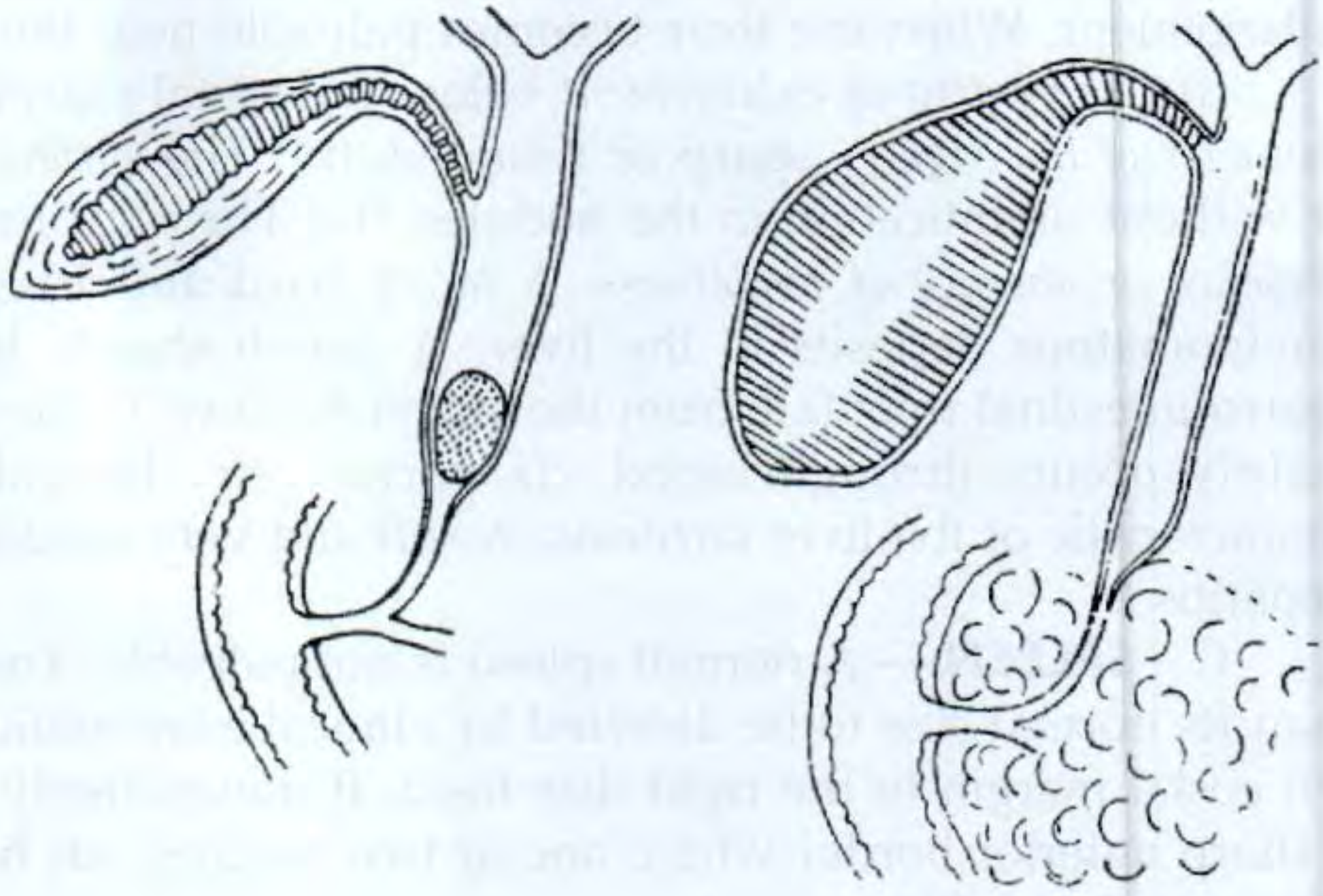
Left: Gallstone in the CBD - gallbladder is shrunken and fibrosed (non-distensible). Right: Carcinoma of the head of the pancreas obstructing the distal CBD - the normal gallbladder distends massively (Courvoisier's sign).
Pathophysiological Basis
The law rests on a fundamental difference in how the two causes of biliary obstruction affect the gallbladder wall:
| Feature | Gallstone obstruction | Malignant obstruction |
|---|---|---|
| Onset | Chronic, recurrent | Gradually progressive |
| Prior inflammation | Yes - repeated bouts of cholecystitis | No prior disease |
| Gallbladder wall | Thick, fibrosed, shrunken (from chronic inflammation) | Thin, pliable, normal |
| Response to rising biliary pressure | Cannot distend (scarred wall) | Distends readily - "blown up" like a balloon |
| Result | Non-palpable gallbladder | Palpably enlarged, tense, non-tender gallbladder |
Key mechanism: Patients with gallstones causing common bile duct (CBD) obstruction almost always have had recurrent cholecystitis, leading to progressive fibrosis of the gallbladder wall. This fibrosed, thickened wall cannot expand when biliary pressure rises. In contrast, malignancy obstructing the distal CBD (e.g., carcinoma of the head of the pancreas, cholangiocarcinoma, ampullary tumour) causes progressive obstruction in a previously normal gallbladder, which distends in an attempt to decompress rising biliary pressure.
Causes of a Positive Courvoisier Sign (Palpable Gallbladder + Jaundice)
These are causes of distal CBD obstruction in a gallbladder not previously diseased:
- Carcinoma of the head of the pancreas - most common cause
- Periampullary carcinoma (carcinoma of the ampulla of Vater)
- Cholangiocarcinoma (distal bile duct)
- Carcinoma of the gallbladder (rare)
- Duodenal carcinoma with bile duct involvement
- Metastatic nodes at the porta hepatis compressing the CBD
- Mirizzi syndrome (less common - stone in the cystic duct/Hartmann's pouch externally compressing the CBD; but the gallbladder may still be palpable in this case)
- High insertion of the cystic duct (anatomical variant - a Courvoisier's gallbladder with high cystic duct insertion is a commonly encountered anatomy in such presentations)
Clinical Significance
- The triad of painless jaundice + palpable non-tender gallbladder + weight loss is highly suspicious for carcinoma of the head of the pancreas until proven otherwise
- The Courvoisier sign is uncommon even in pancreatic cancer (reported in <30% of cases); its absence does not exclude malignancy
- Important caveat: The sign can occasionally be falsely positive - a patient with stones in the gallbladder can still have a palpable gallbladder if the CBD is obstructed by malignancy simultaneously. As noted by Sleisenger & Fordtran: "Deep jaundice without pain, particularly with a palpable gallbladder (Courvoisier sign), suggests neoplastic obstruction of the bile duct, even when the patient has stones in the gallbladder."
- The absence of a palpable gallbladder does not exclude malignancy (the sign has low sensitivity)
Investigations to Follow
In a jaundiced patient with a positive Courvoisier sign:
- LFTs - raised bilirubin + ALP disproportionately (obstructive pattern); ALP rises faster and precedes bilirubin rise
- Ultrasound abdomen - first-line; confirms dilated intrahepatic and extrahepatic bile ducts; identifies the level of obstruction; may show pancreatic mass
- Contrast-enhanced CT scan (CECT) - preferred test if pancreatic head tumour suspected; assesses resectability (vascular encasement, metastases)
- MRCP / MRI - excellent for biliary anatomy and soft tissue characterisation
- EUS - superior for visualising the distal CBD and pancreatic head; can guide FNA biopsy
- ERCP - if cholangitis present, diagnostic uncertainty, or biliary decompression needed (brush cytology, biopsy, stenting); not routine pre-operatively in resectable disease (higher infective complications post-surgery)
- CA 19-9 - tumour marker; raised in pancreatic cancer (not specific or sensitive alone)
- Prothrombin time - check; prolonged obstructive jaundice causes vitamin K malabsorption; correct with Vitamin K before any procedure
Summary
| Courvoisier's Law | |
|---|---|
| Finding | Jaundice + palpable non-tender gallbladder |
| Implies | Malignant (neoplastic) obstruction of the CBD |
| Not due to | Gallstones (which cause gallbladder fibrosis → non-distensible) |
| Most common cause | Carcinoma of the head of the pancreas |
| First described | Ludwig Courvoisier, 1890 |
| Caveat | Low sensitivity; absence of palpable GB does not exclude malignancy |
Sources: Bailey & Love's Short Practice of Surgery (28th ed.), S. Das Manual on Clinical Surgery (13th ed.), Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Fischer's Mastery of Surgery (8th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.