How to Replace fulid in dengue patient in relation to HCT?
Reading File
Finding Sources
Finding Sources
Searching PubMed
dengue fever fluid resuscitation hematocrit management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the information needed for a comprehensive, well-illustrated answer. Let me compile it.
Fluid Replacement in Dengue Patients in Relation to Hematocrit (HCT)
The cornerstone of dengue management - especially Dengue Hemorrhagic Fever (DHF) and Dengue Shock Syndrome (DSS) - is HCT-guided fluid therapy. The hematocrit reflects the degree of plasma leakage (hemoconcentration) and guides both the initiation and titration of IV fluids.
Why HCT Matters in Dengue
Dengue causes increased vascular permeability leading to plasma leakage into extravascular spaces. This results in:
- Rising HCT = hemoconcentration = ongoing plasma leak
- Falling HCT (in a shocked patient not responding to fluids) = internal hemorrhage
- A rise of ≥20% from baseline HCT is a key diagnostic criterion for DHF (Grades I-IV)
"A rapidly decreasing platelet count in parallel with a rising haematocrit compared to the baseline is suggestive of progress to the plasma leakage/critical phase of the disease."
- Park's Textbook of Preventive and Social Medicine
WHO Grading of Dengue Severity (HCT as a Criterion)
| Grade | Clinical Features | HCT Finding |
|---|---|---|
| Dengue Fever (DF) | Fever + 2 symptoms (headache, rash, myalgia, leukopenia) | HCT rise 5-10% |
| DHF Grade I | DF + positive tourniquet test + plasma leakage | HCT rise ≥20% |
| DHF Grade II | Grade I + spontaneous bleeding (epistaxis, black stools) | HCT rise ≥20% |
| DHF Grade III | Grade II + circulatory failure (pulse pressure ≤20 mmHg) | HCT rise >20% |
| DHF Grade IV (DSS) | Profound shock, undetectable BP/pulse | HCT rise >20% |
- Park's Textbook of Preventive and Social Medicine, p. 295
Establishing Baseline HCT
"A haematocrit test in the early febrile phase establishes the patient's own baseline haematocrit... In the absence of the patient's baseline, age-specific population haematocrit levels could be used as a surrogate during the critical phase."
- Park's Textbook of Preventive and Social Medicine
Fluid Management Algorithm
1. Dengue Fever (No DHF) - Grades without plasma leakage
- Oral fluids preferred (ORS, fruit juice, electrolyte-containing fluids)
- Goal: adequate oral intake, urine output at least every 6 hours
- Stable HCT = can be managed outpatient
- IV fluids only needed if oral intake is inadequate
2. DHF Grades I & II - Moderate Disease (HCT rise ≥20%, hemorrhagic tendency)
Algorithm (Fig. 3 from Park's):
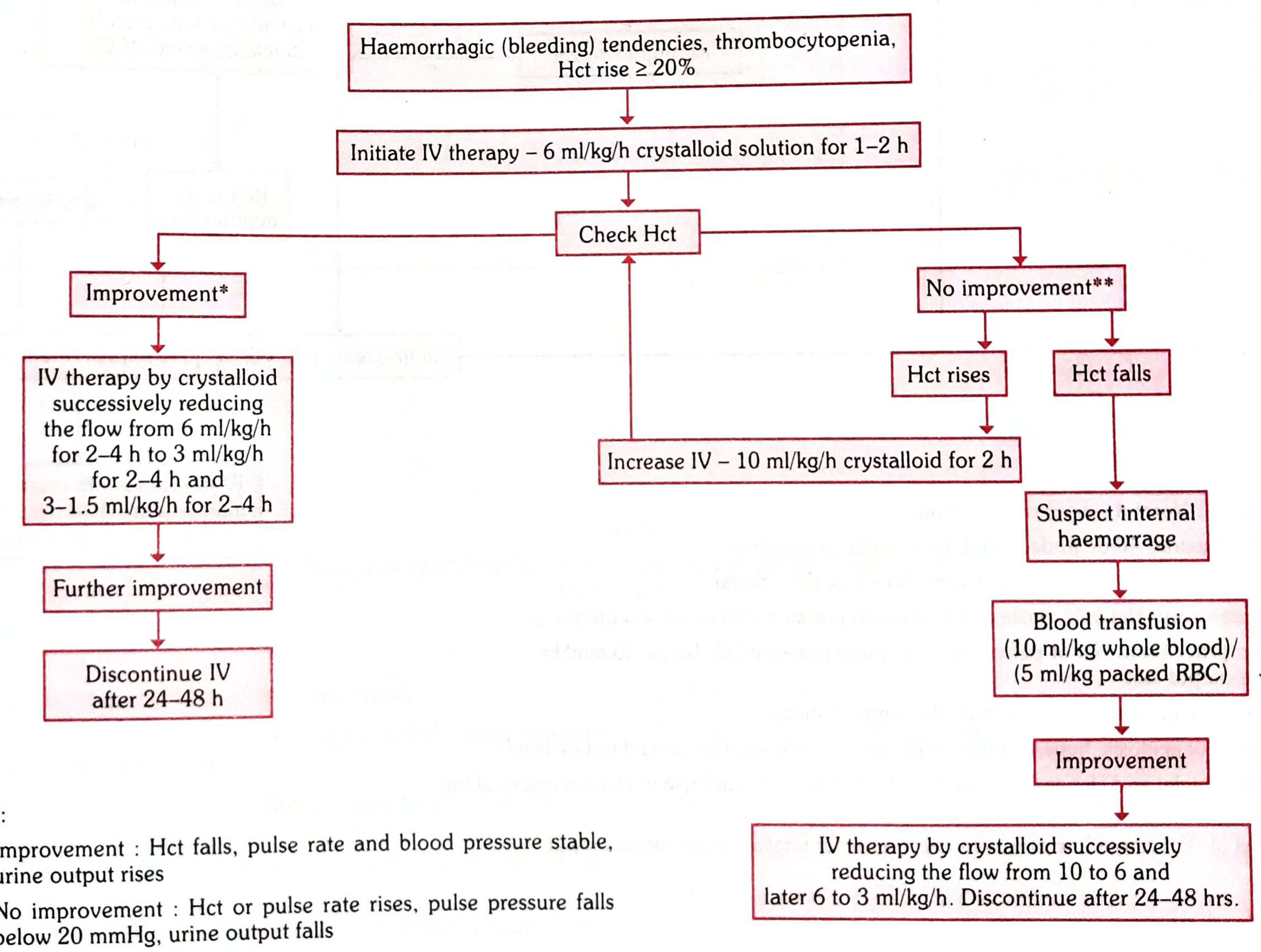
Step-by-step:
- Initiate IV crystalloid (Normal Saline or Ringer's Lactate) at 6 ml/kg/h for 1-2 hours
- Check HCT and assess response:
| Response | HCT Trend | Action |
|---|---|---|
| Improvement | HCT falls, stable vitals, urine output rises | Taper fluids: 6 → 3 → 1.5 ml/kg/h over 2-4 h each. Discontinue after 24-48 h |
| No improvement | HCT rises | Increase IV to 10 ml/kg/h crystalloid for 2 hours |
| No improvement | HCT falls | Suspect internal hemorrhage → Blood transfusion (10 ml/kg whole blood or 5 ml/kg packed RBC) → then step down as per improvement arm |
3. DHF Grades III & IV / DSS - Severe Disease (Compensated Shock)
Trigger: Pulse pressure ≤20 mmHg, SBP <90 mmHg, HCT >20% rise from baseline
Algorithm (Fig. 4 from Park's):
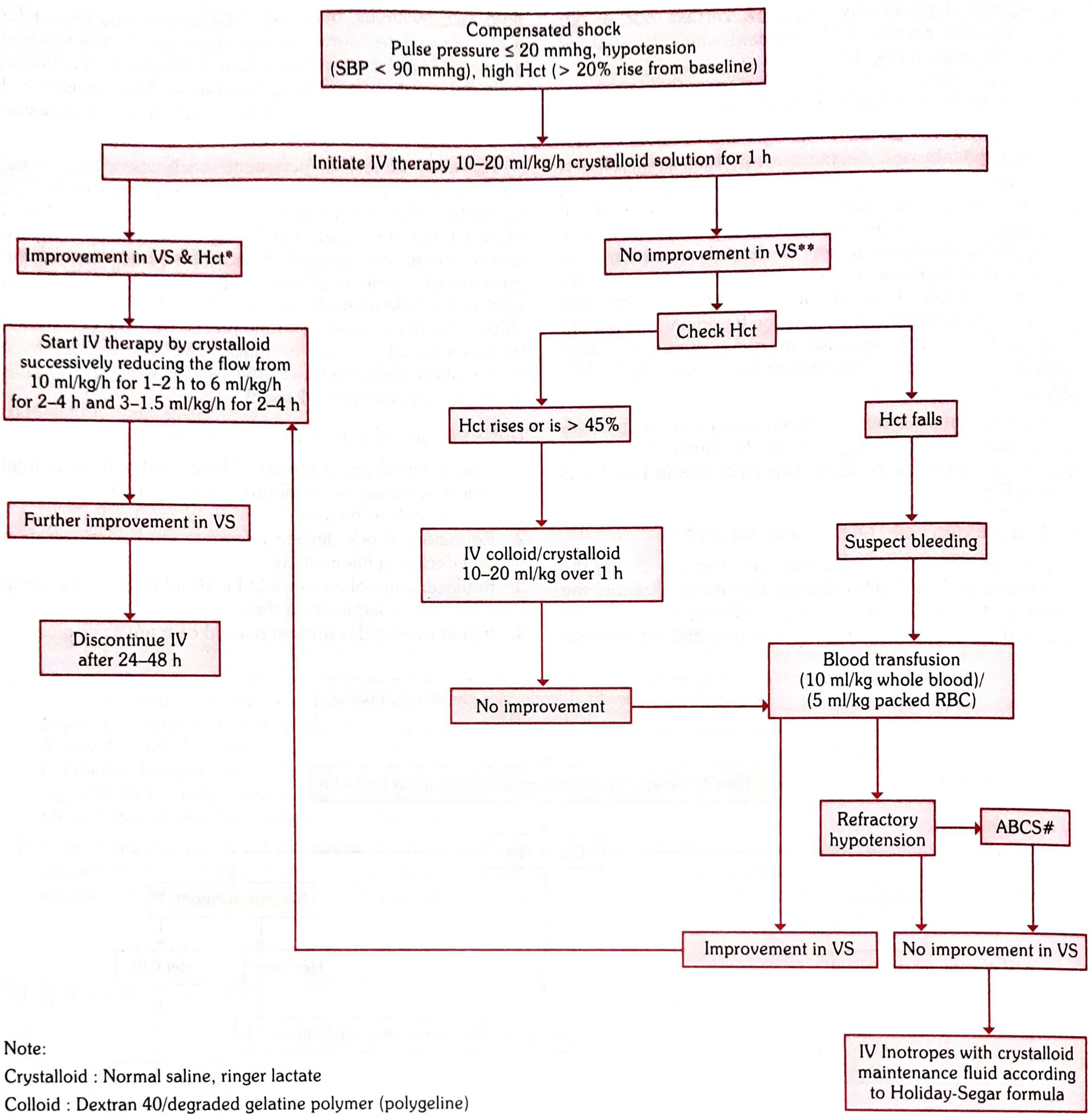
Step-by-step:
- Initiate IV crystalloid at 10-20 ml/kg/h for 1 hour (bolus)
- Reassess vitals AND HCT:
| Response | HCT Trend | Action |
|---|---|---|
| Improvement in vitals & HCT | HCT normalizing | Taper: 10 → 6 → 3 → 1.5 ml/kg/h. Discontinue after 24-48 h |
| No improvement | HCT rises or >45% | Switch to IV colloid or crystalloid 10-20 ml/kg over 1 h (e.g., Dextran 40, polygeline) |
| No improvement | HCT falls | Suspect bleeding → Blood transfusion (10 ml/kg whole blood / 5 ml/kg pRBC) |
| Refractory hypotension despite all above | - | Correct ABCS (Acidosis, Bleeding, Calcium/electrolytes, Sugar) → IV inotropes + maintenance fluids per Holliday-Segar formula |
Key Decision Points: When to Change Fluid Type
| Situation | Fluid Choice |
|---|---|
| Initial resuscitation (all grades) | Crystalloid (NS or Ringer's Lactate) |
| No improvement + HCT rising (shock) | Colloid (Dextran 40 or degraded gelatin polymer) |
| No improvement + HCT falling | Blood transfusion (suspect occult hemorrhage) |
| Fluid overload present | Packed RBCs (not whole blood) |
| Acidosis present | Avoid Ringer's Lactate (hyperosmolar or NS preferred) |
- Park's Textbook of Preventive and Social Medicine, p. 296
- Brenner and Rector's The Kidney: "Fluid therapy is key to dengue management... fluid lost due to capillary leakage must be replaced with IV crystalloid solutions"
Indications for Blood Transfusion
- Overt blood loss ≥10% of total blood volume
- Refractory shock despite adequate fluid administration and declining HCT
- Replacement volume: 10 ml/kg body weight at a time (with coagulogram)
- If fluid overload present: give packed RBCs instead of whole blood
Monitoring Parameters
Monitor every hour in DHF:
- HCT - the primary titration guide
- Vital signs (pulse rate, blood pressure, pulse pressure)
- Urine output (target: adequate output; decline = inadequate resuscitation)
- Signs of fluid overload (pleural effusion, ascites worsening, respiratory distress)
Signs of improvement:
- HCT falls toward baseline
- Pulse rate normalizes and BP stabilizes
- Urine output rises
Signs of no improvement / deterioration:
- HCT or pulse rate continues to rise
- Pulse pressure falls below 20 mmHg
- Urine output falls
Convalescent Phase - Avoiding Fluid Overload
During recovery, reabsorption of leaked plasma causes HCT to fall and circulating volume to increase. IV fluids should be tapered and stopped at 24-48 hours to prevent pulmonary edema and fluid overload.
"Close attention to fluid status has significantly reduced mortality from dengue, and aggressive fluid repletion has been needed to address significant loss of fluid volume."
- Goldman-Cecil Medicine
Summary Table
| Phase | HCT Change | Action |
|---|---|---|
| Febrile (no DHF) | Mild rise (5-10%) | Oral fluids; monitor |
| DHF I-II (plasma leak) | Rise ≥20% | IV crystalloid 6 ml/kg/h; titrate by HCT |
| DHF III-IV (shock) | Rise >20% | IV crystalloid 10-20 ml/kg/h bolus; colloid if no response |
| No response + HCT falls | Falling | Suspect hemorrhage; transfuse blood |
| Convalescent | HCT normalizes/falls | Taper and stop IV fluids; watch for overload |
This is a shared conversation. Sign in to Orris to start your own chat.