Pneumonia: Etiology Classification Diffetences between Lobar pneumonia & Bhronchopneumonia Morphology Lobar pneumonia: Gross and microscopic features Four stages of lobar pneumonia: Congestion Red hepatization Grey hepatization Resolution All microscopy of stages. Clinical Features Complications Laboratory diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from both Robbins textbooks. I have all I need to produce a thorough, well-structured answer with actual microscopy images. Let me now compile the complete response.
PNEUMONIA - Complete Pathology Notes
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Robbins & Kumar Basic Pathology (10e)
1. ETIOLOGY
Pneumonia results from failure of host defense mechanisms, invasion by microbial pathogens, or both. Predisposing host factors include:
- Loss of the cough reflex - coma, anesthesia, neuromuscular disorders, drugs, or chest pain
- Mucociliary dysfunction - cigarette smoke, inhalation of hot or corrosive gases, viral diseases, or genetic ciliary defects (immotile cilia syndrome)
- Secretion accumulation - cystic fibrosis, bronchial obstruction
- Impaired macrophage function - alcohol, tobacco smoke, anoxia, oxygen intoxication
- Pulmonary congestion and edema
- Innate/humoral immune defects - pyogenic bacterial infections; MYD88 mutations associated with pneumococcal pneumonia
- Cell-mediated immune defects - intracellular organisms, Pneumocystis jirovecii
Causal Organisms by Setting (Pneumonia Syndromes - Robbins Table 15.7)
| Setting | Key Organisms |
|---|---|
| Community-Acquired Acute | S. pneumoniae (most common), H. influenzae, M. catarrhalis, S. aureus, Legionella pneumophila, Klebsiella pneumoniae, Mycoplasma pneumoniae, Chlamydia spp., Coxiella burnetii (Q fever), Viruses (RSV, influenza A/B, adenovirus) |
| Healthcare-Associated | S. aureus (MSSA/MRSA), P. aeruginosa, S. pneumoniae |
| Hospital-Acquired | Gram-negative rods (Klebsiella, Serratia, E. coli, Pseudomonas), MRSA |
| Aspiration | Anaerobic oral flora (Bacteroides, Prevotella, Fusobacterium, Peptostreptococcus) ± aerobic bacteria |
| Chronic/Granulomatous | Mycobacterium tuberculosis, fungi (Histoplasma, Coccidioides) |
| Immunocompromised Host | CMV, Pneumocystis jirovecii, Aspergillus, Candida, atypical mycobacteria |
2. CLASSIFICATION
Pneumonia is classified by:
A. Etiologic Agent
- Bacterial, Viral, Fungal, Parasitic, Aspiration, Chemical
B. Clinical Setting (as in Table 15.7 above)
- Community-Acquired Acute Pneumonia
- Healthcare-Associated Pneumonia
- Hospital-Acquired (Nosocomial) Pneumonia
- Aspiration Pneumonia
- Chronic Pneumonia
- Necrotizing Pneumonia / Lung Abscess
- Pneumonia in the Immunocompromised Host
C. Anatomic Pattern (Morphologic Classification)
- Lobar Pneumonia - consolidation of an entire lobe or large portion
- Bronchopneumonia (Lobular) - patchy multifocal consolidation
- Interstitial Pneumonia - inflammation primarily in alveolar septa (typically viral)
3. DIFFERENCES: LOBAR PNEUMONIA vs. BRONCHOPNEUMONIA
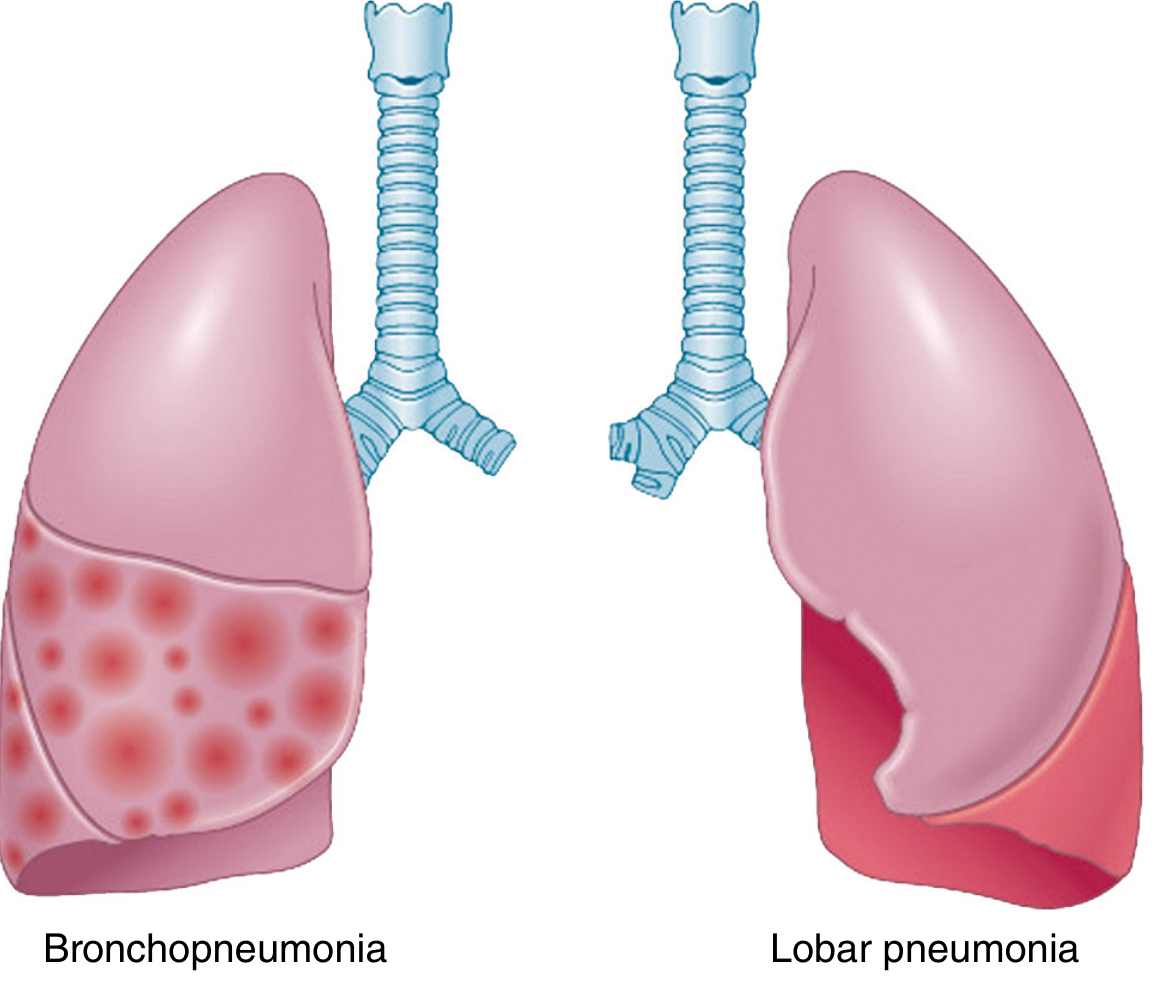
Fig. 15.28 - Comparison of bronchopneumonia and lobar pneumonia (Robbins, Cotran & Kumar)
| Feature | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Distribution | Consolidation of entire lobe or large lobar segment | Patchy, multifocal, lobular consolidation |
| Extent | Uniform, affects one (rarely more) lobe | Often multilobar, bilateral, basal |
| Common organisms | S. pneumoniae (most common), K. pneumoniae | S. aureus, H. influenzae (non-encapsulated), Gram-negatives |
| Typical patient | Previously healthy adult | Debilitated, elderly, post-viral infection |
| Gross appearance | Entire lobe uniformly firm, airless, liver-like | Multiple elevated, dry, gray-red to yellow patches |
| Histology | Diffuse alveolar exudate filling entire lobe; RBCs + neutrophils + fibrin | Neutrophilic exudate fills bronchi, bronchioles, and adjacent alveoli |
| Stages | Four classic stages (congestion, red/gray hepatization, resolution) | No classic staging; suppurative inflammation |
| Air bronchograms | Characteristic (visible on CXR/CT) | Less prominent |
| Volume loss | Minimal in early stages | Variable |
| Pleuritis | Common (peripheral spread) | Less common |
| Prognosis | Generally better in healthy adults | Worse due to underlying debility |
4. MORPHOLOGY OF LOBAR PNEUMONIA
Gross Features
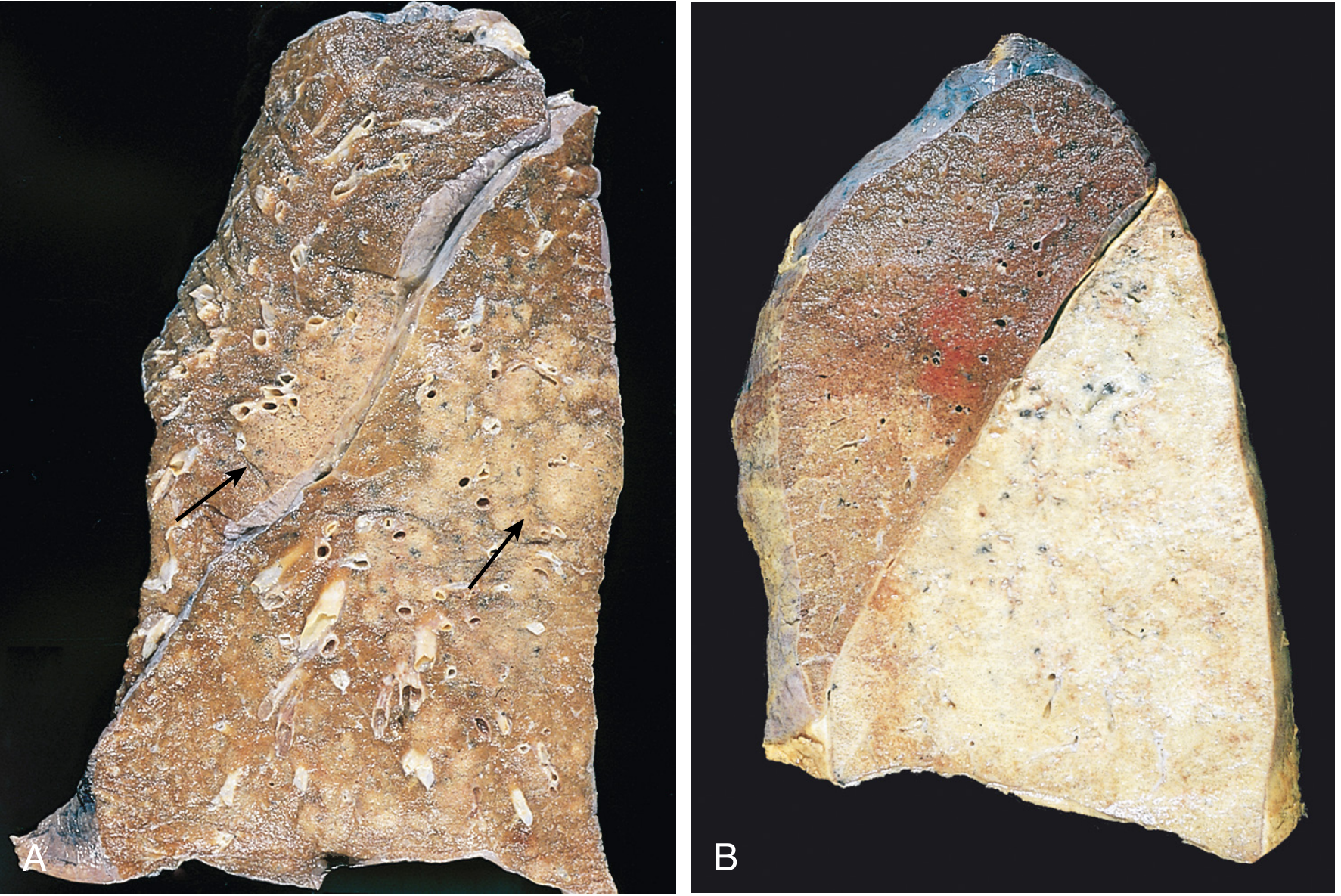
Fig. 15.29 - (A) Bronchopneumonia - patchy consolidation (arrows). (B) Lobar pneumonia - gray hepatization, lower lobe uniformly consolidated. (Robbins, Cotran & Kumar)
FOUR STAGES OF LOBAR PNEUMONIA
Stage 1: CONGESTION (Day 1-2)
Gross:
- Lung is heavy, boggy, and red
- The cut surface exudes blood-stained fluid
Microscopy:
- Vascular engorgement (dilated, congested capillaries)
- Intraalveolar edema fluid with few neutrophils
- Numerous bacteria may be present in alveolar spaces
- Alveolar walls intact
Stage 2: RED HEPATIZATION (Day 3-4)
Gross:
- Lobe is red, firm, and airless
- Liver-like consistency (hence "hepatization")
- Cut surface: dry, granular, red
Microscopy:
- Massive confluent exudation filling alveolar spaces
- Alveoli packed with neutrophils + red blood cells + fibrin
- Fibrin strands may cross alveolar walls via pores of Kohn
- Capillaries compressed by exudate
Stage 3: GRAY HEPATIZATION (Day 5-7)
Gross:
- Lobe becomes gray-brown (color change as RBCs disintegrate)
- Still firm, liver-like consistency
- Dry, granular cut surface
Microscopy:
- Progressive disintegration of red cells (RBCs lysed - color change)
- Fibrinopurulent exudate persists in alveoli
- Predominantly neutrophils and fibrin remain (no intact RBCs)
- Alveolar walls still intact
Stage 4: RESOLUTION (Day 8 onwards)
Gross:
- Lung softens as exudate liquefies
- Returns toward normal aeration
- If uncomplicated, architecture restored
Microscopy:
- Enzymatic digestion of the fibrinopurulent exudate
- Produces granular, semifluid debris
- Debris is: resorbed, ingested by macrophages, expectorated, or organized by fibroblasts
- Alveolar macrophages prominent
- Restoration of normal architecture
KEY MICROSCOPY IMAGES - ALL STAGES
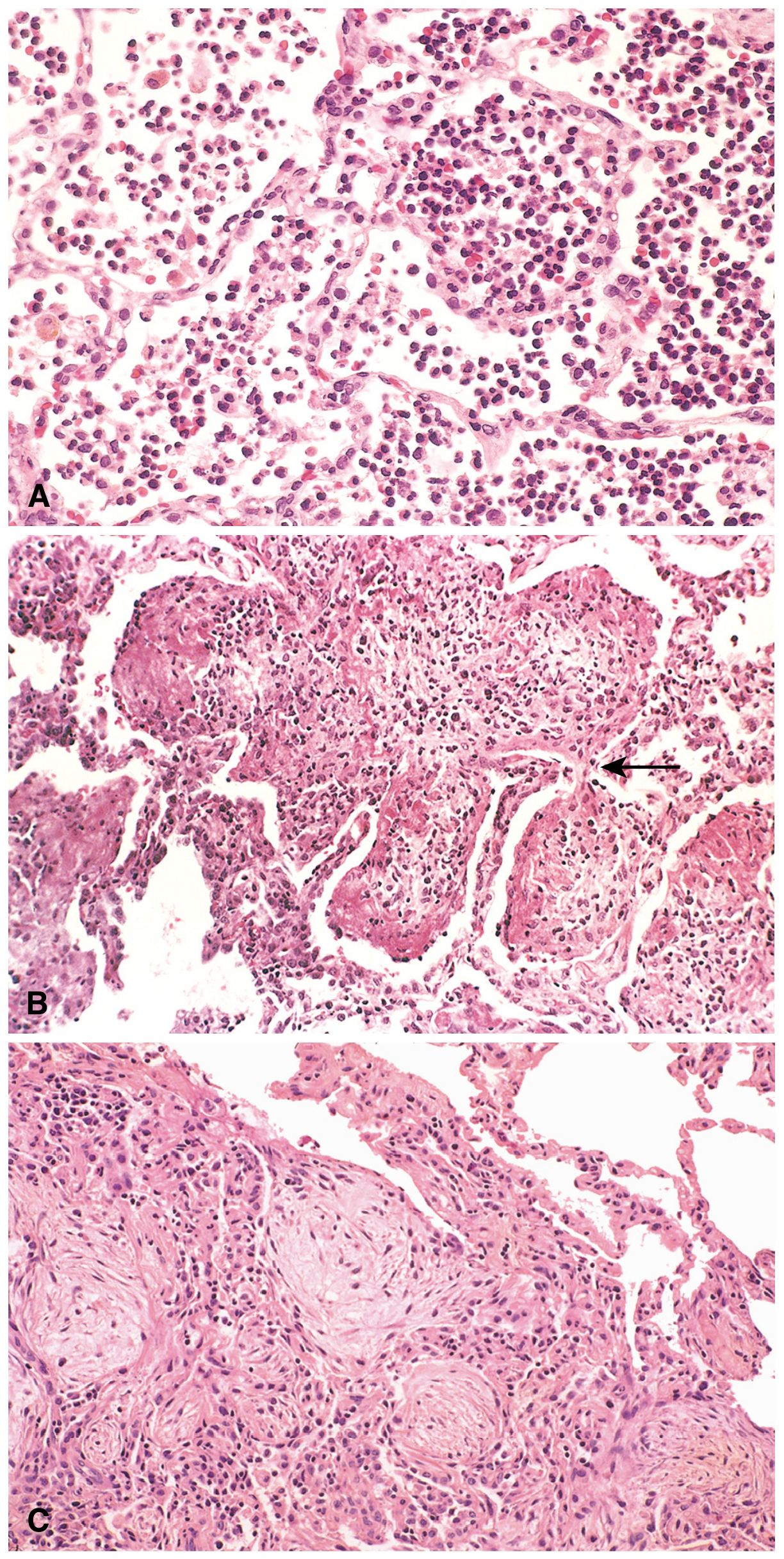
Fig. 15.30 - Stages of bacterial pneumonia.
- (A) Acute pneumonia / Red Hepatization: Alveoli are massively filled with neutrophils, erythrocytes, and fibrin strands.
- (B) Gray Hepatization: Fibrinopurulent exudate with progressive RBC disintegration; arrow indicates fibrin.
- (C) Resolution: Macrophage-dominated phase, debris being cleared, architectural framework being restored.
(Robbins, Cotran & Kumar Pathologic Basis of Disease)
5. CLINICAL FEATURES
- Abrupt onset of high fever with shaking chills
- Cough productive of mucopurulent sputum
- Occasional hemoptysis
- Pleuritic chest pain and pleural friction rub (when pleuritis is present)
- Dyspnea and tachypnea
- Radiologic findings:
- Lobar pneumonia: entire lobe radiopaque; air bronchograms visible on CT
- Bronchopneumonia: patchy focal opacities (multifocal)
- Response to antibiotics: with effective treatment, patients become afebrile within 48-72 hours
- In viral pneumonia: respiratory distress is out of proportion to clinical and radiologic signs; inflammation predominantly in alveolar septa
6. COMPLICATIONS
- Tissue destruction and necrosis → lung abscess formation
- Spread to pleural cavity → fibrinopurulent pleuritis → empyema (pus in pleural space)
- Bacteremic dissemination (hematogenous spread) to:
- Heart valves → endocarditis
- Pericardium → pericarditis
- Brain → meningitis / brain abscess
- Kidneys, spleen, joints → suppurative arthritis, abscesses
- Organization of exudate → carnification (fibrotic lung, failure to resolve)
- Pleural adhesions (from organized fibrinous pleuritis)
- Septicemia and septic shock
Note: Fewer than 10% of hospitalized pneumonia patients now die, and death is usually from a complication (empyema, meningitis, endocarditis, pericarditis) or an underlying predisposing condition (debility, chronic alcoholism).
7. LABORATORY DIAGNOSIS
Sputum Analysis
- Gram stain: Most important initial step
- S. pneumoniae: gram-positive lancet-shaped diplococci; abundant neutrophils
- S. aureus: gram-positive cocci in clusters
- Klebsiella: gram-negative rods (mucoid capsule)
- Caveat: S. pneumoniae is normal flora in ~20% of adults → false positives possible
- Sputum culture and sensitivity: identifies organism and guides antibiotic therapy
Blood Cultures
- More specific but less sensitive than sputum (only 20-30% positive in early illness)
- Positive blood cultures confirm bacteremia and guide targeted therapy
Other Tests
- CBC: Leukocytosis with neutrophilia (bacterial); lymphocytosis (viral/atypical)
- Chest X-ray / CT: Confirms diagnosis, delineates extent; air bronchograms in lobar pattern; patchy infiltrates in bronchopneumonia
- Urinary antigen tests: Legionella pneumophila (serogroup 1), S. pneumoniae
- Serology: Cold agglutinins (Mycoplasma), specific IgM/IgG titers for atypicals
- Bronchoscopy with BAL (bronchoalveolar lavage): For immunocompromised or non-responding patients
- PCR / Molecular testing: Increasingly used for viral and atypical pathogens (influenza, SARS-CoV-2, Mycoplasma, Legionella)
- Pleural fluid analysis: If empyema suspected; Light's criteria for exudate; Gram stain and culture
Sources: Robbins & Kumar Basic Pathology (Robbins Pathology), p. 470 | Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 660-664 | Fishman's Pulmonary Diseases and Disorders
Need this in a easy language understanding
PNEUMONIA - Easy Language Notes 🫁
1. WHAT IS PNEUMONIA?
Think of your lungs like a sponge full of tiny air pockets (alveoli). Normally, you breathe air in and out freely. In pneumonia, germs infect the lung and fill those air pockets with fluid, pus, and dead cells instead of air. The lung becomes solid - it can no longer do its job of exchanging oxygen.
2. ETIOLOGY (Why does pneumonia happen?)
Your body normally protects the lungs. Pneumonia happens when these defenses fail:
| Defense Mechanism | How it Fails |
|---|---|
| Cough reflex (clears germs out) | Fails in coma, alcohol intoxication, after anesthesia |
| Tiny hairs (cilia) that sweep germs out | Damaged by cigarette smoke, viral infections |
| Mucus system that traps germs | Blocked in cystic fibrosis, bronchial obstruction |
| Macrophages (lung's own security guards) | Weakened by alcohol, smoking, lack of oxygen |
| Immune system | Weakened in HIV, diabetes, old age, steroid use |
Think of it like a city's security system failing - once one barrier breaks, invaders (bacteria/viruses) get in easily.
3. CLASSIFICATION (Types of Pneumonia)
By WHERE you caught it:
| Type | Where Caught | Common Bugs |
|---|---|---|
| Community-Acquired | Outside hospital, normal life | S. pneumoniae (most common), Mycoplasma |
| Hospital-Acquired | While admitted in hospital | MRSA, Pseudomonas, Klebsiella |
| Aspiration | Food/vomit accidentally goes into lungs | Mouth bacteria (anaerobes) |
| Immunocompromised | In patients with weak immunity | Pneumocystis, fungi, CMV |
By PATTERN of lung involvement:
- Lobar Pneumonia - entire lobe affected (like one whole room flooded)
- Bronchopneumonia - multiple small patches affected (like several puddles scattered)
- Interstitial Pneumonia - the walls between air sacs inflamed (usually viral)
4. LOBAR vs BRONCHOPNEUMONIA - Key Differences
Left = Bronchopneumonia (patchy spots). Right = Lobar pneumonia (entire lower lobe solid red).
| Feature | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Imagine it as... | One entire room flooded | Several small puddles in many rooms |
| Who gets it | Healthy young/middle-aged adults | Elderly, debilitated, post-viral illness |
| Area affected | Whole lobe or large part of it | Patchy, bilateral, lower lobes mostly |
| Main bug | Streptococcus pneumoniae | Staph aureus, H. influenzae |
| Gross appearance | Uniform, firm, liver-like | Multiple raised, yellowish-gray patches |
| Goes through stages? | YES - 4 classic stages | No clear staging; just suppurative (pus-filled) |
| Pleuritis (chest pain) | Common | Less common |
| CXR finding | Whole lobe white/opaque | Patchy white spots |
5. MORPHOLOGY OF LOBAR PNEUMONIA
Gross Features (what you see with naked eye):
The lobe goes through a dramatic transformation - from normal spongy pink tissue to something that looks and feels like a piece of liver.
THE 4 STAGES - Explained Simply
🔴 STAGE 1: CONGESTION ("The Alarm Stage") - Day 1-2
Simple Explanation: Germs have just arrived. Blood vessels dilate, fluid leaks in - like a fire alarm going off and the fire trucks rushing in.
GROSS:
- Lung is heavy, red, and boggy (like a wet sponge)
- Oozes blood-stained fluid when cut
MICROSCOPY:
- Blood vessels are dilated and engorged (full of blood)
- Alveoli have edema fluid + very few neutrophils
- Lots of bacteria visible
- Alveolar walls still intact and normal
🩸 STAGE 2: RED HEPATIZATION ("The Battle Stage") - Day 3-4
Simple Explanation: Army (neutrophils) has fully arrived. Massive battle happening. Alveoli completely packed with cells - the lung is now solid like a liver. "Hepatization" literally means "looks like liver."
GROSS:
- Lung is red, firm, and completely airless
- Feels and looks like a piece of liver when cut
- Cut surface is dry and granular
MICROSCOPY:
- Alveoli PACKED with:
- 🔴 Red blood cells (RBCs)
- 🟡 Neutrophils (white cells)
- 🕸️ Fibrin strands (like a net)
- Capillaries compressed by all this exudate
- No air spaces visible
⚪ STAGE 3: GRAY HEPATIZATION ("The Cleanup Begins") - Day 5-7
Simple Explanation: The RBCs break apart (no more red color), but the pus and fibrin are still there. Lung turns gray-brown. Still feels like liver but is now gray colored.
GROSS:
- Lung turns gray-brown in color
- Still firm (liver-like) but now grayish
- Dry, granular surface
MICROSCOPY:
- RBCs have disintegrated (that's why gray, not red)
- Fibrin + Neutrophils (pus) still fill the alveoli = fibrinopurulent exudate
- Alveolar walls still intact
- No bacteria being killed → gradually clearing
✅ STAGE 4: RESOLUTION ("The Healing Stage") - Day 8 onwards
Simple Explanation: The mess is cleaned up. Enzymes break down the exudate. Macrophages (the janitors) come and mop everything up. Lung returns to normal.
GROSS:
- Lung softens as the solid exudate liquefies
- Air slowly returns to alveoli
- Normal spongy texture returning
MICROSCOPY:
- Enzymes digest the fibrinopurulent exudate → becomes granular, semifluid debris
- This debris is:
- Resorbed into blood
- Eaten by macrophages (the janitors!)
- Coughed out (expectorated)
- Or organized by fibroblasts (scar formation if healing goes wrong)
- Macrophages are the dominant cell in this stage
- Architecture of lung gradually restores
Summary of All 4 Stages at a Glance
| Stage | Days | Color | Consistency | Key Microscopy Cells |
|---|---|---|---|---|
| Congestion | 1-2 | Red | Boggy, wet | Edema fluid + few neutrophils + bacteria |
| Red Hepatization | 3-4 | Red | Firm (liver-like) | RBCs + neutrophils + fibrin |
| Gray Hepatization | 5-7 | Gray-brown | Firm (liver-like) | Neutrophils + fibrin (no RBCs) |
| Resolution | 8+ | Normal | Soft, returning normal | Macrophages + debris clearing |
Microscopy Images - All Stages
(A) = Red Hepatization - Look at how densely packed the alveoli are - dark blue dots = neutrophils, pink = RBCs and fibrin. No air space at all.
(B) = Gray Hepatization - Still packed with cells but fewer intact RBCs. Fibrin strands visible (arrow). Grayish appearance begins.
(C) = Resolution - Alveoli starting to clear. Macrophages (larger cells) dominating. Loose, pale debris visible. Air spaces beginning to reappear.
(A) Bronchopneumonia - Patchy yellow-gray areas (arrows) scattered throughout the lung. Rest of lung is normal.
(B) Lobar pneumonia (Gray Hepatization) - Entire lower lobe is uniformly solid/grayish-white. Clear line between normal upper lobe and consolidated lower lobe.
6. CLINICAL FEATURES (What the patient looks like)
Think of typical lobar pneumonia as a dramatic, sudden illness:
| Symptom | Why it happens |
|---|---|
| High fever + shaking chills | Immune response to bacteria |
| Cough with yellow/green sputum | Pus being cleared from lungs |
| Hemoptysis (blood in sputum) | Blood vessel damage |
| Pleuritic chest pain (sharp, worse on breathing) | Inflammation spreads to pleura (lung lining) |
| Pleural friction rub (heard with stethoscope) | Roughened inflamed pleural surfaces rubbing |
| Breathlessness | Alveoli filled with fluid = less oxygen transfer |
| Whole lobe white on X-ray | Lobar pneumonia = entire lobe opaque |
| Patchy opacities on X-ray | Bronchopneumonia = scattered white patches |
Good news: With antibiotics, patients become fever-free within 48-72 hours!
7. COMPLICATIONS (What can go wrong)
Think of pneumonia spreading outward like ripples in a pond:
Lung infection
↓
Spreads to pleura → EMPYEMA (pus in chest cavity)
↓
Destroys lung tissue → LUNG ABSCESS
↓
Bacteria enter blood → BACTEREMIA
↓
Spreads to heart → ENDOCARDITIS / PERICARDITIS
Spreads to brain → MENINGITIS / BRAIN ABSCESS
Spreads to joints → SEPTIC ARTHRITIS
↓
Lung fails to resolve → CARNIFICATION (scar tissue replaces lung)
| Complication | Simple Explanation |
|---|---|
| Lung abscess | Pus pocket forms in destroyed lung tissue |
| Empyema | Pus collects between lung and chest wall |
| Endocarditis | Bacteria reach heart valves via blood |
| Meningitis | Bacteria reach brain covering via blood |
| Carnification | Exudate organizes into scar instead of resolving |
| Pleural adhesions | Inflamed pleura sticks together permanently |
8. LABORATORY DIAGNOSIS (How we confirm it)
Step-by-Step Approach:
1. Sputum Gram Stain (First and fastest test)
- Look under microscope at stained sputum
- S. pneumoniae = paired oval bacteria (lancet-shaped diplococci), gram-positive (purple)
- Lots of neutrophils = active bacterial infection
- ⚠️ S. pneumoniae lives normally in 20% of healthy people's throats, so a positive stain doesn't always mean disease
2. Sputum Culture
- Grow the bacteria to identify exact species and which antibiotics will kill it
- Takes 24-48 hours but tells you the exact bug
3. Blood Culture
- Only 20-30% positive in early illness
- More specific than sputum (if positive, definitely the bug causing illness)
- Important for severe/hospitalized cases
4. CBC (Blood Count)
- Bacterial pneumonia = high WBC (leukocytosis) with lots of neutrophils
- Viral pneumonia = high lymphocytes instead
- Simple, quick clue to type of infection
5. Chest X-Ray / CT Scan
- Lobar pneumonia: whole lobe white (opaque)
- Bronchopneumonia: scattered white patches
- CT shows air bronchograms in lobar pneumonia (airways visible within the solid lung)
6. Urine Antigen Tests
- For Legionella and Streptococcus pneumoniae
- Quick, non-invasive
7. PCR / Molecular Tests
- For viruses (influenza, COVID-19) and atypical bacteria (Mycoplasma, Legionella)
- Fast and very accurate
8. Bronchoscopy + BAL
- Camera into lungs, wash and collect fluid
- Used when patient isn't responding to treatment or is immunocompromised
- Best test for unusual organisms
Quick Revision Summary
PNEUMONIA = Lung alveoli filled with exudate instead of air
TYPES: Lobar (whole lobe) vs Bronchopneumonia (patchy)
STAGES of Lobar:
1. Congestion → Red, boggy, few neutrophils, bacteria
2. Red Hepatization → Red, firm, RBCs + neutrophils + fibrin
3. Gray Hepatization → Gray, firm, neutrophils + fibrin (RBCs gone)
4. Resolution → Macrophages clear debris, normal returns
SYMPTOMS: Fever, chills, cough, chest pain, breathlessness
COMPLICATIONS: Abscess, Empyema, Endocarditis, Meningitis
LAB: Sputum Gram stain + culture, Blood culture, CXR, CBC
This is a shared conversation. Sign in to Orris to start your own chat.